
Remember me
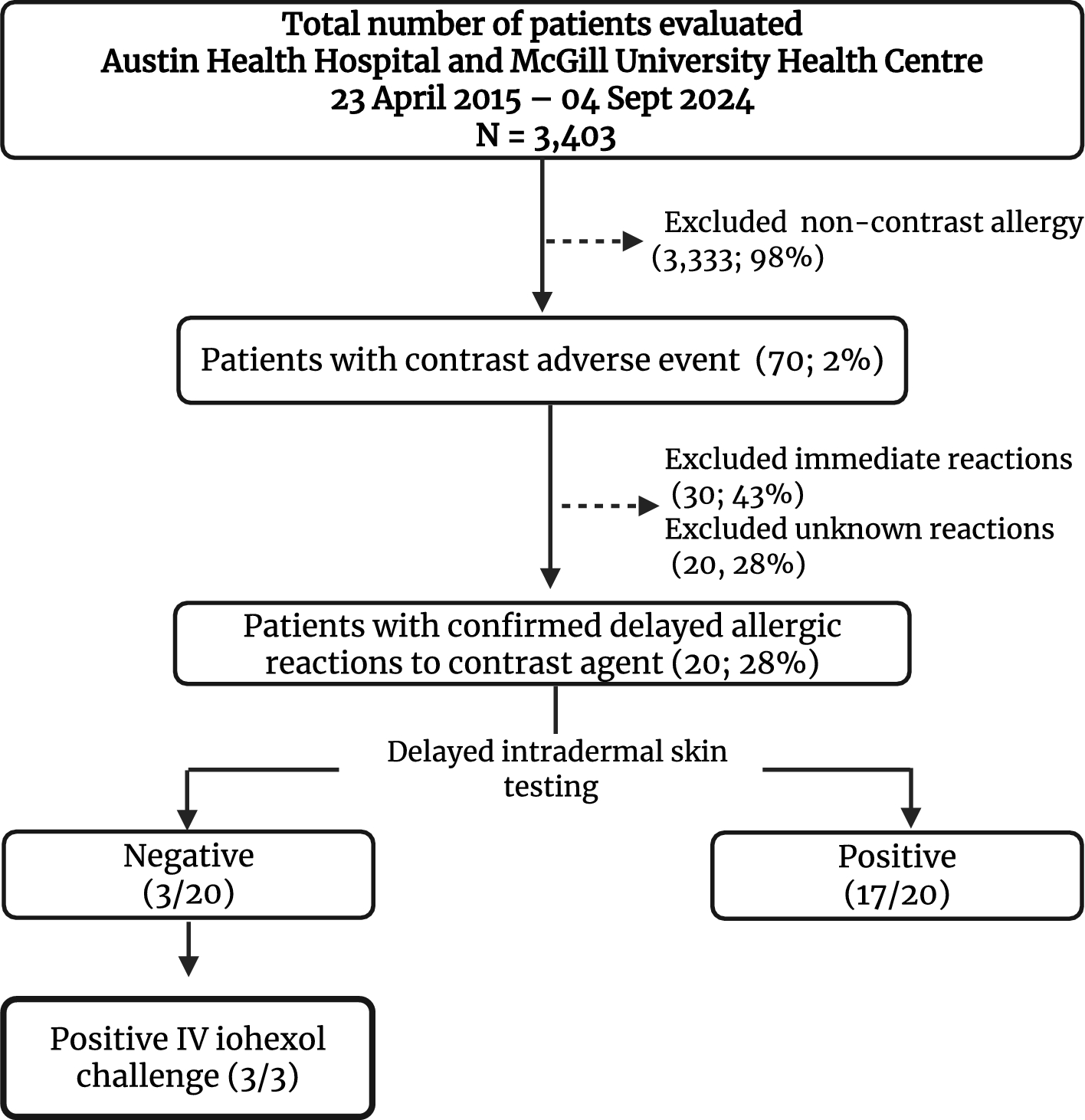
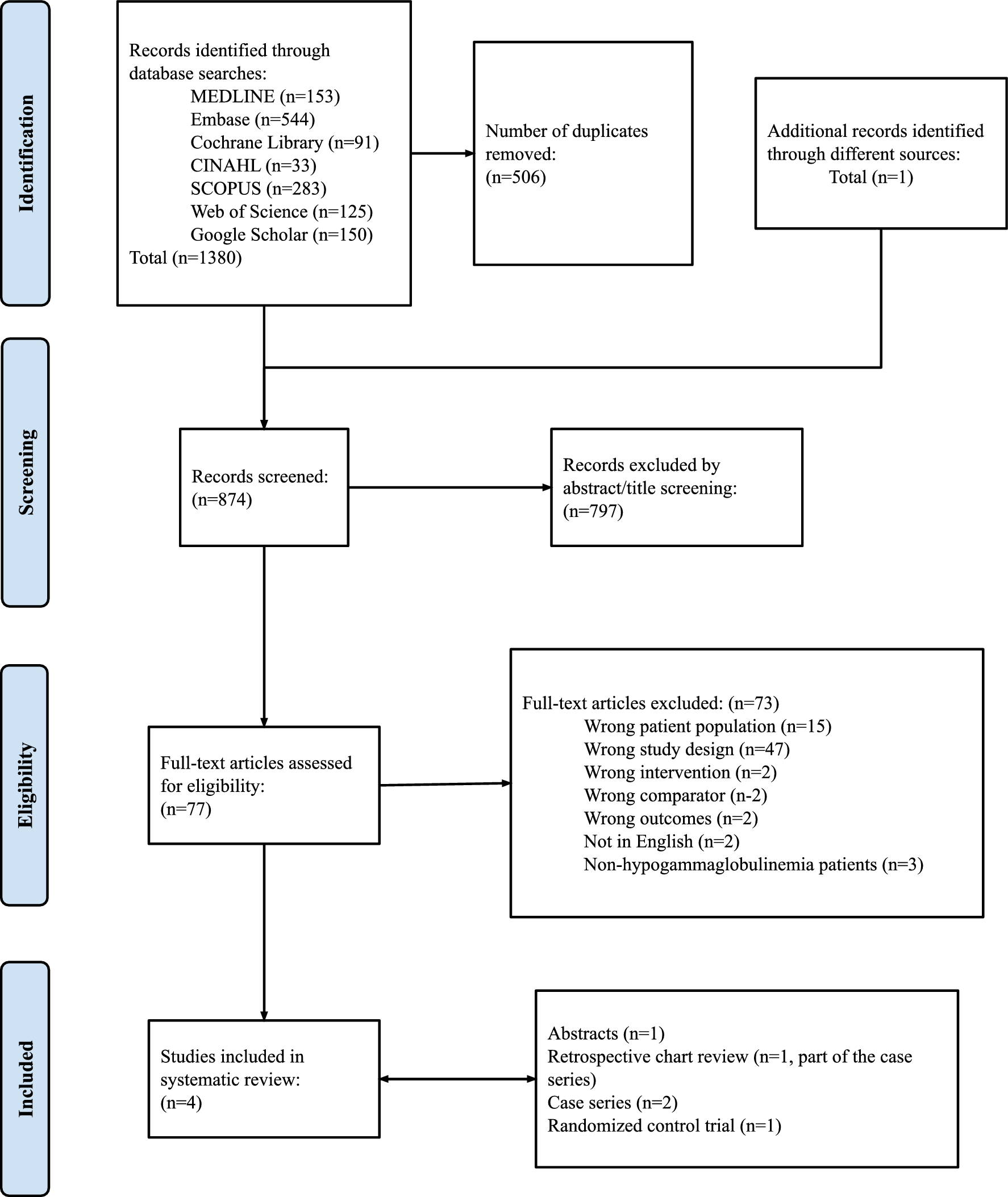
Among the 3403 patients evaluated for a drug allergy label in both centers, 70 reported a history of contrast adverse reaction (Fig. 1). Among these, 20 patients with 36 radiocontrast-associated DHRs were enrolled (Table 2), including 10 from Australia and 10 from Canada, between 2015 and 2024. Reactions occurred in patients who had not undergone specific premedication protocols to prevent them, with some individuals also having a history of multiple reactions. Iohexol alone was implicated in 16 subjects, iodixanol alone was involved in 2 subjects, and 2 subjects reacted after both iohexol and iodixanol.
Fig. 1
Delayed intradermal testing All 20 patients underwent dIDT, with 17 testing positive and 3 testing negative (Fig. 1). The three patients with negative dIDT (patients 6, 15 and 16) underwent an IV challenge with iohexol, and all had a positive non-severe IV challenge (no premedication) (Figs. 1, 2).
Fig. 2
Examples of delayed positive intradermal skin testing and intravenous challenges. A Patient 3—Positive for iohexol 1/10 (#2) and 1/1 (#8), iodixanol 1/10 (#3) and 1/1 (#9), iopromide 1/10 (#4) and 1/1 (#10), and ioversol 1/10 (#5) and 1/1 (#11). This patient had no systemic reaction following IDT and required topical and oral corticosteroids (prednisolone 25 mg PO for 3 days). B Patient 8—Positive for iohexol 1/10 (#2) and 1/1 (#3), iodixanol 1/10 (#4) and 1/1 (#5), iopamidol 1/10 (#8) and 1/1 (#9) at 12 h after intradermal testing. C Patient 13—Positive for iohexol 1/10 (#2) and 1/1 (#3), and iodixanol 1/1 (#5) on day 3 after intradermal testing. D Patient 14—Positive for iohexol 1/10 (#2) and 1/1 (#3), iodixanol 1/10 (#4) and 1/1 (#5), iopamidol 1/10 (#8) and 1/1 (#9) at 24 h after intradermal testing. E Patient 10—Positive for iohexol 1/10 (#2) and 1/1 (#3), iodixanol 1/10 (#5) and 1/1 (#6), and iobitridol 1/10 (#9) and 1/1 (#10). This patient had no systemic reaction following IDT and required topical corticosteroids. F Patient 10—Delayed IDT after 1 week. G Patient 19—Positive non-severe delayed reaction following IV challenge with iobitridol, presenting as a localized skin eruption at the previous IDT site for iohexol, iodixanol, and iobitridol. H Patient 16—Positive non-severe delayed reaction following IV challenge with iohexol, occurring 48 h after the challenge and lasting 72 h. No treatment was required. I Patient 15—Positive non-severe delayed reaction following IV challenge with iohexol
ICM cross-reactivity. Significant cross-reactivity was observed between iodixanol (the dimer of iohexol) and iohexol (Fig. 1). Among the 15 patients with a history of reaction to iohexol and a positive dIDT to iohexol, 100% (15/15) had a positive dIDT to iodixanol. Inversely, among the two patients with a history of reaction to iodixanol, both tested positive only to iodixanol on dIDT and one accepted iohexol and iopamidol challenges and tolerated them (Table 3).
Table 3 ICM hypersensitivity testing results and cross-reactivityAmong the 15 patients with a positive dIDT to iohexol, cross-reactive responses were observed between iohexol and iopromide (3/4, 75%; including one equivocald dIDT result), iohexol and ioversol (3/4, 75%), iohexol and iopamidol (4/6, 67%) and iohexol and iobitridol (3/5, 60%)—(Tables 2 and 3). In addition, patient 6, in whom reactivity to iohexol was confirmed by challenge after a negative dIDT, tolerated an iobitridol challenge leading to a cross-reactivity rate of 50% (3/6). Except for the patient who tested negative to iopromide, tolerance to all other non-cross-reactive ICM was confirmed by challenge. Three patients (1, 3 and 4) had positive dIDT to ioversol, iopromide, iodixanol and iohexol. Patients 3, 10 and 18 had a positive dIDT to iohexol, iodixanol and iobitridol. Four patients (7, 8, 14 and 17) had a positive dIDT to iohexol, iodixanol and iopamidol. Patient 19, who presented with severe maculopapular exanthem associated with iohexol, had positive dIDT to both iohexol and iodixanol and negative dIDT to iobitridol. The patient had no prior exposure to iobitridol. Based on the negative dIDT, an IV challenge with iobitridol was performed, which resulted in a localized skin eruption. This eruption occurred at the previous iobitridol intradermal testing site, which was distinct from the sites used for iohexol and iodixanol testing.
ICM challenge. Overall, 7/20 (35%) patients could tolerate a challenge with an alternative ICM (Table 2).
Ex vivo testing. The IFN-γ ELISpot was performed in 4 patients across a range of concentrations with inconsistent results in the context of a clear clinical history and positive dIDT (Table 4). In all 4 patients, the assay failed to identify the culprit ICM while showing the highest IFN-γ release to ioversol, including in patient 2, who subsequently tolerated an intravenous challenge with this same agent.
Table 4 Ex vivo testing results—ELISpot Results measuring interferon-gamma release by T lymphocytes in response to co-incubation with iodinated contrast media
Comments (0)