
Remember me
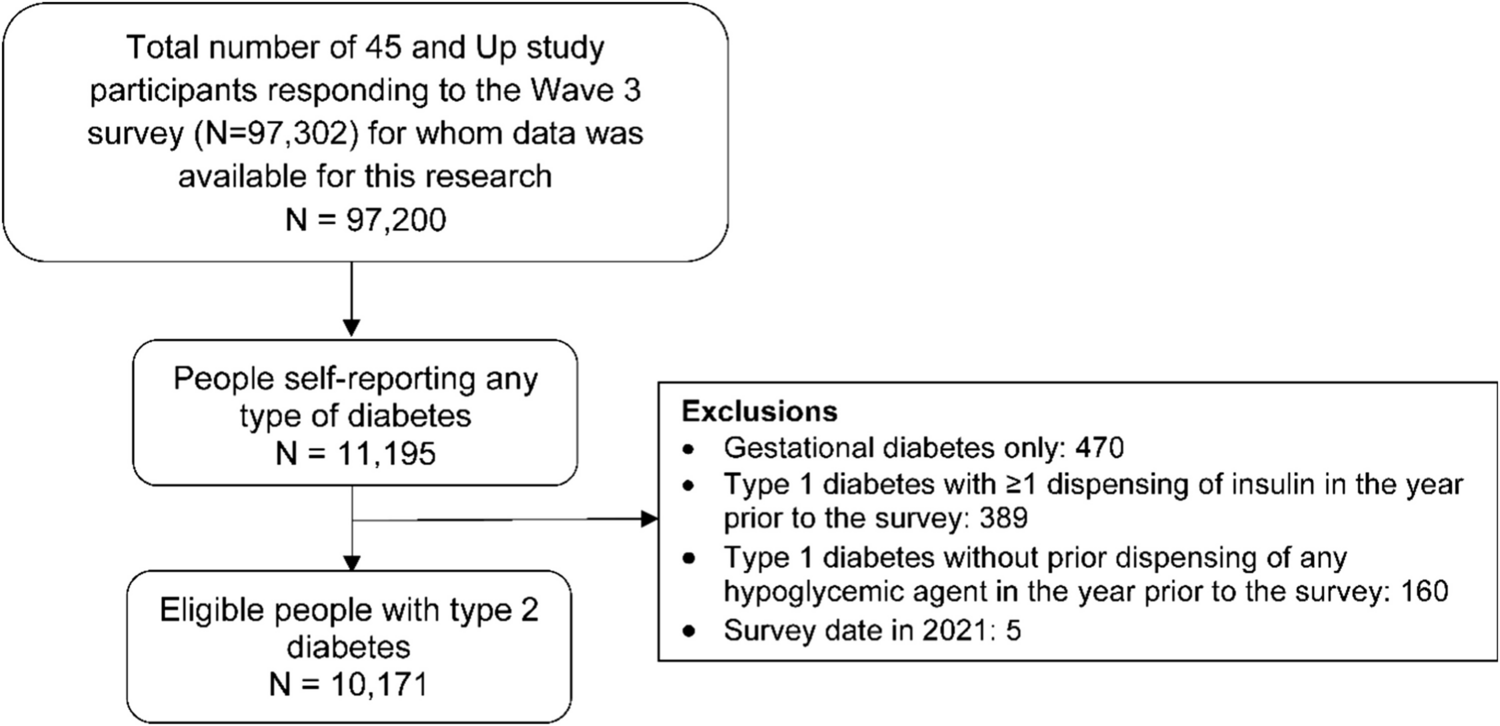
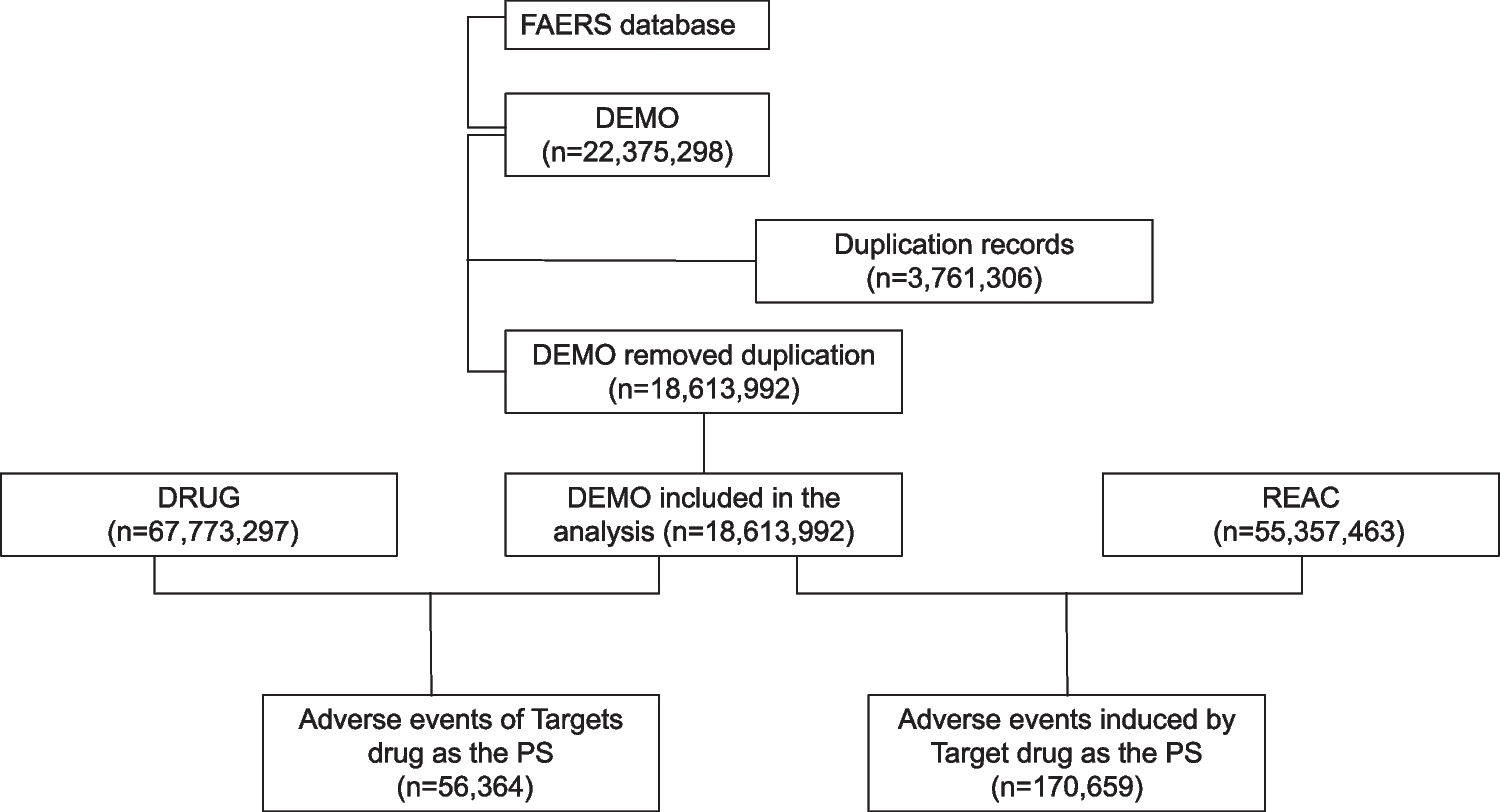

The systematic literature search revealed 9692 studies overall. We excluded 9632 studies during screening on the basis of title and abstract; the remaining 60 studies underwent full-text review, and 43 of them were subsequently excluded for reasons outlined in Fig. 1, leaving 17 studies to be considered in the systematic review. The studies were published between 2017 and 2024 and included overall 2,613,693 patients (eTable 2). Nine studies were conducted in North America [13, 17, 22,23,24,25,26,27,28], four studies in Asia [14, 29,30,31], and four studies in Europe [32,33,34,35].
Fig. 1
Flowchart illustrating the selection of included studies. Abbreviations: RCTs, randomized controlled trials; DOACs, direct oral anticoagulants
Twelve studies used healthcare claims data [13, 14, 17, 22, 24,25,26,27,28,29, 32, 35], two studies used nationwide registries [33, 34], and three studies used electronic health records (eTable 2) [23, 30, 31]. Three studies applied nested case–control designs [14, 24, 25] and 14 studies applied cohort designs [13, 17, 22, 23, 26,27,28,29,30,31,32,33,34,35]. AF was explicitly mentioned as an inclusion criterion in 13 studies [13, 14, 17, 22,23,24,25,26, 28,29,30, 33, 34]; the other four studies did not specify the indication for DOAC use [27, 31, 32, 35]. Five studies included patients adding on an antiarrhythmic drug while on a DOAC [14, 17, 26, 28, 31], three studies included patients adding on a DOAC while on an antiarrhythmic drug[13, 22, 32], while the temporal order of the two drugs was not specified in nine studies [23,24,25, 27, 29, 30, 33,34,35]. Eight studies compared concomitant use of DOACs and antiarrhythmic drugs versus use of DOACs alone [14, 22,23,24,25, 29, 30, 32], six studies compared concomitant use of DOACs and antiarrhythmic drugs versus concomitant use of DOACs and non-antiarrhythmic drugs [13, 26,27,28, 31, 35], two studies compared concomitant use of DOACs and antiarrhythmic drugs versus concomitant use of VKAs and antiarrhythmic drugs [33, 34], and one study compared concomitant use of DOACs and antiarrhythmic drugs versus concomitant use of DOACs and other antiarrhythmic drugs [17]. Selected patient characteristics in the included studies can be found in eTable 3.
Concomitant use of DOACs and antiarrhythmic drugs versus use of DOACs aloneEight studies compared concomitant use of any or specific DOACs and antiarrhythmic drugs versus use of any or specific DOACs alone regarding the risk of major bleeding (Table 1) [14, 22,23,24,25, 29, 30, 32]. Most comparisons yielded increased risks, with the strongest increases being observed for DOACs plus verapamil versus DOACs (OR, 1.56; 95% CI, 1.02–2.39) [14] and for DOACs plus diltiazem versus DOACs (HR, 1.56; 95% CI, 1.15–2.12) [23]. Two studies assessed the risk of stroke/SE and all-cause mortality showing no differences [30, 32].
Table 1 Main findings of the included studiesConcomitant use of DOACs and antiarrhythmic drugs versus concomitant use of DOACs and non-antiarrhythmic drugsSix studies compared concomitant use of any or specific DOACs and antiarrhythmic drugs versus concomitant use of any or specific DOACs and non-antiarrhythmic drugs regarding the risk of major or any bleeding (Table 1) [13, 17, 26, 27, 31, 35]. Two studies showed increased risks (HRs, 1.21 & 2.87) [17, 31], one study showed mixed findings depending on the antiarrhythmic drug and the subtype of major bleeding [35], two studies showed no differences in the risk [26, 27], while one study lacked the necessary statistical power [13]. Three studies assessed the risk of stroke/SE and the risk of all-cause mortality, respectively, showing no differences in the risk [17, 27, 35].
Other comparisonsTwo studies compared concomitant use of apixaban and antiarrhythmic drugs (dronedarone or amiodarone) versus concomitant use of VKAs and the same antiarrhythmic drugs regarding the risk of major bleeding showing no differences (Table 1) [33, 34]. Analyses on the risk of stroke/SE and all-cause mortality either lacked the necessary statistical power or showed no differences. One study compared concomitant use of DOACs and amiodarone versus concomitant use of DOACs and flecainide or sotalol, showing a 42% increased risk of major bleeding, no difference in the r
Comments (0)