Study design and study population
We included all primary small head MoM and CoP THAs performed between 03/1998 and 06/2011 at a large University Hospital. Since March 1996 all patients undergoing a THA are prospectively enrolled in the hospital-based arthroplasty registry. Completeness of recording of THAs is > 99% based on validation against the hospital’s diagnosis coding system, completeness of revision capture is > 96% based on data from the Swiss national joint registry (SIRIS). In a previously published article [23], we evaluated the results up to 12 years after surgery for these prostheses, end of follow-up being 31 December 2012. We updated the outcomes of this cohort with a follow-up until 31 December 2022. THAs performed for fracture or metastatic disease were excluded. Overall, 2785 patients met the inclusion criteria, after exclusion of 47 patients who had refused to consent, 3257 primary THAs in 2738 patients were included, 864 MoM and 2393 CoP THAs. The hospital-based arthroplasty registry was approved by the ethics committee of our institution (reference no. CER: 05–017 (05-0419)).
Exposure
All THAs received the same cup, a Morscher press-fit, uncemented, and monoblock acetabular cup (Zimmer Ltd, Winterthur, Switzerland). According to surgeon’s preference either a metal-on-metal bearing or ceramic-on-polyethylene bearing was used. Both types of bearings were available during the inclusion period. The implants were described as follows in our previously published paper [23]. The uncemented monobloc Morscher press-fit acetabular component (Zimmer Ltd, Winterthur, Switzerland) was used for all patients. This has a flexible titanium mesh shell backing which is bonded directly to an outer ultrahigh-molecular-weight polyethylene (UHMWPE) surface to eliminate the potential for backside wear. Two types of bearing were used according to surgeon preference. One was a metal-on-metal (MoM) bearing (Metasul, Zimmer Ltd) composed of a high-carbon (N 0.2%) cobalt–chromium alloy 28 mm femoral head which articulates with a high-carbon (N 0.2%) cobalt-chromium alloy inlay embedded into the UHMWPE liner. The second choice was a conventional UHMWPE bonded directly to the titanium mesh shell, combined with a third generation alumina ceramic 28 mm (Sulox, Zimmer Ltd) diameter head (CoP bearing). The acetabular components were sterilized by gamma irradiation in an inert atmosphere. The cemented stems included the Müller straight stem and the Virtec stem, both manufactured from Protasul-10 alloy (CoNiCrMo) (both Zimmer). The uncemented stems were the Spotorno CLS, Protasul-100 titanium alloy or the Wagner Conus, Protasul-64 titanium alloy (both Zimmer). For cemented stems, gentamicin-loaded bone cement was used, and cementing was performed using a third-generation technique.
Outcomes
The following outcomes were assessed: all-cause revision, presence of ALTR at revision, any other reoperation, prosthetic joint infection, dislocation, periprosthetic fracture, and mortality. Revision surgery was defined as any change to a component of the arthroplasty (cup, head, and/or stem), while reoperation included any type of surgery not involving a change of component of the arthroplasty (for instance: arthroplasty irrigation/debridement, osteosynthesis, abductor reinsertion). ALTR was defined based on the perioperative findings and pathology report. Periprosthetic fracture included any fracture diagnosed postoperatively. Dislocation included any diagnosis for dislocation.
Covariates
The following covariates were evaluated: age, sex, preoperative Body Mass Index (BMI), American Society Anaesthesiology (ASA) score, comorbidity count (beside osteoarthritis), diabetes (present or absent), smoking status (never vs. ever-smoker), diagnosis (primary vs. secondary osteoarthritis), stem fixation (cemented vs. uncemented), and Charnley score. Comorbidity count was classified in less than four or ≥ 4 [24]. Ever smokers included former and current smokers.
Data collection
Patients included in the local hospital-based arthroplasty registry have their information on preoperative status and surgical intervention routinely documented by the operating surgeon on specific designed data collection forms. Information about co-morbidities is retrieved from anesthesia records and discharge summaries by a medical secretary. Outcomes (all-cause revision, any other reoperation, PJI, dislocation and periprosthetic fracture) are collected by the operating surgeon or during the telephone interview if performed outside of our hospital [25].
Statistics
Continuous variables were assessed for normality and reported as mean with standard deviation and compared with the t-test. Categorical variables were reported as proportions. To compare the two bearing surface groups Pearson Chi-Square tests was used.
To compare the outcomes, incidences rates were calculated and expressed in person-years. The person-time for the outcomes was the length between date of surgery and the outcome, revision for any reason, loss of follow up, death, or end of follow up (December 31, 2022) whatever came first. Unadjusted and adjusted hazard ratios (HR) with 95% confidence intervals (CI) were calculated with a Cox regression model. Adjustment was performed for sex, age at surgery, diagnosis, type of stem fixation, number of diseases, BMI, ASA score and smoking status.
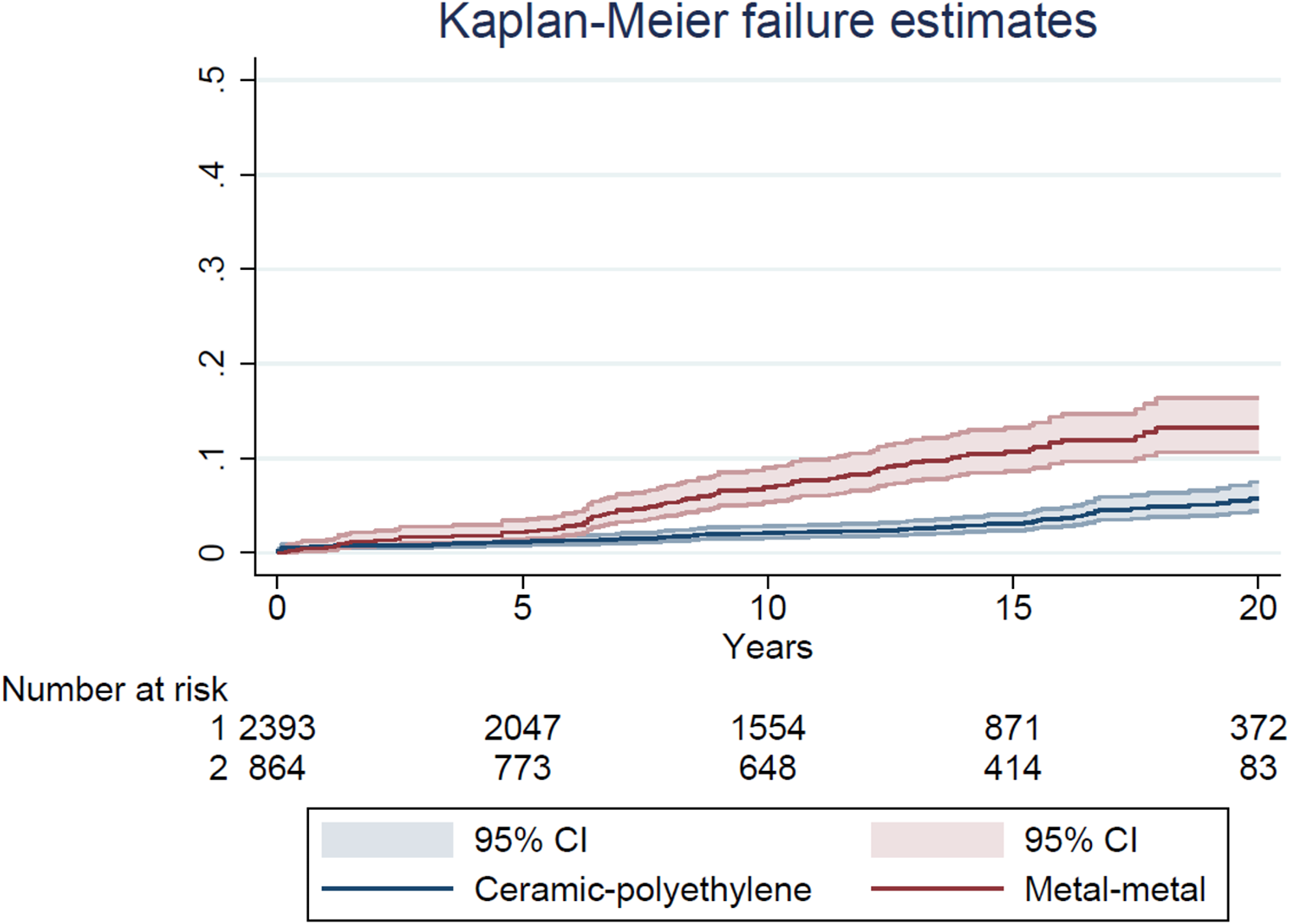
The cumulative risks of all-cause revision (CRR) were visualized by bearing surface using Kaplan-Meier analysis. Smoothed hazard estimates were obtained with their 95% CIs to evaluate whether the timing of the revisions differed between the two groups [26]. Hazard estimates quantify the immediate risk, in this case of all-cause revision, attached to an individual known to be alive at time t. All analysis were performed using a statistical package PASW statistics version 25 (Chicago: SPSS Inc.) and Stata version 17 (Stata Corp., College Station, Texas).




Comments (0)