Rising rates of body image concerns in men
Over the past decade, research has consistently indicated rising rates of body image concerns among men, with muscularity-oriented eating behaviours (MOEB) emerging as particularly salient, especially among gay men [12]. Recent estimates suggest men now comprise up to 25% of individuals affected by eating disorders (EDs), with prevalence rates increasing faster than those observed among women [18]. This notable shift challenges traditional perceptions of EDs as predominantly female conditions, underscoring the need to reassess gendered assumptions in diagnosis and intervention. Indeed, according to the National Centre for Biotechnology Information [20], approximately 10 million men in the United States will experience a clinically significant ED during their lifetime.
Sexual orientation and male body image
Within this broader context, existing literature consistently demonstrates that gay men report higher levels of body image distress and MOEB compared to heterosexual men. For instance, a recent meta-analysis by Nowicki et al. [21] found that sexual minority men experience significantly greater body image disturbance and disordered eating symptoms than their heterosexual counterparts. These observed differences highlight the necessity of investigating unique patterns and psychological correlates of body image distress among diverse male populations [16]. These disparities likely stem from sociocultural and minority stress-related factors rather than inherent group characteristics, and it is critical to avoid attributing causality to gay communities themselves. As Simone et al. [28] note, pressures toward leanness and muscularity are experienced more intensely among gay men due to cultural appearance ideals and objectifying environments,however, these influences should be contextualized within broader societal and structural systems.
Clarifying key constructs: EDs, and MOEB
Throughout this manuscript, we clearly distinguish among key terms. The phrase EDs specifically refers to clinically diagnosable conditions outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), such as anorexia nervosa, bulimia nervosa, binge eating disorder, Other Specified Feeding or Eating Disorders (OSFED), and Unspecified Feeding or Eating Disorders (UFED), replacing the DSM-4 category Eating Disorder Not Otherwise Specified (EDNOS). “MOEB” explicitly describe dietary practices intended to increase muscle mass, encompassing behaviours that range from adaptive nutritional strategies to potentially maladaptive patterns. In discussing broader, subclinical eating-related problems, we use the term “disordered eating.” Clarifying these distinctions is critical, as MOEB represents a unique set of behaviours that traditional ED diagnostic criteria may inadequately capture, particularly among male populations.
Importance of exploring interrelationships among MOEB, MD, and EA
Understanding the interrelationships among MOEB, MD, and EA holds clinical and theoretical importance for several reasons. First, while these conditions frequently co-occur, they are typically studied separately, potentially obscuring patterns of comorbidity essential for comprehensive assessment and intervention [23, 32]. Second, elucidating the connections between these constructs can reveal common underlying vulnerabilities or transdiagnostic mechanisms—such as perfectionism, body surveillance, or emotional dysregulation—that could become treatment targets. Third, examining how associations vary by sexual orientation is vital for developing tailored screening protocols and treatments for specific populations [5]. Clinically, exploring these interrelationships enhances the potential for early identification and supports integrated treatment models addressing multiple interconnected concerns simultaneously, rather than treating each as an isolated issue.
To provide clearer theoretical grounding for our analytic approach, we conceptualize MOEB and MD as antecedents or contributing factors to compulsive exercise behaviour. Previous research and models—such as the Transactional Model of EA [6]—propose that EA often emerges as a maladaptive coping mechanism in response to body dissatisfaction, rigid eating beliefs, or appearance-focused goals. In this framework, EA is not a standalone pathology but part of a broader symptom cluster that includes disordered eating and body image concerns. Thus, our decision to model EA as the outcome variable reflects the theoretical understanding that compulsive exercise often functions as a behavioural strategy for regulating distress or compensating for perceived physique deficits associated with MD and MOEB.
Existing research and gaps
Although previous research indicates elevated vulnerability to body image concerns among sexual minority men, few studies have investigated how MOEB, MD, and EA co-occur in men—or how these relationships differ by sexual orientation. Addressing this gap is crucial, as understanding these associations can inform the development of targeted clinical screening tools, enhance early detection strategies, and guide effective intervention programs tailored specifically to the unique needs of diverse male populations, including sexual minority men.
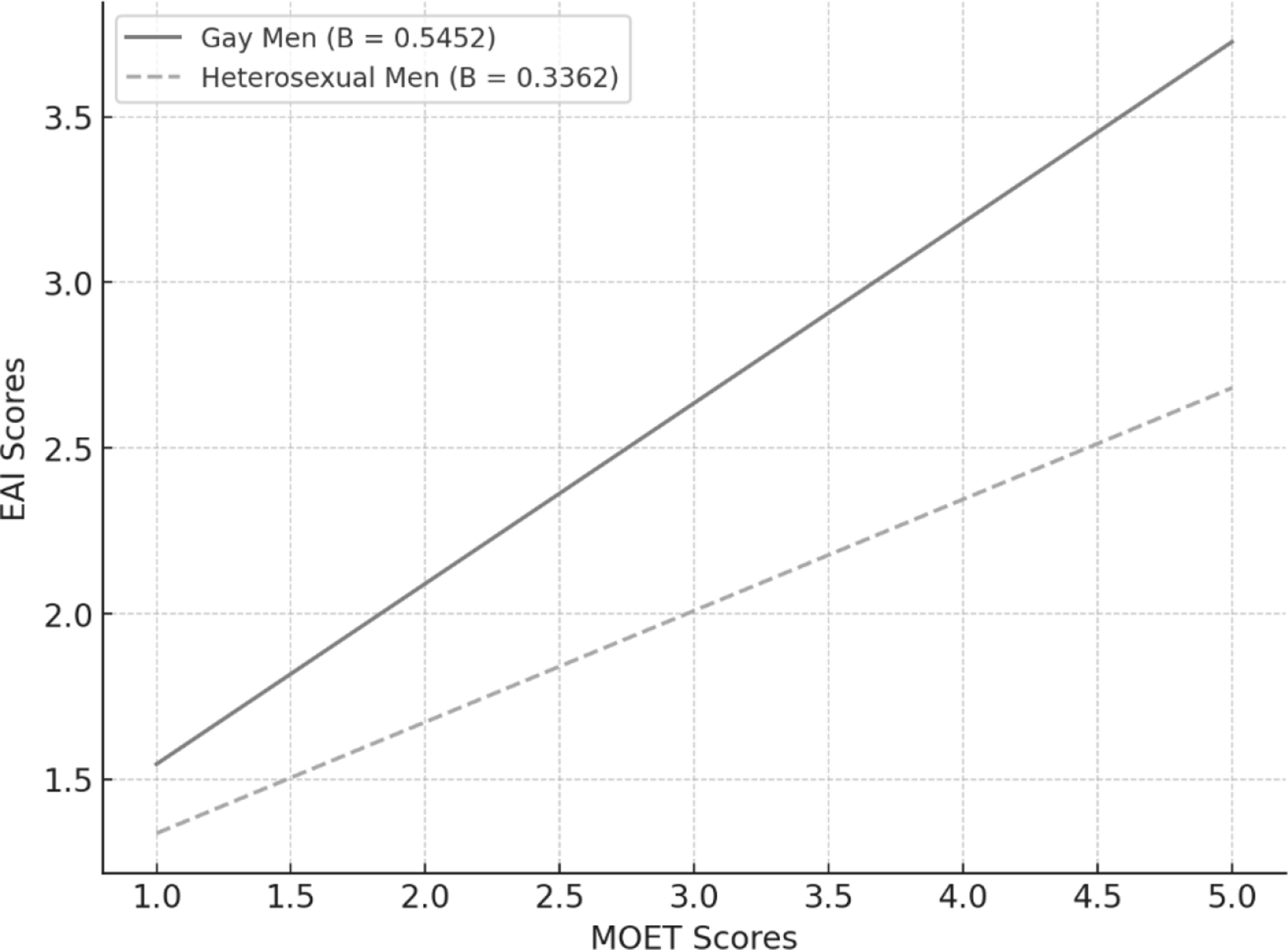
Our study extends Schmidt et al.’s [27] findings by directly comparing gay and heterosexual men, focusing explicitly on MOEB and EA as distinct but interrelated outcomes. Schmidt et al.’s study used general disordered eating and body dissatisfaction indicators in sexual minority men but did not assess EA or muscularity-specific eating patterns. In contrast, our study employs male-specific measures such as the MOET, MDDI, and EAI, offering more nuanced insights into male body image pathology. This comparative approach not only contextualizes the findings within broader clinical practice but also helps clinicians better identify and respond to at-risk individuals across different populations.
Although our study does not directly measure minority stress or underlying mechanisms, our comparative approach provides critical context for interpreting these associations and identifying directions for future research. We expect stronger associations among gay men due to increased exposure to sociocultural pressures such as minority stress, internalized stigma, and heightened appearance ideals [33]. Minority Stress Theory [15] and Objectification Theory [7] provide theoretical grounding for this moderation hypothesis.
These frameworks suggest that gay men may experience unique vulnerability to appearance-related pressures, increasing the likelihood that body image concerns will translate into disordered eating or compulsive exercise behaviours. According to the Transactional Model of EA, the interaction between personal vulnerabilities and sociocultural stressors—including those experienced more frequently by sexual minority men—may intensify the risk for maladaptive exercise patterns. Thus, the decision to test sexual orientation as a moderator is theoretically driven and consistent with emerging models of behavioural health disparities.
MD and EA in male populations
Men’s body image concerns are complex and multidimensional, encompassing traditional eating disorder symptomatology as well as recently recognized phenomena such as MD and EA. These issues are frequently reported among gay men, who may experience distinct sociocultural pressures related to masculinity and appearance. Although such contextual factors are widely discussed in the literature, the current study does not directly measure constructs such as minority stress or objectification experiences. Instead, our goal is to explore observable patterns of association among MD, MOEB, and EA across groups defined by sexual orientation, providing a foundation for future studies examining underlying mechanisms.
MD is a subtype of body dysmorphic disorder characterized by a preoccupation with muscularity and leanness [25, 26]. Individuals experiencing MD may perceive themselves as insufficiently muscular despite possessing above-average muscle mass. This distorted self-perception has been associated in previous research with behaviours including excessive weight training, dietary restriction, and anabolic steroid use [14]. Although our study does not explore the antecedents or underlying mechanisms of MD, existing evidence linking MD symptoms to muscularity-oriented eating behaviours and psychological distress in men [23] supports its inclusion in our investigation.
EA is characterized by compulsive engagement in exercise despite negative physical or psychosocial outcomes [2]. It may present in two forms: primary EA, where the addiction is focused solely on the act of exercising, and secondary EA, which is more directly linked to muscularity-oriented eating behaviours [17]. While the potential interplay between EA, MOEB, and MD remains under-researched, emerging studies suggest that these constructs may cluster together, particularly among men [32]. Our study aims to examine these associations empirically without assuming causal directionality.
Study objectives and hypotheses
The current study investigates the associations among MOEB, MD, and EAin gay and heterosexual men, examining specifically whether sexual orientation moderates these relationships. Based on previous literature and theoretical frameworks discussed earlier, we hypothesized that (1) gay men would report higher levels of MOEB and MD symptoms compared to heterosexual men; (2) gay men would also report higher levels of EA compared to heterosexual men; (3) higher levels of MOEB and MD would significantly predict higher levels of EA across the full sample; and (4) sexual orientation would moderate the relationships between (a) MOEB and EA and (b) MD and EA, with stronger associations expected among gay men due to increased sociocultural pressures and minority stress.

Comments (0)