In this analysis of a survey among patients with various immunodeficiencies, the association of IgRT administration method with patient-reported outcomes was evaluated by comparing the responses of the cohort receiving IVIG and the cohort receiving SCIG.
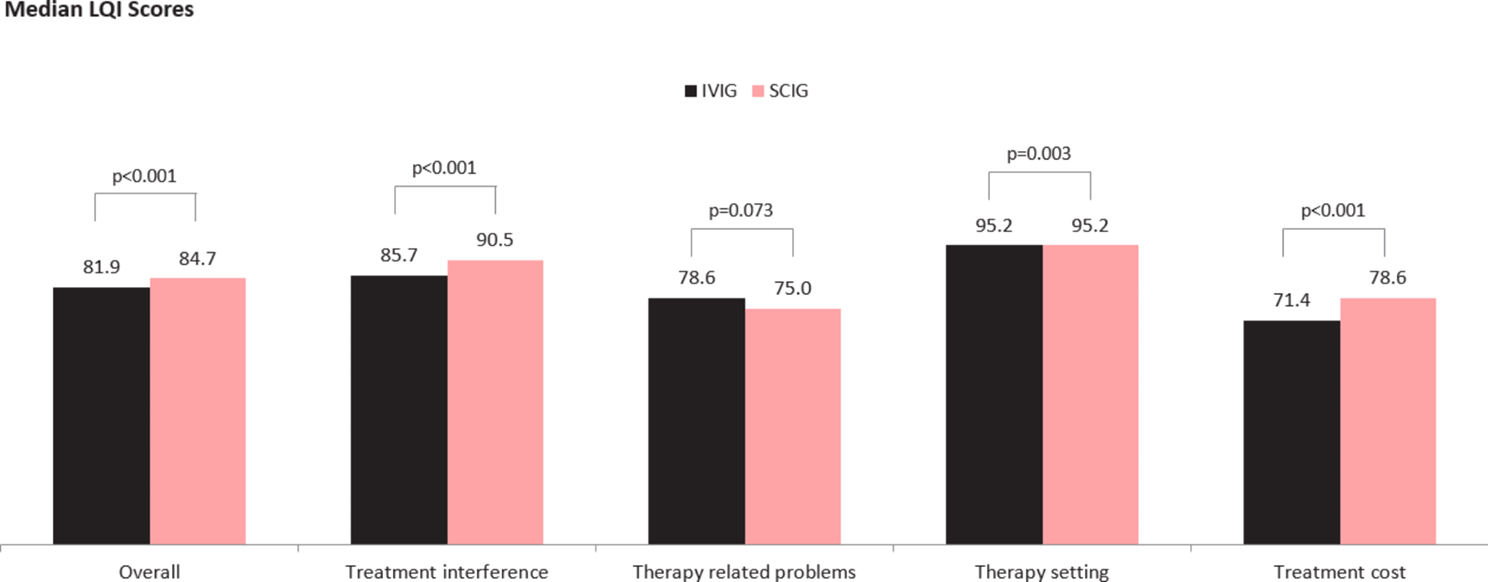
Overall, common variable immunodeficiency was the predominant type of immunodeficiency diagnosis, reported by about 3/4th of patients followed by general hypogammaglobulinemia, reported by an additional 11%. Other immunodeficiencies were reported much less frequently, including secondary immunodeficiency (SID) reported by 3%. SCIG was the more common of the 2 modes of IG administration, reported by 60% of patients, reflective of its growing role in treatment [24], including as high as 40% in patients with SID, consistent with another recent survey [24]. Patients receiving SCIG, compared to those on IVIG, reported a significantly greater score on the LQI tool. This finding is consistent with previous studies that have evaluated the relationship between IG administration methods and patient reported outcomes including quality of life or treatment burden. Gardulf et al. (2008) [4] found that a weekly SCIG infusion regimen was associated with significant improvements in HRQoL and treatment satisfaction, and as noted earlier, particularly in patients who had previously received IVIG therapy in hospital settings. A report on 6 clinical studies conducted in the US, Japan and Europe revealed significant improvements in IgG specific perceptions of quality of life and treatment satisfaction, as measured by the LQI, and in physical function and general health based on corresponding domains of the SF-36v2 Health Survey [35]. A recent study by Kan et al. (2022) [36] also reported higher health status scores (measured by SF-36v2 Health Survey) and IgG specific perceptions of quality of life and treatment satisfaction (LQI) among SCIG users compared to IVIG users. Finally, a recent survey of immunodeficiency patients in Quebec, Canada [24] found that patients on SCIG were associated with higher scores on the effectiveness domain of the Treatment Satisfaction and Quality Medication PRO tool [25], as also with greater acceptability of their symptom state, measured by the Patient Acceptability of Symptom State (PASS) tool [29].
Reported results on the LQI sub-domains and items shed additional light on specific perceived differences between the IVIG and SCIG groups. Thus, while the SCIG group was associated with better total and better 3 out of 4 sub-domain scores, the only exception was the Therapy-Related Problems sub-domain which contains three items, one of which refers to IG treatments in terms of whether they “Have improved my health”, arguably not surprising since IG modes of administration are not expected to differ in terms of their therapeutic effectiveness. On the other hand, SCIG users were significantly more likely to give one of the top two positive scores (6 or 7) on LQI items related to convenience (part of the LQI Treatment Interference sub-domain) including “Are scheduled according to my convenience”, “Do not make me too dependent on others” and “Do not limit my freedom to take trips or move”, and accordingly suggest that SCIG users perceived their treatment to be less lifestyle-limiting than IVIG users. Additionally the finding that SCIG users reported significantly higher scores as well as a higher percentage reporting top two score levels on an item/attribute such as (my IG treatments) “Are given in pleasant atmosphere” (part of the LQI Therapy Setting sub-domain) suggests that SCIG patients find their treatment setting, always their home, to be more pleasant, than IVIG patients find their treatment setting, typically although not exclusively, an infusion center/hospital, to be. Finally, the item (My IG treatments) “Require very little time and cost” was scored significantly higher (better) for SCIG users (as was the Cost sub-domain to which the item belongs) which also suggests that IVIG administration related (unreimbursed) travel costs and time burden does seem to have an unfavorable impact on patients receiving IVIG, compared to SCIG, consistent with evidence on the burden of IV infusions in other conditions as well [37,38,39]. Together, these factors contribute most to differences in IgG specific perceptions of quality of life and treatment satisfaction, as measured by the LQI.
In our evaluation of the LQI stratified by whether or not IVIG patients received their infusions at home or in the infusion center/hospital outpatient setting, we found that the latter sub-group of IVIG patients reported significantly more unfavorable LQI outcomes than IVIG patients receiving home infusions when each was compared to the SCIG group. Yet, even IVIG patients receiving home infusions had significantly poorer scores, compared to SCIG patients, on the Treatment Interference sub-domain which includes items such as (my IG treatments) “limiting my freedom to take trips or move” and “interfere with my social/family life” suggesting that health-care professional administered home IVIG infusions still limit patients’ freedom and sense of privacy and self-control. Overall however, these differences in LQI scores, by setting of IVIG administration, are consistent with a study by Kearns et al. (2017) [5] that did not find a significant difference between IVIG and SCIG users in the individual attribute “are convenient”, as all IVIG patients received their IgRT in the home setting, which is not typical [21, 24]. Consistent with Gardulf et al. (2008) [4], these findings seem to suggest that non-home setting of IVIG infusions certainly exacerbates the greater inconvenience of IVIG administration relative to SCIG administration.
SCIG users also scored other items on the LQI Treatment Interference sub-domain higher than IVIG users. Ratings were higher for SCIG users on the following LQI items: “Do not interfere with my work/school”, “Do not make me too dependent on others”, and “Do not limit my freedom to take trips or move”. Similarly, Lechanska-Helman et al. (2020) [40] found that where parents preferred SCIG over IVIG for children with antibody deficiencies, this choice was driven by the comparatively lower interference with their work or children’s schooling.
Finally, the two LQI items that assess treatment ‘effectiveness’, “My IG treatments, in my opinion are worthwhile” and “Have improved my health” were neither numerically nor statistically different between the IVIG and SCIG cohorts, reinforcing what would be expected in terms of similar treatment effectiveness of the two modes of administration. Taken together, these findings suggest it is convenience and the lack of interference with everyday life) that contribute to the higher overall IgG specific perceptions of quality of life and treatment satisfaction of SCIG patients with immunodeficiency.
Separately from LQI responses, IVIG users were significantly more likely to report missing work or school than SCIG users, indicating a potentially greater interruption to daily life due to treatment. This finding is supported by a previous systematic review and meta-analysis of home-based SCIG versus hospital based IVIG in treatment of primary antibody deficiencies by Abolhassani et al. (2012) [17], which found that home-based SCIG treatment was associated with fewer missed days of work. Lechanska-Helman et al. (2020) [40] similarly observed greater absence from school or work associated with IVIG use than SCIG use.
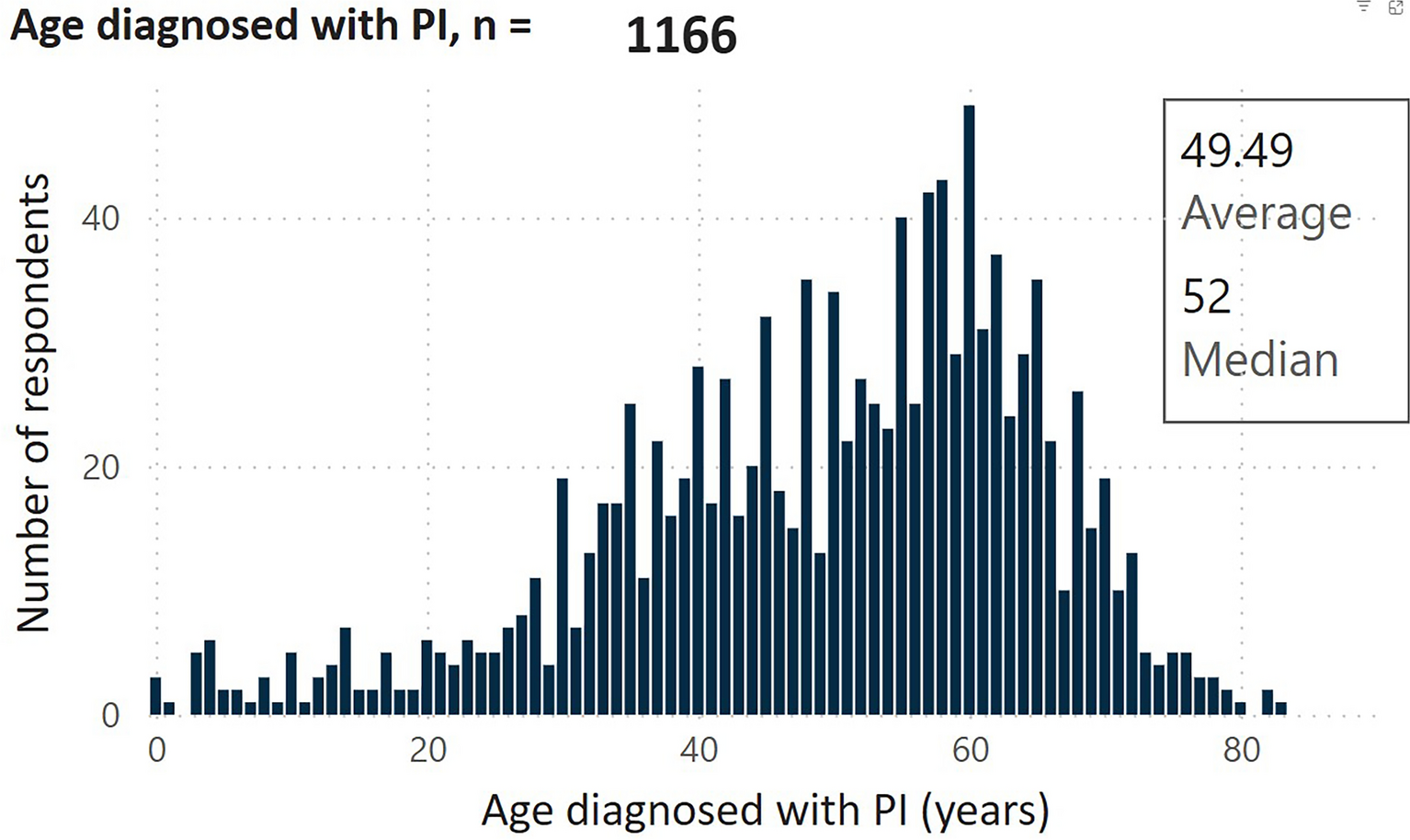
Overall, the Quick DASH score was low for both IVIG and SCIG users, indicating a low rate of disability/difficulty in the use of the shoulders and upper extremities. However, analysis of the individual scores indicated that interference with normal social activities was the highest scoring element (10% said that their arm, shoulder, or hand pain interfered “quite a bit” or “extremely” in normal social activities). IVIG patients were significantly more likely to report this interference and may have been selected for IVIG infusions on account of this greater upper-extremity disability that may be problematic with SCIG self-infusions. The IVIG cohort was also older than the SCIG cohort (60.2 years (63) vs. 56.8 years (59), (p < 0.001) respectively), and greater disability/difficulty in the use of the shoulders and upper extremities is expected in an older population.
Similarly, PROMIS PH-2 and MH-2 scores, measuring “physical health-” and “mental health-related function”, respectively, were not significantly different across the IVIG and SCIG users, which is not surprising, as in a cross-sectional survey comparing two cohorts, several external unmeasured factors can influence such general health outcomes [40]. This was also evident in the similarity on patient acceptability of current symptoms as measured by PASS and overall health perceptions (GHP). As previously noted, by contrast, longitudinal studies of switch from IVIG to SCIG have demonstrated improvements with change even in terms of physical function (as measured by SF-36 v2) [35].
The likelihood of missing school or work was found to be higher for patients on IVIG infusions. This is not surprising since all stages of IgRT took longer; the mean total time investment per infusion for IVIG was more than twice that of each SCIG infusion exclusive of travel time. While the majority of SCIG patients must infuse more regularly than IVIG users (weekly vs. every 4 weeks), it is shorter durations per infusion that have previously been demonstrated to improve patient satisfaction with treatment [15, 21]. Ultimately, at a patient level, choices between the two modalities could allow treatment regimens to be tailored to patient lifestyle and preference for either the more frequent but shorter infusions or longer but less frequent infusions. In summary, our results indicate that ideally switching from IVIG to SCIG would be expected to improve treatment satisfaction on a number of dimensions, but if for patient specific reasons such as lack of comfort with self-infusions, patients are unable to switch to SCIG, then at minimum switching IVIG patients to home infusion and/or more patient-sensitive scheduling of infusions would certainly be of potential patient benefit.
It is important to interpret PRO findings not only in terms of statistical significance but also clinical meaningfulness, in terms of anchor-based and/or empirical methods [41,42,43]. No published studies have evaluated clinically meaningful differences on the LQI in terms of a clinical anchor. Yet, clinical meaningfulness of observed change in the LQI has been determined empirically in terms of the Cohen effect size in a pooled analysis of phase 3 clinical studies evaluating switch from IVIG to SCIG in PID (Mallick et al. 2018). In our cross-sectional study, we similarly deduced clinical meaningfulness based on evaluated effect sizes and determined that differences between the IVIG and SCIG groups on the overall LQI, the Treatment Interference subdomain, the Therapy Setting subdomain, and the Treatment Cost subdomain were all minimally meaningful; however, the difference on the Therapy-related Problems subdomain was determined to be not meaningful. The effect sizes in our study were somewhat lower than those in Mallick et al. 2018, which also found minimal meaningfulness on the overall LQI but also all subdomain scores including the Therapy-related Problems subdomain, that was determined to not be meaningful in our study. The larger LQI improvements with patients switching from IVIG to SCIG, as in Mallick et al. 2018 compared to IVIG-SCIG differences across patient groups, identified in this study may be attributable to different study designs with respect to patient selection. The clinical studies presumably permitted an opportunity for patients switching from IVIG to benefit from previously unavailable SCIG, while in our observational survey, across-group IVIG vs. SCIG differences are likely to reflect in part that patients may already be optimized to their mode of administration based on real world preference or physician selection [44, 45]. Certainly the greater reported upper extremity disability in the IVIG group reflecting in our study would seem to suggest these patients may have been found unsuitable for self-infused SCIGs [44, 45].
Study limitations
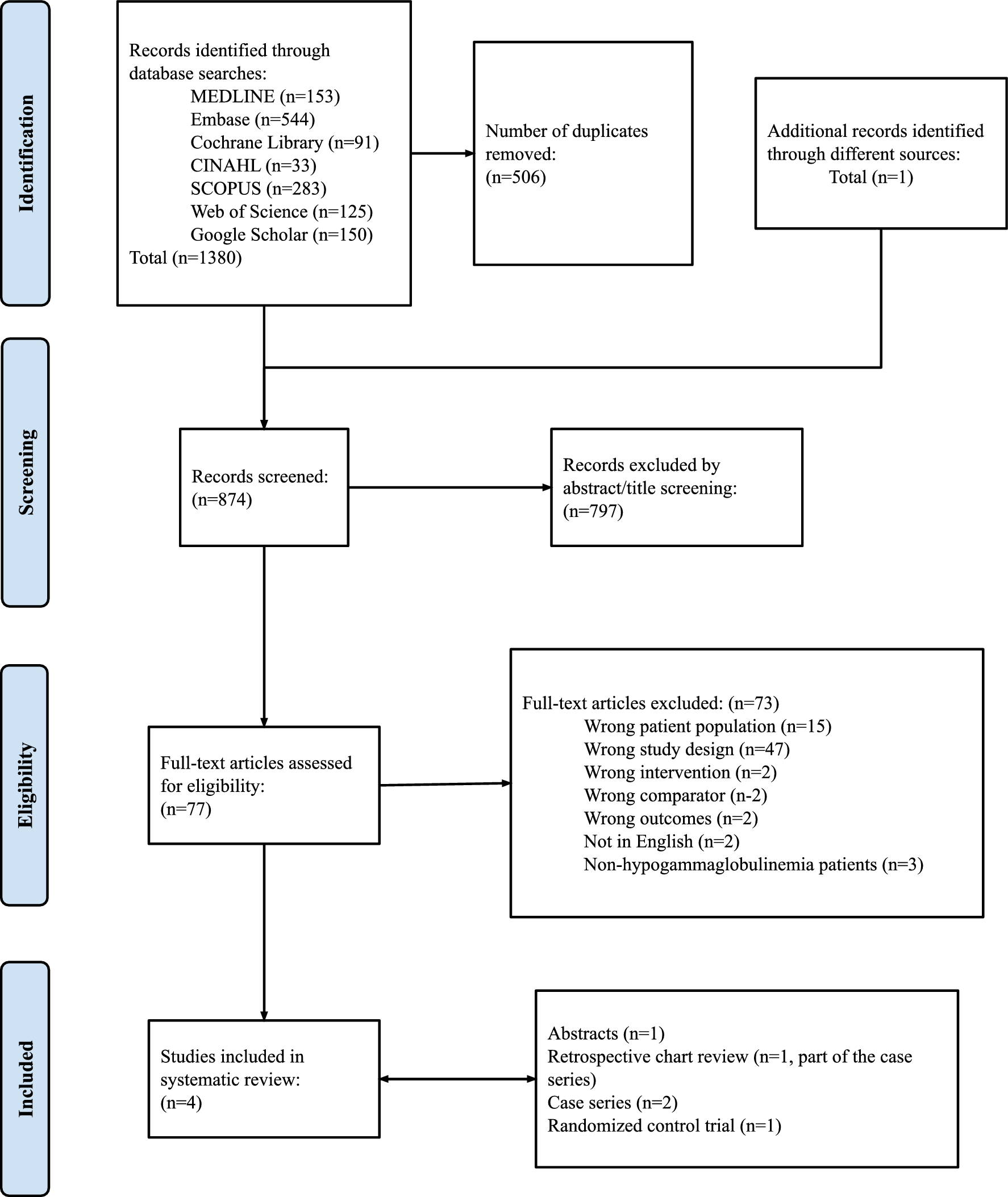
There are inherent limitations with patient-reported surveys, as with any real-world data analysis, which should be borne in mind in interpretation of the evidence. Survey responses inherently rely on patient understanding of the survey questions as unlike in-patient interviews, there is not an opportunity to clarify their meaning. Further, responses to scales assessing various concepts can be contextualized by patients in different ways depending on individual personality and disposition (optimism versus pessimism, happiness versus unhappiness) [46]. Such influences are however more likely to affect the general rather than specific concepts and measurements, as for example suggested by the Wilson-Cleary framework of health outcomes; [47] thus in our study more likely to be reflected in assessment of general health perceptions than immunoglobulin specific perceptions of quality of life and treatment satisfaction [21]. Additionally, as survey responses were not independently verified with patients’ physicians, some of the findings especially as relates to specific immunodeficiency subtype and/or other related conditions may be impacted by absence of fully accurate patient recall on their medical history [48]. Due to the nature of rare disease research, the survey had a relatively low response rate and may have been skewed in terms of certain respondent groups, for example immunodeficiency sub-type. Thus, although IG is known to be underutilized among patients with SID [9, 10], one might still have expected a somewhat higher share of SID among the immunodeficiency population receiving IG therapies in this survey, as another recent survey revealed an overall SID proportion of 10% among IG patients with immunodeficiencies [24], and to that degree results in this survey may not be generalizable to SID. Finally, patient perceptions and preferences for modes of administration can change over time, which was not able to be captured in this cross-sectional survey.
Only US patients were included in this study, and therefore findings may not generalize to outside the US due to practical differences in how patients can access Ig. For example, in the US the availability of home healthcare services permits the opportunity to administer IVIG at home, which is not an option in all countries. Similarly, SCIG can also be collected in the US from local specialty pharmacies or delivered at home, adding to SCIG convenience that may not be possible in other countries where SCIG may have to be collected, for example from specialized blood banks or hospital pharmacies, and may take an average of an hour or more each time [24].

Comments (0)