To the best of our knowledge, this is the first web-based survey exploring endocrinologists’ adherence to the 2023 ETA Clinical Practice Guidelines for thyroid nodule management. We surveyed the approach to two nearly identical clinical scenarios involving a 2.5 cm solitary nonfunctioning thyroid nodule in a middle-aged woman with an FNA cytology report of Bethesda III-AUS, but with differing ultrasound characteristics and associated sonographic risk of malignancy (ROM). Our sample was representative of the national population of endocrinologists in Greece and of sufficient size, owing to a solid response rate of 25%, comparable to other surveys [13, 14].
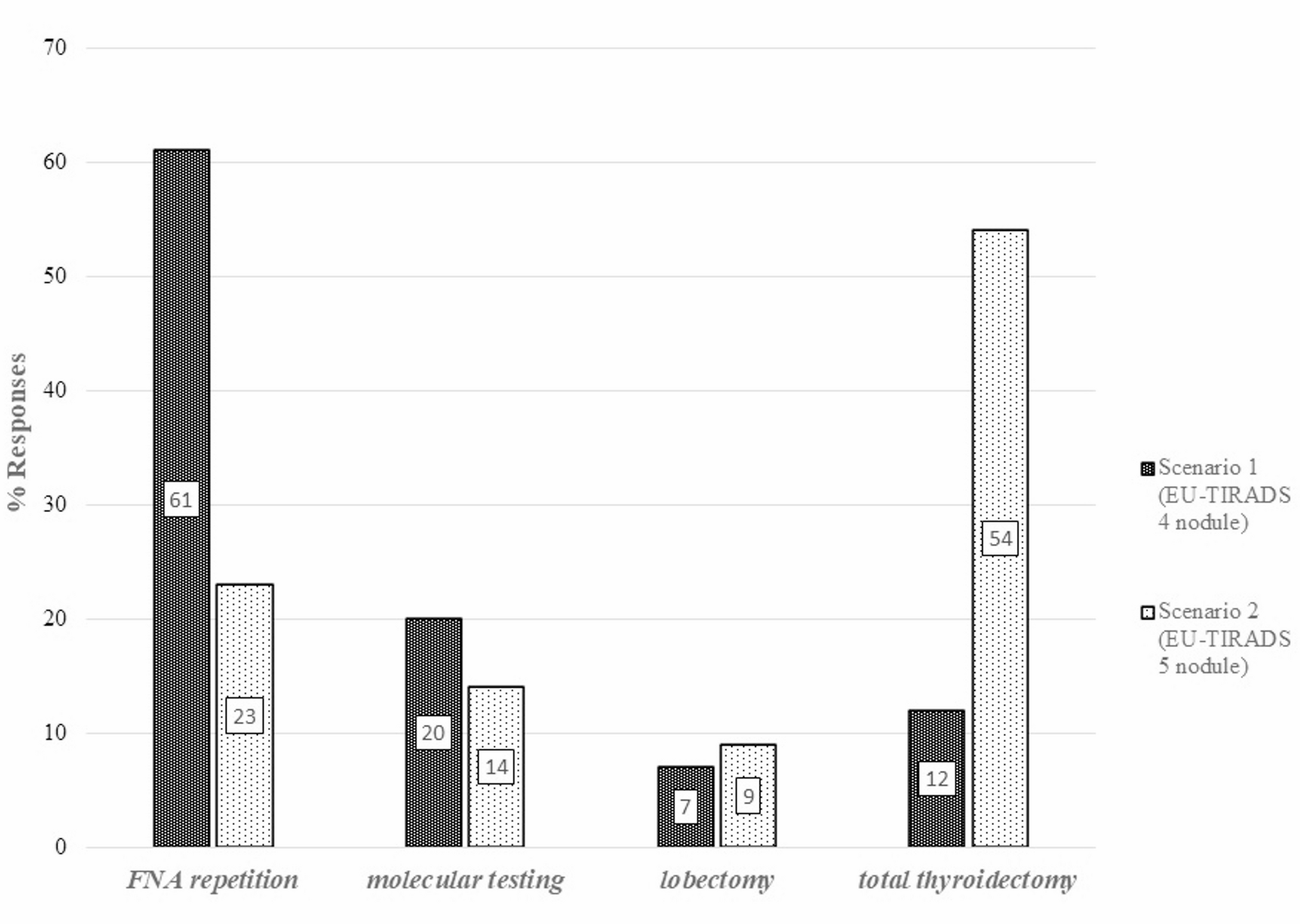
The main and most intriguing finding is the substantial deviation from the recently released ETA guidelines. The EU-TIRADS category significantly influenced the clinical decisions of the respondents and took precedence over cytology results. For a nodule classified as EU-TIRADS 4, 61% of endocrinologists opted for repeat FNA, whereas for a nodule classified as EU-TIRADS 5, 54% favored total thyroidectomy, with only 23% choosing repeat FNA. This approach deviates from the recommendations of not only the ETA, but also of several other scientific societies [5, 7, 15, 16]. The recent 2023 ETA guidelines [6] mandate repeat FNA in these clinical scenarios regardless of the EU-TIRADS category. The primary reasons cited for not adhering to the guidelines were skepticism about them, as well as the lack of access to reliable neck ultrasonography and molecular testing nationwide. Lack of proper information and of experienced surgeons is frequently invoked.
Few surveys have examined clinical practices in the management of thyroid nodules. One American web-based survey, conducted in 2015 and completed by 897 members of the Endocrine Society, AACE, and ATA, found that for AUS/FLUS cytology, 31.5% of respondents opted for repeat FNA, 38.8% for molecular testing, and 24.4% referred patients for thyroid surgery [17]. It is important to note that this survey was conducted immediately prior to the release of the 2015 ATA guidelines.
Repeat FNA may significantly reduce the number of unnecessary surgeries. In nodules with AUS cytology, repeated FNA yields benign results in 36–50% of cases [10, 18]. In our study, FNA repetition was preferred by most participants (61%) for an EU-TIRADS 4 nodule, but only by 23% for an EU-TIRADS 5 nodule. The most experienced endocrinologists with over 10 years of post-residency experience, and comprising 66% of our sample, tended to avoid repeat FNA, preferring total thyroidectomy for EU-TIRADS 4 nodules instead. This is likely an example of “clinical inertia”, in which older Greek endocrinologists may not have adjusted their approach to thyroid nodule management, particularly regarding FNA before surgery [19]. For example, between 2007 and 2016, the indications for total thyroidectomy in Southwestern Greece were often unclear and suspicious FNA cytology for malignancy was documented in only 35.4% of cases prior to surgery. However, from 2011 to 2016, FNA use increased, indicating a shift toward more evidence-based decision-making and reduced instances of unjustified total thyroidectomy. In Greece, FNA is performed under ultrasound guidance by both endocrinologists and radiologists in both public and private sectors; however, we lack national data on the extent to which each group performs the procedure. Compared to physicians in the private sector, those in the public sector were more likely to choose repeat FNA for highly suspicious nodules, probably because aspirations are readily available at public hospitals and reimbursed by our healthcare system.
Molecular testing was chosen by only 20% of participants in the first clinical scenario and by 14% in the second. Jammah et al. reported that 47.3% of endocrinologists opted to repeat FNA in cases of AUS/FLUS (follicular lesion of indeterminate significance), while only 14.1% selected molecular testing due to its limited availability [20]. In contrast, a 2016 clinical survey in Italy found that molecular testing was the preferred approach for AUS/FLUS cytology. That study included 566 members of the Associazione Medici Endocrinologi (AME), with a response rate of 29.6% among respondents: 46% chose molecular testing followed by surgery if the result was positive, 43.6% preferred ultrasound follow-up due to the low malignancy risk, and only 9.3% recommended surgery, without providing further information [13]. Notably, the option to repeat FNA was not provided in that survey and only half of the participants had read the full guidelines. In addition, molecular testing is reported to be 2–5 times more likely in North America compared to other regions, possibly due to its being reimbursed by private insurance when clinically indicated [17]; nevertheless, in the aforementioned web-based survey, only 38.8% selected molecular testing for nodules with AUS/FLUS cytology. In Europe, commercial platforms for molecular testing of thyroid nodules are not routinely available. In Greece, only locally developed gene panels are accessible and only in the capital and the second-largest city. These panels are not covered by the national health system and information about their availability is limited. These factors significantly constrain Greek endocrinologists in utilizing molecular testing.
Regarding the surgical procedure for indeterminate solitary thyroid nodule, most Greek endocrinologists prefer total thyroidectomy over lobectomy. Fewer than 10% of endocrinologists chose lobectomy in either scenario, which is consistent with a previous report showing that this type of surgery is not widely practiced in Greece [19]. Notably, total thyroidectomy was preferred by 12% of clinicians for EU-TIRADS 4 nodules– particularly those with over 10 years of experience– and by 54% for EU-TIRADS 5 nodules. This preference for aggressive management of large or rapidly growing nodules mirrors a 20-year-old American survey conducted before FNA and molecular testing became widespread [21] supporting clinical inertia as a factor in current attitudes. High-resolution ultrasonography remains the best imaging modality for assessing malignancy risk, with the EU-TIRADS TR5 category showing the highest diagnostic accuracy according to a recent meta-analysis [22]. Studies by Trimboli et al. and Lu et al. reported malignancy rates of 87.7% and 80.4% for EU-TIRADS 5 nodules, far exceeding the 22% malignancy rate for Bethesda AUS/FLUS nodules [23, 24]. These findings may raise concerns about the safety and applicability of new approaches for patients with highly suspicious features for thyroid nodules measuring 2.5 cm. However, endocrinologists in the private sector and physicians in large cities are more likely to favor lobectomies. This may be because patients from rural areas are often referred to high-volume surgeons in cities due to a lack of local expertise, making a second completion surgery a logistical challenge.
Although the final question on reasons for non-adherence was not specific to the 2023 ETA guidelines for thyroid nodule management and was intended to apply broadly across all scenario clusters, it still offers valuable insight into general barriers to guideline adherence. Almost half of the responders expressed skepticism about the evidence, about one-third reported an inability to perform reliable ultrasound, approximately one-third cited the unavailability of molecular tests, and about one-fifth indicated a lack of proper information or a shortage of high-volume surgeons. In contrast, a survey of ATA members regarding the 2015 Adult Thyroid Nodule and Differentiated Thyroid Cancer Clinical Practice Guidelines reported that 83% of the responders strongly agreed that the guidelines were easy to apply in daily practice [14]. However, the survey did not assess how these guidelines influenced actual clinical decision-making. An important issue to consider is the discrepancy between physicians’ perceptions of guideline validity and their real-world decision-making. A more recent study by Schumm et al. demonstrated significant variation in guideline adoption and the extent of surgery or active surveillance [25]. Notably, physicians’ perception of 5- and 10-year cancer recurrence risk accounted for only 10.3% of the observed variance in decision-making for papillary thyroid cancer (PTC) patients.
This web-based survey has certain limitations. The final question addressing reasons for non-adherence to guidelines was, as mentioned, not specifically tailored to the 2023 ETA guidelines for the management of thyroid nodules. The limited availability of local laboratory panels for molecular genetic testing represents another constraint. The survey was conducted only 3 months after the publication of the ETA 2023 guidelines, which probably did not allow sufficient time for the guidelines to be widely incorporated into clinical practice. A further investigation should be conducted again after better assimilation of the 2023 ETA guidelines. However, the preference of experienced endocrinologists for total thyroidectomy over FNA repetition in the EU-TIRADS 4 and 5 categories with AUS cytology contradicts the recommendations of established scientific societies released over the past decade, such as the Bethesda 3rd edition and 2015 ATA guidelines. Additionally, the survey enrollment period lasted 5 months, potentially introducing bias. Participants responding closer to April 2024 may have had greater exposure to the guidelines compared to those who participated earlier. Changing long-established practices requires time and improved dissemination of guidelines and evidence-based data, facilitated through continuous medical education.
For clinical practice guidelines to achieve their purpose, their implementation is at least as important as their development and publication; however, this issue has received comparatively little attention. Numerous studies have highlighted the failure of clinicians to follow clinical practice guidelines [26, 27]. One of the main reasons for this is older age [26], as we also observed in the present survey. Clinicians in the latter half of their careers often practice based on personal experience rather than established guidelines. A thorough understanding of the reasons for physicians’ non-adherence to clinical guidelines is crucial for improving healthcare outcomes. Our findings underscore the urgent need to implement strategies that go beyond simply releasing guidelines. They are relevant not only for the latest ETA guidelines, but also for the upcoming ATA guidelines on thyroid nodules, specifically regarding their adoption in Europe or in other countries with healthcare landscapes similar to that of Greece. Systematically documenting the reasons for non-adherence is the obvious first and necessary step in understanding them in depth so that they can be properly addressed in order to optimize the management of thyroid nodules and improve patient outcomes.




Comments (0)