
Remember me



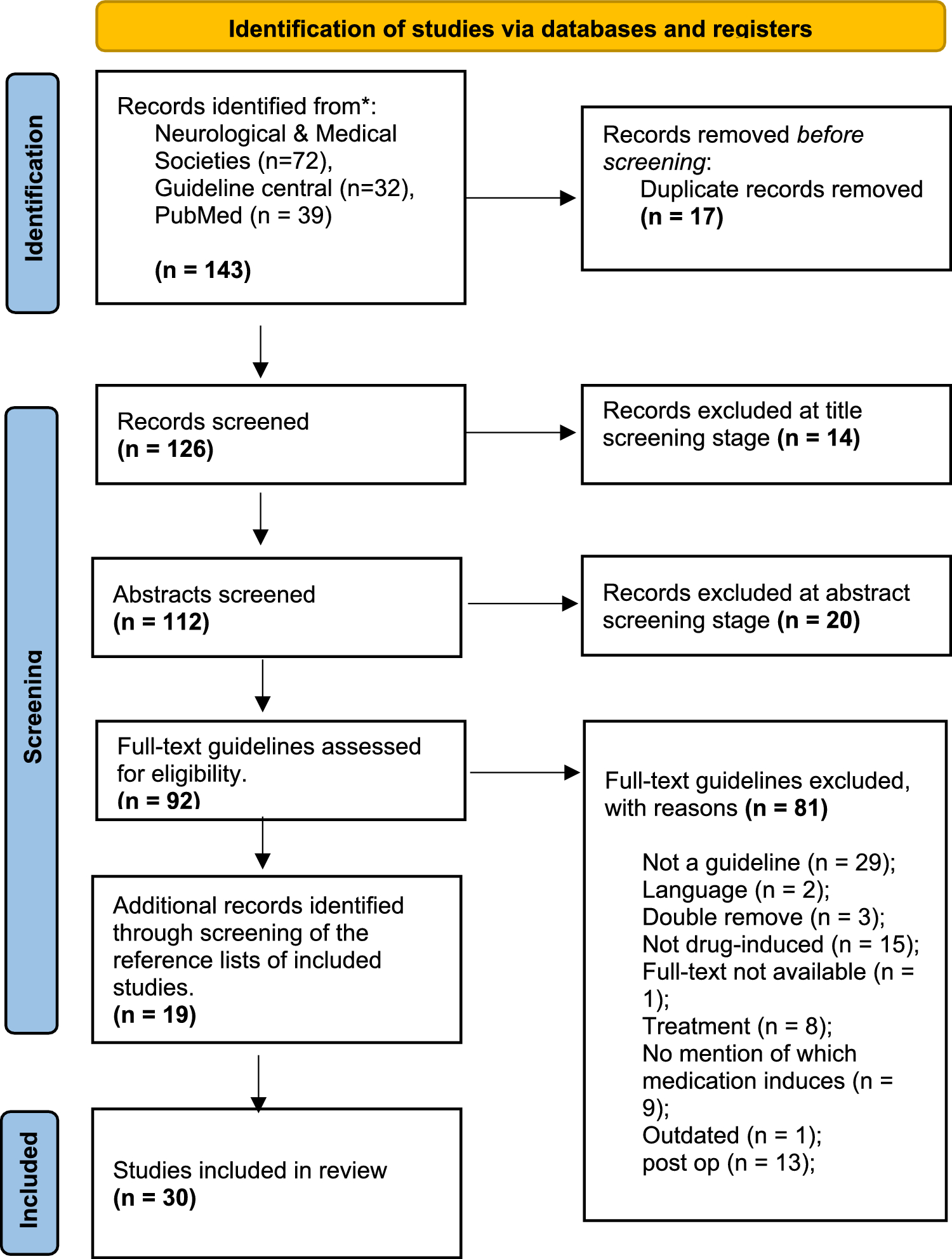

The literature search yielded 143 guidelines. After screening, 30 guidelines were included (Fig. 1). Guidelines were published between 2003 and 2023 the majority of which originated from North-America (n = 11), UK (n = 8), Australia and New-Zealand (n = 5), with one paper each from Denmark, Switzerland, Iceland, Japan, India and one from a global expert group.
Fig. 1
Adapted from: [13] Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021;372:n71. https://doi.org/10.1136/bmj.n71
PRISMA flowchart showing the identification, screening and selection of delirium guidelines across neurological and medical professional organizations, Pubmed and Guideline Central.
Guideline characteristicsGuidelines are either published by national and global professional organizations (n = 21; 70%) or hospitals (n = 8; 26,7%), with one published by American and Australian experts (n = 1; 3,3%). As a result, publications are applicable to a range of primary (n = 19; 63,7%) or secondary (n = 11; 36,3%) healthcare practices (Table 1).
Table 1 : Summary of guideline characteristics and qualityGuideline qualityMost guidelines were deemed to be designed, conducted, and reported with a high quality based on the AGREE II instrument (n = 19, 63,3%) [21]. Only two guidelines could not be assessed as they are single-page care pathways or position statements [24, 33]. No guideline was excluded based on quality (Table 1).
Medication at risk of inducing deliriumCausative medication mechanismA summary of reported mechanisms through which medication can contribute to the development of delirium in adults is summarised in Table 2
Table 2 Summary of reported mechanism or risk through which medication can contribute to the development of a delirium in adultsMedication at risk of causing a deliriumA total of 140 individual medication were listed across 30 guidelines. The medication classes who are cited most often (> 60% of the time) included sedatives (n = 24/80%), opioids (n = 22/73,3%), psychoactive drugs (n = 21/70%) + anti-convulsants (n = 14/46,7%), anti-cholinergic agents (n = 20/66,7%) and anti-histamines (n = 18/60%) (Table 3).
Table 3 Summary of all 140 individual medication reported to carry a risk of causing a delirium in adults organised by ATC CodeSteroids (n = 16/53,3%) anti-depressants (n = 12/40%), H2-Antagonists (n = 12/40%), anti-hypertensives (n = 11/36,7%), anti-parkinsonian (n = 11/36,7%), anti-arrhythmics (n = 10/33%), antibiotics (n = 9/30%) and non-steroidal anti-inflammatory agents (NSAIDs) (n = 8/26,7%) were also mentioned (Supplementary Table 4).
SedativesAntipsychotics:Delirium caused by antipsychotics depends on the dose of the drug and the age of the patient [34]. While antipsychotics are considered a direct risk factor [35] especially in palliative care [31], low dose haloperidol, quetiapine or risperidone may be used as pharmacological treatment for hyperactive delirium where behavioral problems (e.g. severe agitation) and emotional disturbance (e.g. severe anxiety) persist [36]. In older people, caution must be observed due to their side-effect profile, including extrapyramidal symptoms, sedation, anticholinergic effects including increased confusion, cardiovascular effects, and tardive dyskinesia [37]. Antipsychotics reduce the efficacy of anticholinesterase inhibitors (AChEIs) [38] and may trigger or aggravate delirium [39,40,41].
Due to the potential for harm and insufficient evidence for the efficacy of antipsychotics in the prevention and treatment of delirium, these medications should be administered at the lowest effective dose and for the shortest period of time in patients who are severely agitated and/or at risk of harming themselves and/or others [42]. The use of first-generation antipsychotics can be associated with neurological side effects and QTc prolongation [40]. The use of haloperidol and risperidone for agitation/psychosis in a dosage of 0.25–4 mg/day and 0.5–2 mg/day respectively carries the following cautions: EPS symptoms (+ + +), QTc prolongation (+ + , more with IV use) and orthostatic hypotension ( +) [36]. The use of haloperidol and risperidone should be avoided when treating mild delirium in palliative patients should be avoided [31]. Olanzapine, thioridazine, fluphenazine, prochlorperazine, perphenazine, trifluoperazine and chlorpromazine were all identified as medications that carry a risk of inducing cognitive impairment and/ or delirium [36, 43].
Benzodiazepines:Benzodiazepines markedly increase the odds of developing delirium in hospital/surgical wards, in residential/ community care (OR 3.0 95% CI 1.3 to 6.8) and palliative patients [37, 40, 44]. The higher the dose and the longer acting the benzodiazepine, the greater the risk [45]. Benzodiazepines should only be used for alcohol withdrawal, acute seizure management and in palliative sedation to reduce seizure risk, myoclonus, muscle tension, or acute agitation crisis [31, 44].
In addition to evidence that benzodiazepines can trigger or aggravate delirium in older adults, benzodiazepines and other sedative-hypnotics significantly increase the risk of morbidity (e.g. falls, delirium and hip fractures) and mortality [39, 46]. They should never be used as a first choice to treat insomnia, agitation, or delirium [47]. Dementia patients taking benzodiazepines [37, 45] have an increased risk of developing a delirium, falls, worsening agitation, disorientation, stroke, and premature death [47].
Short-acting benzodiazepines can cause cognitive impairment [43]. Lorazepam (medium acting) should only be used in patients with alcohol withdrawal or terminal delirium [33, 36], while alprazolam and oxazepam (medium acting) are not flagged as toxic as lorazepam [43]. Diazepam, clobazam and chlordiazepoxide (long acting) are all considered directly delirogenic drugs [23].
Z-substances/ hypnotics:Zolpidem, a non-benzodiazepine Z-drug was shown to cause confusion, disorientation, and delirium [34, 48]. No other Z-drugs were described.
Psychoactive drugs and antimanic agents:Most guidelines stated that haloperidol is the treatment of choice to manage delirium, however long-term haloperidol use is considered a delirium risk factor [40, 43]. The guideline from the Registered Nurses Association of Ontario (2003), states that thioridazine, fluphenazine, prochlorperazine, trifluoperazine, and perphenazine cause cognitive impairment in older patients. So do chlorpromazine, olanzapine and phenothiazine [45]. Since lithium has a narrow therapeutic window, serum lithium levels should always be monitored especially in patients with renal impairment [34, 40]. Lithium poisoning should be suspected if the patient is on combined treatment of lithium and other antipsychotics. Lithium is therefore considered an indirect risk factor for delirium [35].
OpioidsPethidine [34] and meperidine [28] are the opioids most likely to precipitate a delirium while oxycodone seems least likely [34, 44]. Morphine or fentanyl were not significantly associated with delirium [44]. However transdermal fentanyl patches are contraindicated for non-cancer pain in opioid naïve patients as they pose a significant risk in the precipitation of delirium [37]. Codeine [23], dihydrocodeine [43], propoxyphene [43] and hydromorphone [28] all carry a reported delirogenic risk, with buprenorphine causing excessive drowsiness when combined with alcohol or central nervous system depressants [33]. Combining tramadol with other drugs that affect serotonin levels should be avoided [34].
Psychoactive drugsAnti-convulsantsPhenobarbital, primidone, and clonazepam cause more cognitive impairment than valproic acid, carbamazepine, and phenytoin [34]. One causative mechanism could be the impact on rapid eye movement (REM) sleep or sleep fragmentation of carbamazepine, phenytoin, and phenobarbital [23]. Mysoline is cautioned in palliative care patients [28], while the effects of pregabalin, gabapentin, lamotrigine, topiramate, and valproate are not mentioned.
Anti-cholinergic and antimuscarinic medicationsMost guidelines state that drugs with anticholinergic activity increase the risk of delirium in older patients. They reduce the efficacy of AChEIs while also causing sedation, cognitive impairment, delirium, and falls [36, 38].
Reported anticholinergic medication included belladonna alkaloids [35, 40, 54], homatropine [43], glycopyrrolate
[32], promotility agents [28, 45, 51], and tolterodine [28, 34, 45]. Only two antimuscarinic agents with an increased risk of precipitating a delirium were reported, atropine [23, 35, 43] and hyoscine [23].
AntihistaminesFirst-generation antihistamines such as brompheniramine, hydroxyzine, promethazine and dimenhydrinate carry a higher delirogenic potential compared to newer generations of antihistamines [34, 40, 42, 43], as they cross the blood–brain barrier more readily. Diphenhydramine, in particular should not be administered to prevent or treat delirium [55]. Loratadine and meclizine also exhibit an anticholinergic potential [43].
Therapeutic AlternativesTherapeutic alternatives were only provided by three publications [30, 33, 52]. Only one comprehensive best practice guideline published by the Nurses’ Association of Ontario (2016) [30] offers more comprehensive suggestions. In most cases a switch to a newer generation drug is suggested. Specific dosing recommendations are never provided (Table 4).
Table 4 Suggested alternative medication provided in patients with a high risk of deliriumDelirium in dementia patientsPharmacological measures for the management of delirium in dementia patients must not be considered unless the patient’s behavior has been assessed as posing a danger to themselves or others and if non-pharmacological interventions have failed to be effective. The emphasis should be on regular rather than when required medication [41] (Table 5).
Table 5 Summary of drugs and cautions for medication used in delirium and dementia. Adapted from [41] University Hospital Birmingham NHS, 2015 & James C. et al., 2020)
Comments (0)