Guidelines recommend endoscopic ablation in select UTUC patients, including those with non-invasive tumor stage, low-grade histology, and tumor size < 2 cm [6, 7]. However, no large-scale population-based study validated that endoscopic ablation does not undermine CSM-free rates in select UTUC patients. We addressed this knowledge gap and made several noteworthy observations.
First, UTUC is a rare cancer [1, 6, 7]. Among all stages of UTUC, those considered for endoscopic ablation, namely localized non-invasive low-grade UTUC with tumor size < 2 cm represent even a rarer entity. Specifically, Upfill-Brown et al. relied on the National Cancer Database (NCDB) and identified 851 patients [15]. This highly select patient cohort accounted only for 2.0% of the overall population of 43,036 UTUC patients within the NCDB between 2004 and 2012 [15]. In the current study, we identified 249 localized non-invasive low-grade UTUC patients with tumor size < 2 cm over a 21-year period within the SEER database (2000–2020). In consequence, select UTUC patients should ideally be included in multi-institutional studies or large population-based analyses, as was done in the current study, when cancer-control outcomes represent the outcome of interest in this small subgroup of a rare primary tumor.
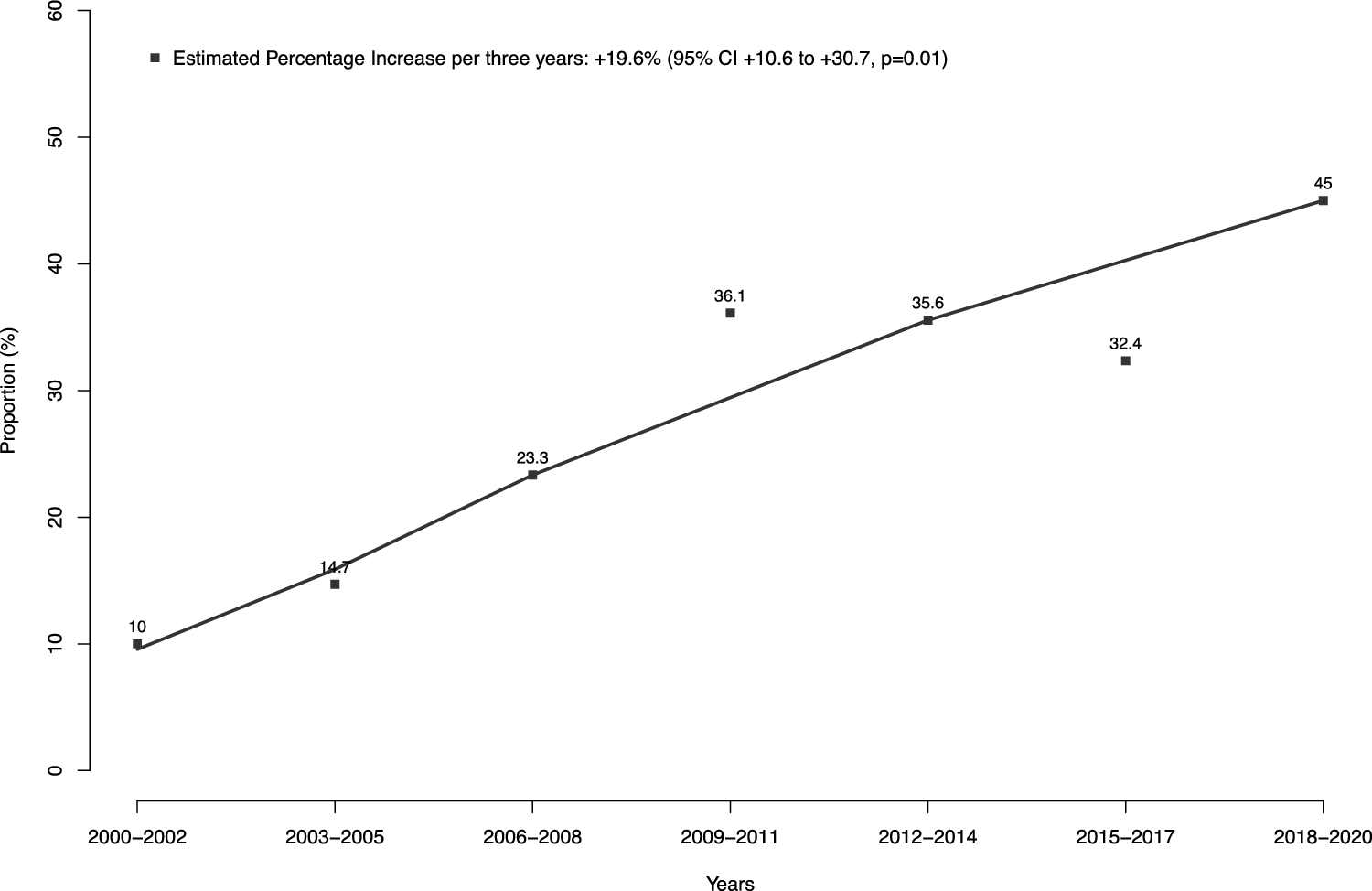
Second, we stratified the study cohort of localized non-invasive low-grade UTUC with tumor size < 2 cm according to surgical treatment type: endoscopic ablation vs. radical nephroureterectomy. Of 249 patients that fulfilled the above selection criteria, as many as 66 benefited from endoscopic ablation. The proportion of patients having benefitted from endoscopic ablation between 2000 and 2020 within the current study is only 27%, which is lower than 38% previously reported by Upfill-Brown et al. based on NCDB [15]. However, the rate of endoscopic ablation increased to 45% in the three most recent years of the current study (EPI + 19.6%; p = 0.01). This observation is highly encouraging. Unfortunately, it cannot be directly compared to the analysis of Upfill-Brown et al. since NCDB data addressing the select subgroup of patients with localized non-invasive low-grade UTUC with tumor size < 2 cm were not tabulated according to years of diagnosis [15]. However, tabulations of endoscopic ablation rates over time in a cohort that relied on wider selection criteria than used in the current study also increased over time [15, 19]. These increases might be explained, among other factors, by broader indication for endoscopic ablation in recent UTUC guidelines [15], technical advances in endourology [20], as well as greater availability of endourological experts than in historical years. Additionally, the increasing rates of endoscopic ablation also indicate increasing acceptance over time of guideline recommendations within the urologic community.
Third, we identified important differences in baseline characteristics between endoscopic ablation vs. radical nephroureterectomy patients. Specifically, endoscopic ablation patients were older (median age 77 vs. 73 years) and harbored smaller tumors (median tumor size 1.0 vs. 1.5 cm) than their counterparts treated with radical nephroureterectomy. Based on these differences, it is essential to rely on propensity score matching (endoscopic ablation vs. radical nephroureterectomy patients) to reduce or ideally eliminate uncontrolled confounding or bias originating from patient and tumor characteristics, as was done in the present study. After detailed propensity score matching for age at diagnosis and tumor size that resulted in minimal cohort differences, 66 of 66 (100%) endoscopic ablation and 66 of 183 (36%) radical nephroureterectomy patients remained. Indeed, the use of propensity score matching virtually perfectly eliminated meaningful differences between endoscopic ablation vs. radical nephroureterectomy patients. However, other patient characteristics, such as performance status and comorbidities (e.g. cardiovascular disease or chronic kidney disease), which may influence treatment decision-making due to elevated risk of perioperative complications, could not be considered as covariates in the present study, as the current version of the SEER database does not provide this information [21]. Moreover, an important attrition in the size of the nephroureterectomy cohort was also recorded, without concomitant loss of observations within the endoscopic ablation cohort. Such phenomenon unfortunately invariably accompanies the use of propensity score matching.
Fourth, we addressed CSM as cancer-control endpoint. Specifically, we tested for CSM differences in localized non-invasive low-grade UTUC patients with tumor size < 2 cm treated with endoscopic ablation vs. radical nephroureterectomy. In survival analyses that relied on propensity score matched cohorts of endoscopic ablation and radical nephroureterectomy patients (66:66), ten-year CSM rates were 15.7% after endoscopic ablation vs. 13.9% after radical nephroureterectomy (CSM Δ1.8%; p = 0.9). In competing risks regression models that accounted for OCM and relied on propensity score matching as well as additional multivariable adjustment, these rates translated into a HR of 1.10 (95% CI 0.42–2.87; p = 0.9). Since previous studies either did not meet the guideline-defined inclusion criteria for low-risk UTUC patients [12,13,14] or, if they did, addressed different study endpoints, such as OM instead of CSM [15], no direct comparison of the current results with previous studies can be made. However, these results among select low-risk UTUC patients convincingly illustrate that CSM rates, which may be expected after endoscopic ablation, are clearly not inferior to those observed after radical nephroureterectomy. Patients and clinicians should consider that endoscopic treatment is associated with additional benefits compared to radical nephroureterectomy, such as shorter hospital stay, fewer Clavien–Dindo high-grade postoperative complications, and less decline in estimated glomerular filtration rate (eGFR) [8]. Furthermore, progression to dialysis-dependent kidney disease is associated with a decrease in quality of life as well as higher health costs [22]. In consequence, endoscopic ablation may be offered and preferred not only at centers of excellence with established track records of kidney-sparing management in low-risk UTUC patients, but also in population-based settings when technically feasible.
Finally, the current study also addressed OCM in localized non-invasive low-grade UTUC patients with tumor size < 2 cm as a secondary endpoint. Absolute ten-year OCM rates of 46.3 vs. 57.9% (ΔOCM 11.6%; p = 0.5) were recorded after endoscopic ablation vs. radical nephroureterectomy. These rates illustrate that the majority of mortality events represented non-cancer-related deaths. Specifically, of all deaths in patients treated with endoscopic ablation 27 of 35 were OCM events. Similarly, of all deaths in patients treated with radical nephroureterectomy 35 of 43 represented OCM events. The phenomenon of higher OCM than CSM rates may be explained in several ways. First, low CSM rates may be attributed to the low-grade nature of UTUC examined in the present study, making it more likely to die from other health conditions (e.g., cardiovascular diseases) before UTUC progresses to a fatal stage. Second, UTUC occurs in elderly patients. Age-related decline and frailty make the UTUC patient cohort susceptible to other causes of death. Third, treatment-related morbidity may be another explanation. However, the observation of lower CSM and higher OCM rates applies to both treatment groups (endoscopic ablation and radical nephroureterectomy). Therefore, it is more likely that the observation of lower rates of CSM and higher rates of OCM may be attributed to the nature of low-risk UTUC, rather than to differences between the two patient cohorts or delivered treatments. However, the SEER database is not detailed enough to allow more definitive assessment of those associations. In consequence, the proposed explanations remain preliminary at its best.
Nevertheless, lack of specific CSM consideration in previous analyses may have resulted in erroneous consideration of the majority of deaths in analyses that attempted to quantify cancer control outcomes. Possibly, in NCDB analyses, where endoscopic ablation was interpreted as a treatment option with worse survival outcomes compared to radical nephroureterectomy, the methodological flow where OM instead of CSM is considered as study endpoint, may have contributed to this potential misinterpretation [15]. This potential misinterpretation of treatment comparisons when OM is used instead of CSM as the study endpoint has already been demonstrated for other treatment comparisons, such as trimodal therapy vs. external beam radiotherapy in non-metastatic urothelial carcinoma of the bladder, as well as radiotherapy vs. partial penectomy in localized penile cancer [23, 24]. In these cases, reliance on OM alone would have led to misleading conclusions regarding treatment efficacy, as differences in mortality were influenced by competing risks rather than cancer-related deaths. Therefore, CSM represents an essential survival endpoint in treatment comparisons in localized non-invasive low-grade UTUC patients with tumor size < 2 cm since CSM only accounts for a small proportion of OM events and the competing and potentially confounding OCM effect accounts for the remaining majority of OM events.
Taken together, the proportion of patients undergoing endoscopic ablation increased from 10 to 45%, reflecting growing confidence in endoscopic management for select UTUC patients. After strict methodology, including propensity score matching, multivariable adjustment, and accounting for OCM, CSM rates after endoscopic ablation vs. radical nephroureterectomy neither showed statistically significant or clinically meaningful differences. These observations among North American UTUC patients provide a large-scale contemporary validation of the current European guideline recommendations to identify low-risk UTUC patients eligible for endoscopic ablation.
Despite its novelty, the present study is not devoid of limitations. First, the current study shares the limitations of all UTUC studies that used an observational study design and a retrospective database, such as SEER [2, 12, 13, 25,26,27,28,29,30,31], NCDB [15, 19] or multi-institutional databases [8, 10, 14, 32]. Even after strict and systematic adjustment for confounders and biases relying on propensity score matching, multivariable adjustment and accounting for OCM or CSM in competing risks regression models, a potential for selection biases remained. Second, despite the large scale of the SEER database, the sample size within the SEER database is limited due to the rarity of localized non-invasive low-grade UTUC with tumor size < 2 cm. Therefore, subgroup analyses according to specific endoscopic procedures, such as electrocautery or laser ablation were not possible. Third, the current study focuses on the comparison of endoscopic ablation vs. radical nephroureterectomy. Other kidney-sparing surgical techniques, such as partial nephrectomy or segmental ureterectomy, which may also be considered in select UTUC patients were not included [33]. Fourth, patient clinical characteristics, such as performance status or comorbidities (e.g. cardiovascular disease or chronic kidney disease) are not available in the current version of the SEER database. Therefore, these patient characteristics that may have influenced treatment decision cannot be considered as matching variables or for further adjustments in multivariable models in the present study [31]. However, lack of comorbidities was at least in part addressed with competing risks regression analyses that accounted for OCM since most important comorbidities result in OCM. Fifth, the SEER database only provides a limited amount of detail regarding tumor characteristics and procedural details. Unfortunately, the number and frequency of endoscopic ablations cannot be analyzed. Likewise, drug-specific information regarding postoperative or adjuvant intravesical instillation therapies is not available. Moreover, the current version of the SEER database only provides tumor morphology and stage at initial diagnosis. Therefore, data on non-organ-confined tumors (pT3/pT4), positive lymph nodes (pN +), and positive surgical margins (R1) are unavailable for endoscopic ablation patients who later underwent radical nephroureterectomy. Additionally, detailed information regarding tumor appearance, such as tumor focality, pathological characteristics, such as urinary cytology, as well as clinical characteristics, such as hydronephrosis are unknown. Nevertheless, all available risk stratification variables for non-metastatic UTUC patients, provided by the SEER database, were considered as inclusion criteria for the selection of the current study cohort. Finally, the SEER database does not include earlier cancer-control endpoints than CSM and OCM. In consequence, other study endpoints that could be equally as interesting as CSM, such as intravesical recurrence or metastasis could not be addressed within the present database.



Comments (0)