In this retrospective observational study, we established reference intervals for neutrophil, monocyte, and lymphocyte CPD in newborns, defining ranges from birth to postnatal day 28 across different gestational age groups. In an exploratory analysis of sepsis and NEC cases, we identified early alterations of most CPD parameters, suggesting that CPD could provide attractive biomarker candidates for the diagnosis of sepsis and NEC.
Previous studies have shown that hematological parameters vary with gestational and postnatal age, highlighting the importance of establishing reference intervals in newborns.23,24,25,26,31 Our study contributes to this body of knowledge by establishing reference intervals for CPD in a large cohort of hospitalized newborns. While reference intervals for CPD have been established in the adult population, to our knowledge, this is the first report on neonatal intervals.32,33,34 Furthermore, our findings highlight the considerable impact of gestational and postnatal age on neutrophil, monocyte, and lymphocyte CPD, revealing variations in complexity, fluorescence, and size across gestational age and throughout the neonatal period, contributing to increase our understanding of the developmental biology of blood leukocytes.
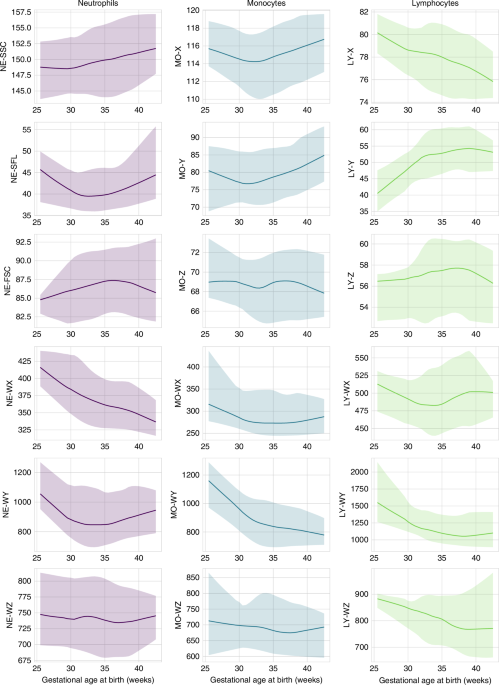
Reference intervals for CPD parameters, which capture the evolution of leukocyte subpopulation morphology and functionality, reveal trends that differ from those of absolute cellular counts.24,25,26 Across the three CPD subpopulations assessed in our study, we observed a reduction in the distribution width of most CPD parameters with increasing gestational age, probably indicating enhanced cellular homogeneity in more mature infants. In line with those findings, CPD distribution width reference intervals in adults are lower than those of full-term neonates, suggesting a developmental process towards greater cellular homogeneity.32,33,34 In contrast, each mean CPD parameter exhibited its own unique pattern of change with both gestational and postnatal age.
NE-SSC, an indicator of neutrophil cell complexity and granule content, progressively increases with gestational but not postnatal age, indicating that the maturation process of neutrophils could depend mainly on gestational age at birth.35 The reference intervals in full-term newborns are close to those observed in adults.32,33,34 NE-SFL, which depends on the RNA/DNA neutrophil content ratio, may reflect cellular immaturity or activation.36,37 In our results, NE-SFL shows complex changes across gestational and postnatal age, with reference intervals in full term newborns closely aligning with adult ranges, likely reflecting the dynamic interplay between neutrophil maturation and immune system activation in early life.32,33,34,35,38 NE-FSC, proportional to neutrophil size, also shows a complex pattern of changes with increasing gestational and postnatal age. As NE-FSC values are higher in adults, it could indicate that the maturation process in terms of neutrophil size extends beyond the neonatal period.32,33,34
MO-X, reflecting monocyte cellular complexity, exhibits complex variations according to gestational age at birth. Values in term newborns approach those observed in adults.32,33,34 MO-Y, which depends on the RNA and DNA content of monocytes, exhibits a complex pattern in relation to gestational age at birth. Neonatal values remain lower than those observed in the adult population, likely reflecting a reduced transcriptional ability in neonates, particularly in preterm infants.32,33,34,39 MO-Z, reflecting monocyte cellular size, remains relatively stable across different gestational and postnatal ages, aligning closely with the reference ranges established in adults.32,33,34
LY-X, indicating lymphocytic complexity and granularity, decreases with increasing gestational age at birth, while it remains relatively stable with increasing postnatal age. Adults present even lower reference ranges.32,33,34 LY-Y, which depends on RNA and DNA content, increases with gestational age at birth and subsequently exhibits a complex evolution during the neonatal period. Term newborns exhibit values comparable to adult ranges.32,33,34 This variation could be related to phenotypical changes, such as increased expression of transcription factors in more mature infants at birth and the rise in cytotoxic T/NK lymphocytes and B lymphocytes during the first postnatal weeks.40,41 LY-Z, reflecting the size of lymphocytes, remains stable across gestational ages at birth and throughout the neonatal period, with term neonates showing values lower than those observed in adults.32,33,34
In our exploratory analysis on sepsis and NEC, most CPD parameters show substantial differences between cases and neonates in the reference group at the onset of disease. NE-SFL and LY-X exhibit the highest diagnostic accuracy, which is superior to classical hematological parameters and CRP. NE-SFL has the strongest diagnostic potential for sepsis/NEC. The higher NE-SFL might be related to increased transcriptional activity in immature or activated neutrophils mobilized into peripheral blood during sepsis.36,37 Studies conducted in adults have identified a potential of NE-SFL to detect sepsis at the onset of symptoms, and a correlation with bacterial load.36,42,43,44,45 A pilot study showed higher NE-SFL in critically ill children with sepsis compared to those without infection.46 Few studies have investigated LY-X in sepsis, with conflicting results in adults.42,43,44 Our exploratory analysis identifies high LY-X, in newborns with sepsis/NEC, suggesting a potential role as a biomarker.
In line with previous studies, leukopenia, neutropenia, and elevated I/T ratio have low to moderate accuracy in detecting sepsis and NEC, with high specificity but low sensitivity and PPV.27,28,29,47 Similarly, CRP has moderate sensitivity and specificity, consistent with published findings, underscoring its limited utility as a standalone diagnostic marker.48,49 In our exploratory analysis, NE-SFL and LY-X provide a better trade-off between sensitivity and specificity, further supporting the potential of CPD parameters in the diagnosis of neonatal sepsis and NEC. Moreover, CPD offer several benefits compared to classical biomarkers. Since they are automatically generated with the CBC, they are available 24/7 without additional costs or extra sampling, a crucial feature for preterm newborns. In addition, as numerical data, CPD provide an objective, accurate, and faster alternative to manual differential counts.18
In our study, we evaluated three multivariate logistic regression models integrating the most accurate biomarkers from our univariate analysis, namely NE-SFL, LY-X, leukopenia, and CRP. While measuring multiple biomarkers concurrently has shown promise in diagnosing sepsis in adults, evidence supporting its use in neonatal sepsis remains limited.43,50,51,52,53,54 In our exploratory analysis, these models slightly improve specificity and PPV compared to NE-SFL alone, but the overall performance remains mostly unchanged, with PPV still limited.
This study benefits from its large population of hospitalized newborns, ensuring comprehensive and representative data. Reference intervals were rigorously defined following recommendations from neonatal literature.23 The use of mixed-effects models allowed to analyze the effects of gestational and postnatal age, while accounting for interindividual variability. This study has limitations. Although our large cohort provided an effective basis for determining reference intervals for CPD parameters, the small number of sepsis/NEC cases restricted our ability to evaluate their diagnostic performance, allowing only exploratory analyses in the early identification of sepsis/NEC. The monocentric and retrospective design limits the generalizability of the findings. As 30% of patients were excluded due to missing CPD parameters, this could have introduced some bias in our analyses. Due to the lack of prenatal data in our cohort, we could not exclude infants born from mothers with conditions known to influence neonatal leukocyte parameters. To minimize the impact of these potential confounders, we excluded neonates with any documented neutropenia.


Comments (0)