The association between BMI and lumbar BMD has been extensively investigated across diverse demographic cohorts. However, the specific relationship is nonlinear and context-dependent, with studies reporting divergent conclusions. Notably, a significant positive association between BMI and lumbar BMD with the coeffietient 0.056 has been documented in Tang’s study [7]. While the biological mechanisms underlying this association remain only partially elucidated, two prominent hypotheses have emerged. The mechanical loading hypothesis posits that chronically elevated mechanical stress on weight-bearing bones in individuals with higher BMI induces osteogenic activity, thereby augmenting BMD [7]. Alternatively, an endocrine-mediated pathway has been proposed involving regulatory interplay between adipokines (insulin-like growth factor 1 [8]) and bone-active hormones (estrogen [9]), which modulate the homeostasis of adipose and osseous tissues.
In addition to the positive correlation between BMI and BMD, negative correlations have also been found in other studies, with several different mechanisms being reported to be involved in those negative relationships. For example, obesity-related oxidative stress and low-grade chronic inflammation may stimulate the activity of osteoclasts, leading to reduced BMD [10, 11]. Obesity could also stimulate pre-osteoblasts to differentiate toward adipocytes rather than osteoblasts, resulting in increased bone fragility [12].
Our present study showed a positive association between BMI and lumbar BMD. In the subgroup analysis stratified by gender, this positive correlation maintains consistency, though some disparity was observed between genders. Although the relationship between female BMI and BMD is significant in all three models, its correlation is slightly lower than that of males. This may be related to biological differences in women, hormone levels, or health behavior.
The observed sexual dimorphism in body composition and endocrine signaling likely arises from divergent adipose tissue distribution patterns and hormonal regulation [13]. Women exhibit estrogen dominance in bone metabolism, whereas men rely on testosterone’s direct effects and its indirect contribution via peripheral aromatization to estrogen [14]. Males demonstrate preferential accumulation of visceral adipose tissue (VAT) [15], a metabolically active depot strongly associated with chronic low-grade systemic inflammation. VAT functions as an endocrine organ, releasing proinflammatory cytokines (e.g., TNF-α and IL-6) and free fatty acids that mechanistically contribute to insulin resistance and oxidative stress through dysregulation of glucose homeostasis and mitochondrial dysfunction [16]. These factors inhibit osteoblast activity while stimulating osteoclastogenesis, partially offsetting the mechanical benefits of higher body weight on bone [17]. Additionally, males exhibit lower circulating estrogen levels compared to females, reducing the antiresorptive effects of estrogen on bone metabolism [9]. This dual burden of inflammation and diminished hormonal protection may explain the stronger positive correlation between BMI and BMD in males, as mechanical loading alone cannot fully counteract metabolic harms. Conversely, females have higher subcutaneous fat [13], which may secrete adipokines (leptin), with mixed effects on bone metabolism [18, 19]. Estrogen’s protective role in bone health [20] might further explain the weaker correlation in females.
The observed racial disparities in the association between BMI and lumbar BMD may stem from multifactorial interactions involving genetic, hormonal, and body composition differences. For instance, African American populations are reported to have higher baseline BMD compared to Caucasians, potentially due to genetic polymorphisms influencing bone remodeling pathways, such as variations in the LRP5 or VDR genes linked to bone density regulation [21,22,23]. Additionally, racial differences in fat distribution (visceral vs. subcutaneous adipose tissue) and muscle mass may modulate mechanical loading effects on bone. Hormonal factors, such as vitamin D status (influenced by skin pigmentation and sun exposure) may further contribute [24, 25]. Socioeconomic factors could also play a role in these disparities [26]. Future studies incorporating bioimpedance analysis or dual-energy X-ray absorptiometry (DXA)-derived fat/lean mass measurements are warranted to elucidate these mechanisms.
In subgroup analyses stratified by BMI tertiles, the positive association between BMI and lumbar BMD was observed exclusively in the highest tertile (Q3: BMI ≥ 40 kg/m²). Employing further threshold effect analysis, our findings revealed a U-shaped relationship between BMI and BMD, with a point of inflection at 36.1 kg/m2. When a BMI was less than 36.1 kg/m2, the relationship between BMI and lumbar BMD was negatively correlated. When a BMI was greater than 36.1 kg/m2, the relationship was positively correlated. The non-linear association likely reflects competing mechanisms influenced by the severity of obesity, as hereby explained. (1) Metabolic dominance at lower obesity levels (BMI 30–36.1 kg/m²), as follows. In individuals with moderate obesity, metabolic dysfunction—driven by visceral adipose tissue accumulation—may suppress bone formation. Excess visceral fat secretes proinflammatory cytokines (TNF-α, IL-6) and adipokines (leptin), which promote oxidative stress and insulin resistance [10, 12]. These factors inhibit osteoblast differentiation and activity while stimulating osteoclastogenesis, leading to reduced BMD [10, 12]. Concurrently, insulin resistance impairs the anabolic effects of insulin-like growth factor 1 (IGF-1) on bone remodeling [8], supporting the observed inverse relationship between BMI and BMD. (2) Mechanical and hormonal adaptation at higher obesity levels (BMI > 36.1 kg/m²), as follows. Beyond the inflection point, mechanical loading from increased body weight may override metabolic harms. We acknowledge BMI’s limitations in assessing tissue-specific effects and therefore advocate for future mechanistic studies incorporating dual-energy X-ray absorptiometry (DXA). Additionally, according to Wolff’s law, repetitive stress on the skeleton stimulates osteoblast-mediated bone formation to adapt to heavier loads [7]. Severe obesity is associated with elevated estrogen levels due to aromatization of androgens in subcutaneous adipose tissue [9], which exerts antiresorptive effects on bone. Furthermore, higher muscle mass relative to fat mass in some individuals with severe obesity could amplify mechanical benefits, as lean mass strongly correlates with BMD [27]. These adaptive responses may explain the positive correlation between BMI and BMD in the Q3 group (BMI > 40 kg/m²). The inflection point (BMI 36.1 kg/m²) likely marks a shift in the dominant regulatory mechanism. Below this point, metabolic dysfunction (inflammation and insulin resistance) outweighs mechanical stimuli. Above it, mechanical loading and compensatory hormonal changes (e.g., estrogen and IGF-1) become predominant. In addition, Song’s research also shows a positive correlation between BMI and lumbar spine BMD [28]. This dual-phase mechanism aligns with the “obesity paradox” where severe obesity may confer protective effects in certain contexts [29]. However, individual variability in fat distribution (visceral vs. subcutaneous) and muscle mass complicates this relationship, underscoring the need for body composition analysis in future studies.
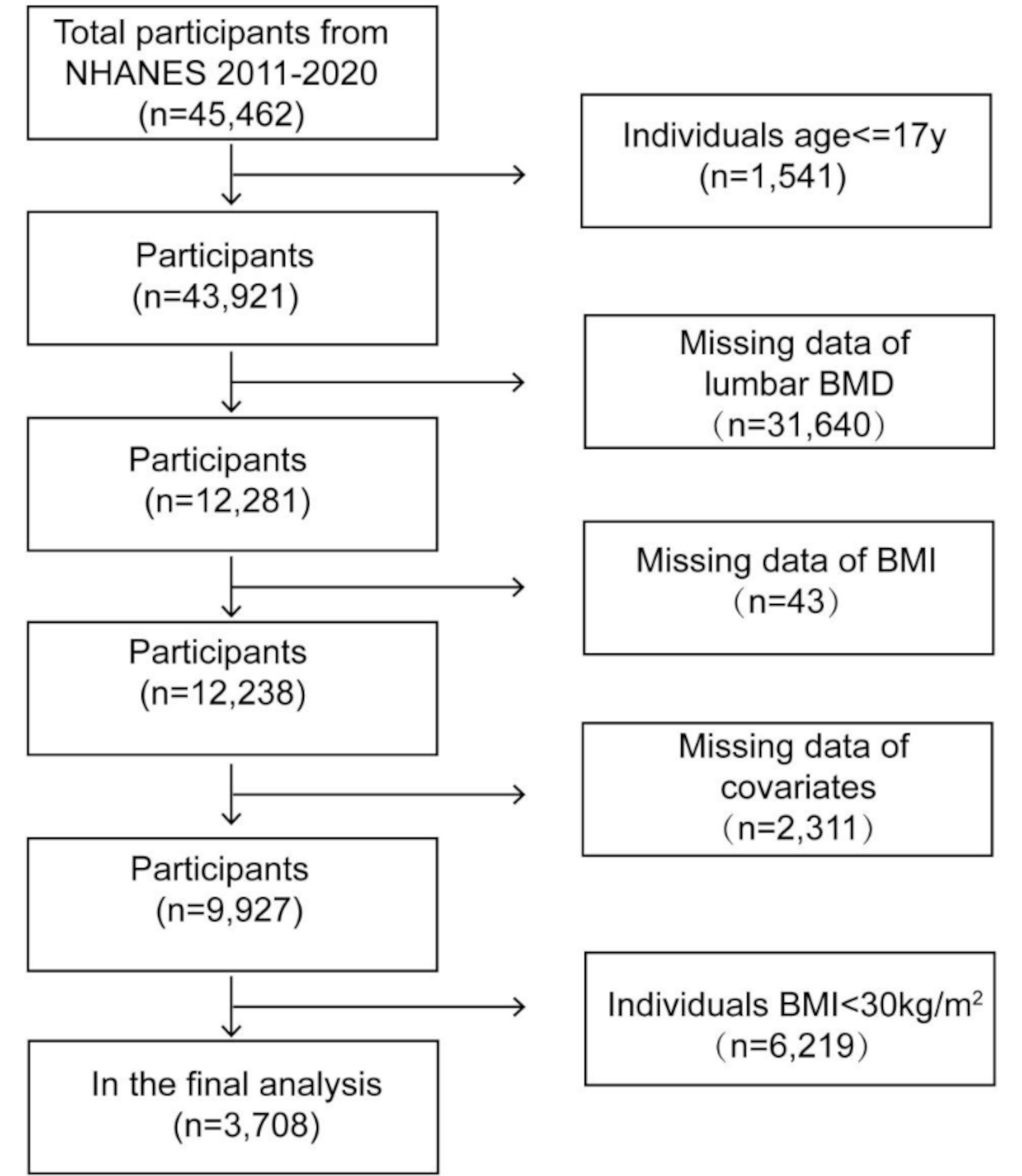
Our study utilized a large, nationally representative sample from NHANES 2011–2020, enhancing the generalizability of our findings. The identification of a U-shaped relationship between BMI and lumbar BMD provides novel insights into the complex interplay between obesity and bone health. This nonlinear association underscores the need to consider BMI thresholds in clinical assessments, particularly for individuals with BMI ≥ 36.1 kg/m² where mechanical loading may outweigh metabolic risks.
However, our study has several limitations. First, the cross-sectional design inevitably limited the drawing of an inference of a causal correlation between BMI and lumbar BMD among obese adults. More fundamental mechanistic research was needed to understand their particular mechanism. Second, while BMI is a practical obesity metric in epidemiological settings, it does not differentiate fat mass from lean mass, which are key determinants of bone health. Although NHANES lacks direct body composition data (e.g., DXA-derived fat/lean mass), we adjusted for biochemical markers (albumin and creatinine) as surrogates. Hormonal profiles (e.g., IGF-1 and leptin) were also unavailable, potentially confounding the BMI-BMD relationship. Nevertheless, our findings highlight the need for future studies integrating body composition and hormonal assays to clarify whether the U-shaped association reflects mechanical adaptation or metabolic interplay. Although BMD remains a validated predictor of fracture risk in the general population [30], its utility may be attenuated in obese populations due to the dual regulatory effects of adipose tissue on bone metabolism [5]. For instance, Compston demonstrated that overweight/obese women exhibit higher lumbar BMD without proportional reduction in non-vertebral fracture risk, underscoring the need to integrate bone microarchitecture (trabecular bone score and TBS) or fall risk factors for comprehensive assessment [31]. The BMD rebound observed at BMI > 36.1 kg/m² in our study may reflect mechanoadaptive compensation, although its translation to fracture risk reduction requires prospective validation. These limitations do not invalidate the observed threshold effect but contextualize its interpretation.




Comments (0)