
Remember me




A total of 78 patients were included in the study (Table 1). The mean age (SD) was 48.5 (13.8) years and 61.5% (48/78) of patients were male. In terms of body mass index (BMI) 28.2% (22/78) of the patients were overweight and 41% (32/78) were obese. Active smoking was reported in 73.1% (57/78) of cases. Relevant comorbidities were present in 31 patients (39.8%), including 11 patients (14.1%) with concomitant psoriasis and two (2.6%) with psoriatic arthritis. The mean age at disease onset was 26.4 (12.8) years, and the mean disease duration was 22.0 (12.8) years.
Table 1 Basal characteristics of the sample (N = 78)At baseline, the mean abscesses and nodules (AN) count was 6.2 (6.2), with an average of 2.1 abscesses (2.5) and 4.0 nodules (2.7). The mean monthly flare frequency was 2.0 (1.0) and the mean pain score on the VAS was 7.4 (2.1).
In terms of disease severity, 60.3% (47/78) of patients were classified as Hurley stage III, 39.7% (31/78) as stage II, with a mean of 4.8 (1.5) affected anatomical areas. On the basis of the clinical phenotype (Martorell classification), 64.1% (50/78) of patients had the inflammatory subtype, 10.3% (8/78) had the follicular subtype, and 25.6% (20/78) presented with a mixed form. According to the anatomical phenotype (Molina-Leyva classification), 82.1% (64/78) were classified as progressor forms, 15.4% (12/78) as lower forms, and 2.6% (2/78) as upper forms.
A total of 91.0% (71/78) of patients had received prior adalimumab therapy, and 43.6% (34/78) had previously been treated with secukinumab. The mean (SD) number of prior systemic immunomodulators used was 1.8 (1.4).
Most of the patients, 66.7% (52/78), received the approved dosing regimen for HS, consisting of bimekizumab 320 mg (administered as two subcutaneous injections of 160 mg or one injection of 320 mg) every 2 weeks until week 16, followed by 320 mg every 4 weeks thereafter. The remaining patients received psoriasis dosing, 19.2% (15/78); 320 mg every 4 weeks, 2.6% (2/78); and 320 mg every 2 weeks, 11.5% (9/78).
EffectivenessIHS4 Responder Rates (IHS4-55/75/90/100) and Combined TreatmentFig. 1
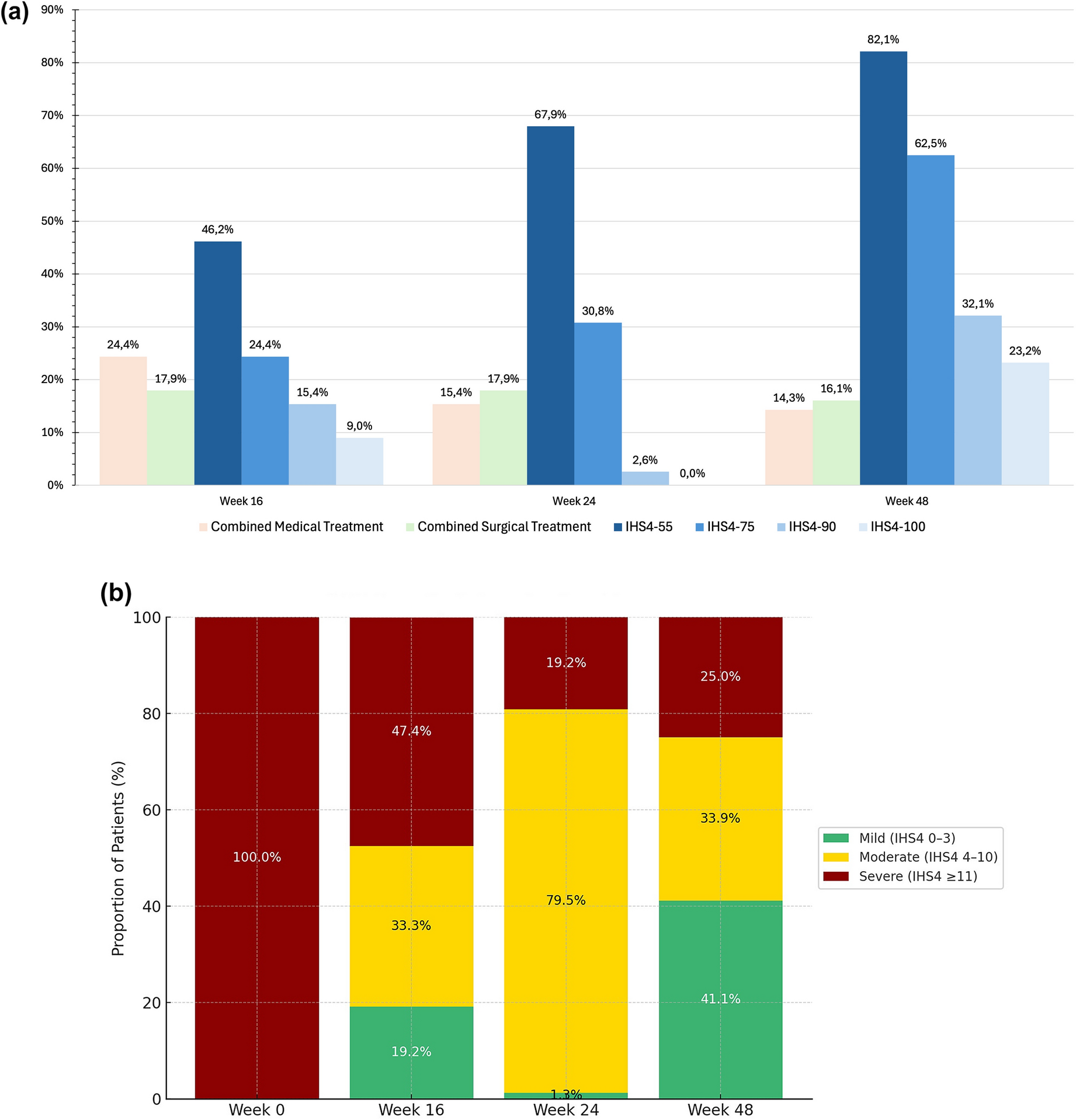
Effectiveness* of bimekizumab over time, as observed analysis. a International Hidradenitis Suppurativa Severity Score System (IHS4) 55/75/90/100 response rates. b Evolution of IHS4 severity categories over time. *Proportional distribution of patients according to IHS4-defined disease severity (mild, IHS4 0–3; moderate, IHS4 4–10; severe, IHS4 ≥ 11) at baseline and follow-up visits (weeks 16, 24, and 48)
At week 16, 46.2% (36/78) of patients achieved an IHS4-55 response,24.3% (19/78) achieved an IHS4-75 response, 15.4% (12/78) an IHS4-90 response, and 9.0% (7/78) an IHS4-100 response (Fig. 1a). At this timepoint, 24.4% (19/78) of patients received concomitant medical treatment and 17.9% (14/78) underwent surgical procedures. At week 24, 67.9% (53/78) of patients reached an IHS4-55, 30.7% (24/78) an IHS4-75, and 2.5% (2/78) an IHS4-90 response. No patients reached a complete response (IHS4-100). At this visit, 15.4% (12/78) received concomitant medical treatment and 17.9% (14/78) underwent surgery. At week 48, 82.1% (46/56) of patients achieved an IHS4-55, 62.5% (35/56) an IHS4-75, 32,1% (18/56) an IHS4-90, and 23.2% (13/56) an IHS4-100 response. Combined treatment was administered in 14.3% (8/56) as medical therapy and in 16.1% (9/56) as surgical intervention. Overall, combined treatment was performed in 38.9% (113/290) of visits.
The mean IHS4 score decreased progressively throughout the follow-up period. The mean (SD) baseline score was 24.2 (13.4), dropping to 14.9 (10.1) at week 16, 11.4 (8.4) at week 24, and 7.5 (6.3) at week 48. This reduction was statistically significant (p < 0.001).
Categorical Change in IHS4 Disease SeverityA categorical shift was observed in the distribution of disease severity (mild [IHS4 0–3], moderate [4–10] and severe [≥ 11]) over time (Fig. 1b). At baseline, 88.5% (69/78) of patients presented with severe disease. By week 16, this proportion had fallen to 47.4% (37/78), and by week 48, only 25.0% (10/39) remained in the severe category, while 41.1% (16/39) had achieved a mild level of disease activity. Among patients in the mild category, complete clinical remission (IHS4 = 0) was recorded in 11.5% (9/78) at week 16 and 23.2% (13/56) at week 48. No patients reached IHS4 = 0 at week 24. This analysis allowed for a clear visualization of how patients shifted between severity categories over time according to IHS4 thresholds.
Pain ReductionPatient-reported pain, measured using the VAS, showed a notable decrease over time. The mean (SD) baseline VAS score was 7.4 (2.1), decreasing to 4.3 (2.5) at week 16, 3.1 (2.5) at week 24, and 2.7 (2.7) at week 48 (p < 0.001) (Fig. 2a).
Fig. 2
Impact of bimekizumab on patient-reported outcomes and lesion burden, as observed analysis. a Mean pain Visual Analog Scale (VAS) score over time. b Mean number of draining tunnels over time. c Monthly flare frequency throughout the study
Number of Draining TunnelsThe number of draining tunnels also decreased progressively over time: from a mean (SD) of 3.3 (2.3) at baseline to 1.9 (1.9) at week 16, 1.4 (1.8) at week 24, and 1.0 (1.7) at week 48. This reduction was statistically significant (p < 0.001) (Fig. 2b).
Monthly FlaresThe frequency of flares per month decreased from a mean (SD) of 2.0 (0.6) at baseline to 0.8 (0.4) at week 16, 0.6 (0.3) at week 24 and 0.5 (0.3) at week 48. This reduction was statistically significant (p < 0.001) (Fig. 2c).
Predictors of IHS4-55 and IHS4-100 Response at Week 48No statistically significant associations were identified between achieving an IHS4-55 response at week 48 and key demographic or clinical variables, including sex, age, BMI, active smoking status, disease duration prior to bimekizumab initiation, clinical phenotype (Martorell classification), anatomical phenotype (Molina-Leyva classification), dosing regimen, basal IHS4, baseline speed of progression, or Hurley stage (Table 2).
Table 2 Determinants of IHS4-55 response at week 48A significant inverse correlation was observed between the number of affected anatomical areas and the likelihood of achieving IHS4-55 response (β = − 0.485, SD 0.243; p = 0.046), indicating lower response rates in patients with more extensive disease involvement.
Other factors, including Hurley stage II vs. III 80.95% (17/56) vs. 82.86% (29/56) (p = 0.85), prior exposure to systemic immunomodulators (β = − 0.441, SD 0.271; p = 0.1038), previous treatment with secukinumab (28.6% vs. 11.4%; p = 0.1517), baseline IHS4 score (β = − 0.0019, SD 0.026; p = 0.9389), history of systemic antibiotic therapy (23.1% vs. 16.3%; p = 0.5749), and prior surgical interventions (26.3% vs. 13.5%; p = 0.2363), were not significantly associated with treatment response.
An exploratory analysis was performed to identify potential factors associated with IHS4-100 achievers (super responders) at week 48. Univariate analysis included all the variables shown in Table 2, showing a significant inverse association with baseline IHS4, speed of progression, and progressor phenotype vs. primary forms (upper, lower, atypical). A binomial multivariate logistic regression model was performed showing that (data shown as β coefficient and SD) a lower speed of progression − 2.49 (1.15) p = 0.002 and the presence of a primary phenotype (upper, lower, or atypical vs. progressor) 0.82 (0.45) p = 0.059 were associated with achieving IHS4-100, with independence from baseline IHS4 value p = 0.77.
Hurley stage III is a well-established factor related to lower response to biologic drugs [12, 25]. No differences in effectiveness were observed between Hurley stage II and III in our cohort. Consequently, we performed exploratory sub-analysis to explore if the therapeutic approach was different according to this clinical feature. Analysis revealed that Hurley stage III was associated with more frequent use of cooling or combined treatment at baseline, and more use of combined antibiotic and surgical treatment at any time during follow-up (Table 3, Fig. 3). Specifically, systemic antibiotics were administered at any time in 31.9%% (15/47) of Hurley III patients vs. 12.9% (4/31) in Hurley II (p = 0.0474), and systemic corticosteroids in 12.77% (6/47) vs. 0% (0/31), respectively (p = 0.0418). Surgical procedures were also more commonly performed in Hurley III patients, with 42.55% (20/47) undergoing surgery vs. 19.35% (6/31) in Hurley II (p = 0.0283).
Table 3 Differences in therapeutic approach by Hurley stageFig. 3
Differences in therapeutic approach by Hurley stage
Safety and Treatment DiscontinuationDuring the follow-up period, a total of 34 adverse events were reported among the 78 patients (34/78, 43.6%). The most common were mucocutaneous candidiasis, 26.9% (21/78), with oral candidiasis (11/78, 14.1%) being the most frequent presentation; followed by eczematous reactions, 8.9% (7/78), with eyelid eczema being the most common presentation, 57.1% (4/7) (Fig. 4). Three patients (3.8%) presented psoriasiform reactions. Isolated cases (1/78, 1.3%) each included vulvovaginal candidiasis, angular cheilitis, oral aphthosis, fatigue, worsening of fibromyalgia, diarrhea after injection, acute cholangitis, and onset of Crohn’s disease in a patient without familiar or personal history of inflammatory bowel disease.
Fig. 4
Main adverse events and reasons for discontinuation during bimekizumab treatment
A total of eight patients (8/78, 10.3%) discontinued treatment, mainly because of a lack of efficacy (5/78, 6.4%), with discontinuations occurring at weeks 24, 34, and 48. Other reasons for withdrawal included the onset of Crohn’s disease (1/78, 1.3%, week 24), paradoxical psoriasis (1/78, 1.3%, week 40), and non-specified reasons (1/78, 1.3%, week 32).
Comments (0)