While DAIR is widely accepted as the preferred treatment strategy for postoperative acute PJI, there is ongoing debate regarding the optimal time frame within which it can be performed successfully. The present study aimed to evaluate the five year success rates of DAIR for acute PJIs occurring within different time intervals following index arthroplasty. Results indicated no significant difference in outcomes between patients who underwent DAIR within the first four weeks versus those treated between weeks five and 12.
These findings align with a recent multi-centre study that also reported no significant differences in revision rates at one year follow-up across similar time frames [9]. In that study, which included 769 patients, the one year failure rate reached 38%, with failure rates of 42% for weeks one to two, 38% for weeks three to four, 29% for weeks five to six, and 42% for weeks seven to12. Similarities in causative microorganisms, comorbidities, and symptom duration were observed across time intervals, supporting the viability of DAIR beyond the four week mark, provided it is performed within one week of symptom onset and modular component exchange is feasible.
Conversely, current IDSA guidelines recommend DAIR only for PJIs diagnosed within the first four weeks post-index arthroplasty [8]. This limitation potentially excludes a considerable subset of patients who could benefit from DAIR, possibly exposing them to complications related to early implant removal. This consideration is particularly relevant as approximately 25% of early PJIs of the present series manifested between weeks five and 12 after the index surgery.
Other studies, however, present conflicting perspectives. A recent retrospective analysis of 189 knee PJIs managed with DAIR reported that time from index arthroplasty was a significant predictor of outcome, reporting two year success rates of 67.4%, 52.9%, 42.4%, 41.5%, and 29.1% for PJIs treated within zero to one, one to three, three to 12 months, one to three years, and over three years, respectively [11]. These authors concluded that DAIR remains a reasonable option for PJIs occurring within the first year, given the risks associated with staged revision surgery.
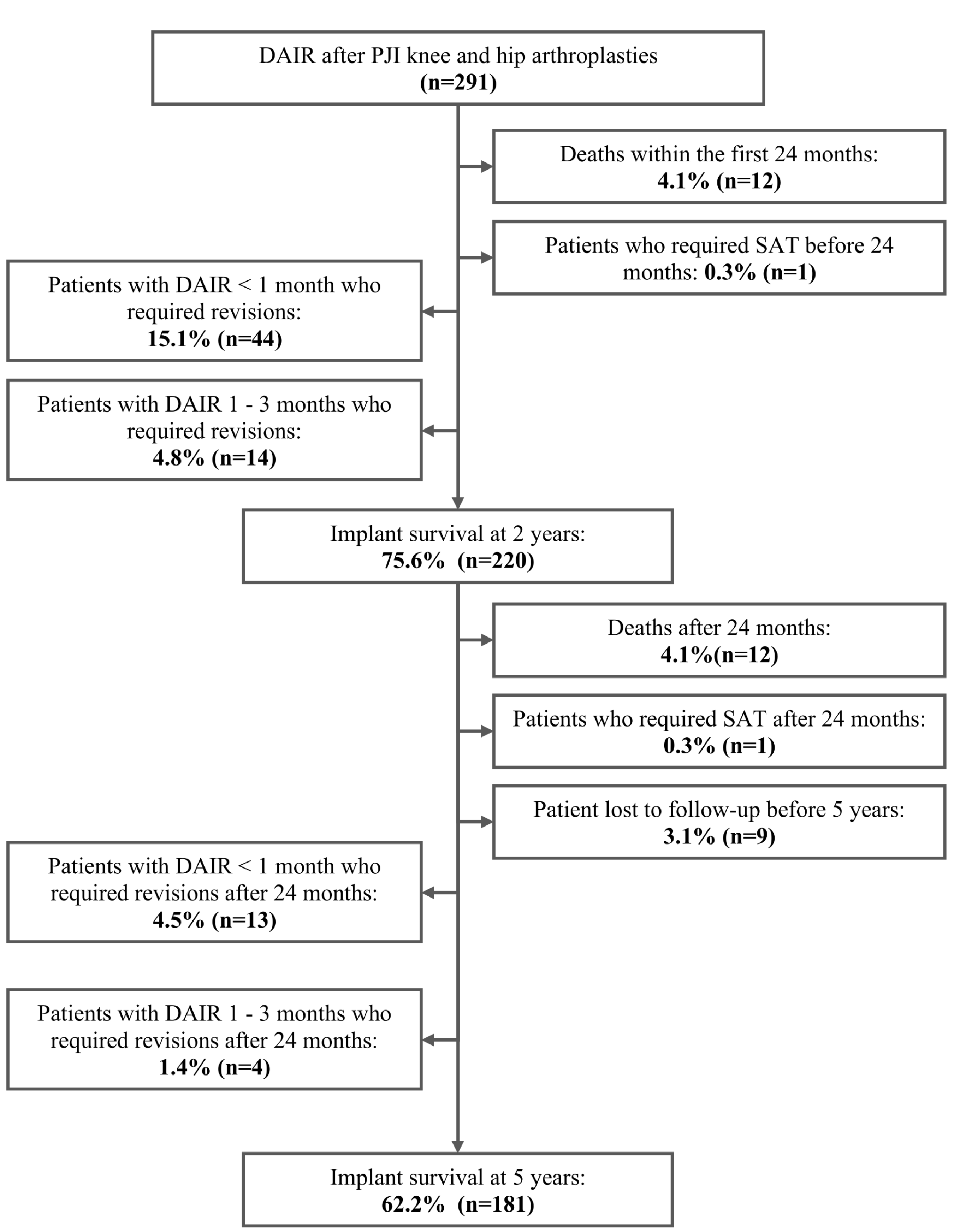
Long-term data on DAIR success beyond two years are scarce. Clauss et al. [12] followed 56 patients with hip PJI treated with DAIR, reporting a 16% revision rate after an average follow-up of 6.1 years. Our study observed a higher five year revision rate of 25.8% (75 out of 291), which may reflect differences in patient populations or treatment protocols. Similarly, Grammatopoulos et al. [13] reported an 85% implant survival rate at five years in 122 PJI cases managed with DAIR for both primary and revision hip arthroplasties, with 23% requiring additional surgery. Notably, in that study, prolonged antibiotic therapy lasting from 0.5 to three years was common, and suppressive antibiotic therapy (SAT) was not counted as a failure outcome.
The present study has several inherent limitations. Foremost, its retrospective design may have introduced selection bias, limiting control over confounding variables and constraining the scope of the data collected. Additionally, the absence of a control group is a limitation, and it is important to acknowledge that clinical practices and protocols may have evolved over the study period, potentially affecting outcomes. Consequently, these factors should be considered when interpreting the generalizability of our findings. Nonetheless, the study cohort represents one of the largest published to date. Despite a debatable five year success rate of 70%, we believe that DAIR remains a viable approach for managing acute PJIs within the first three months post-arthroplasty.
In conclusion, our data suggest no significant difference in outcomes between patients undergoing DAIR within four weeks and those treated between weeks five and 12. However, it is noticeable that the overall success rate decreased from 75.6 to 62.2% in the last three years of follow-up. Further prospective studies with larger cohorts and extended follow-up are needed to confirm these findings and refine criteria for DAIR success.




Comments (0)