
Remember me



This was a retrospective single-centre study of RHF surgically treated between January 2008 and December 2017. The operative database identified 242 patients who sustained a RHF during the study period. The inclusion criteria were patients of 18 years or older presenting a closed comminuted RHF confirmed by a preoperative CT-scan, surgically treated within 15 days of the traumatism, with a minimum of five years follow-up.
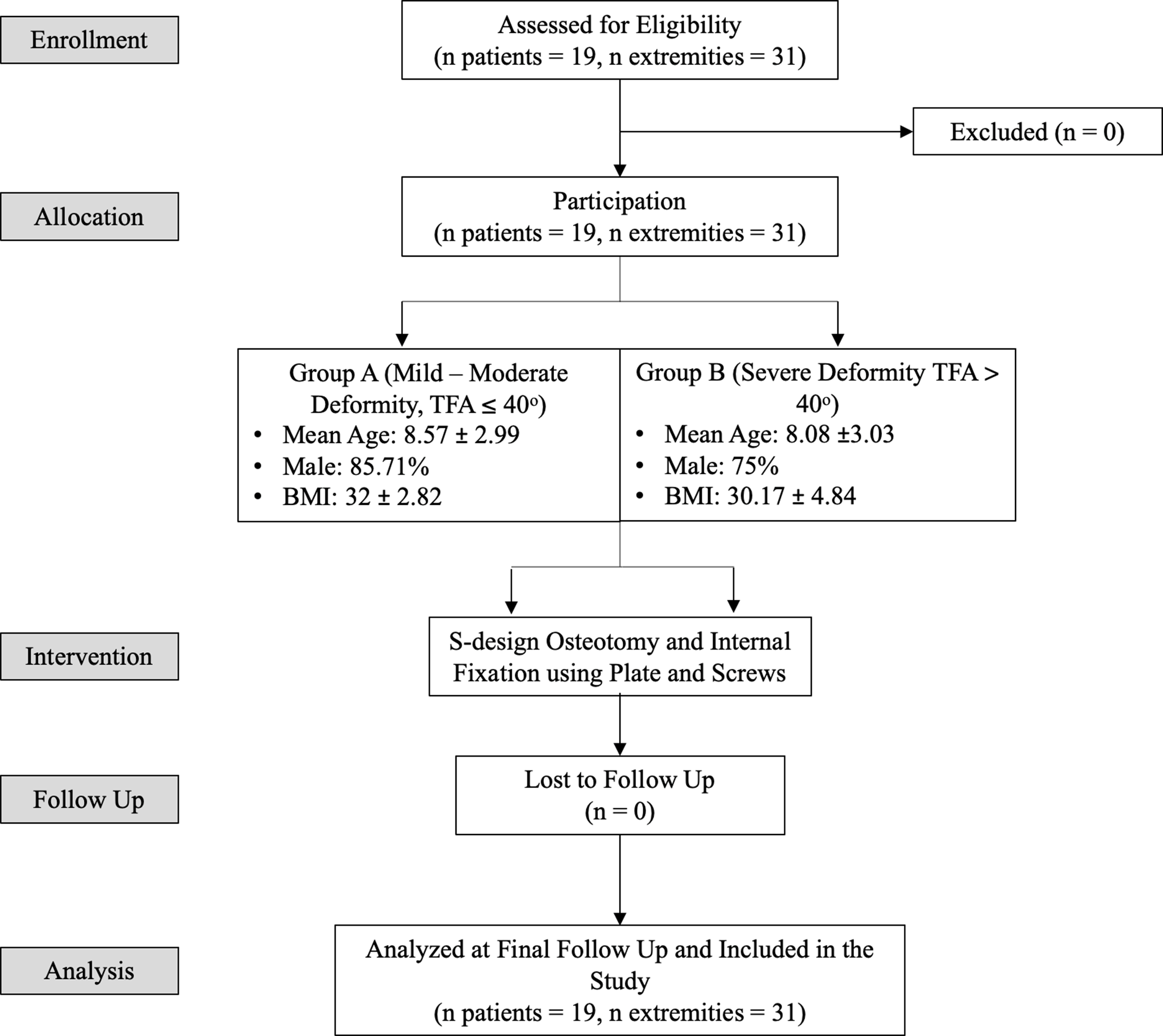
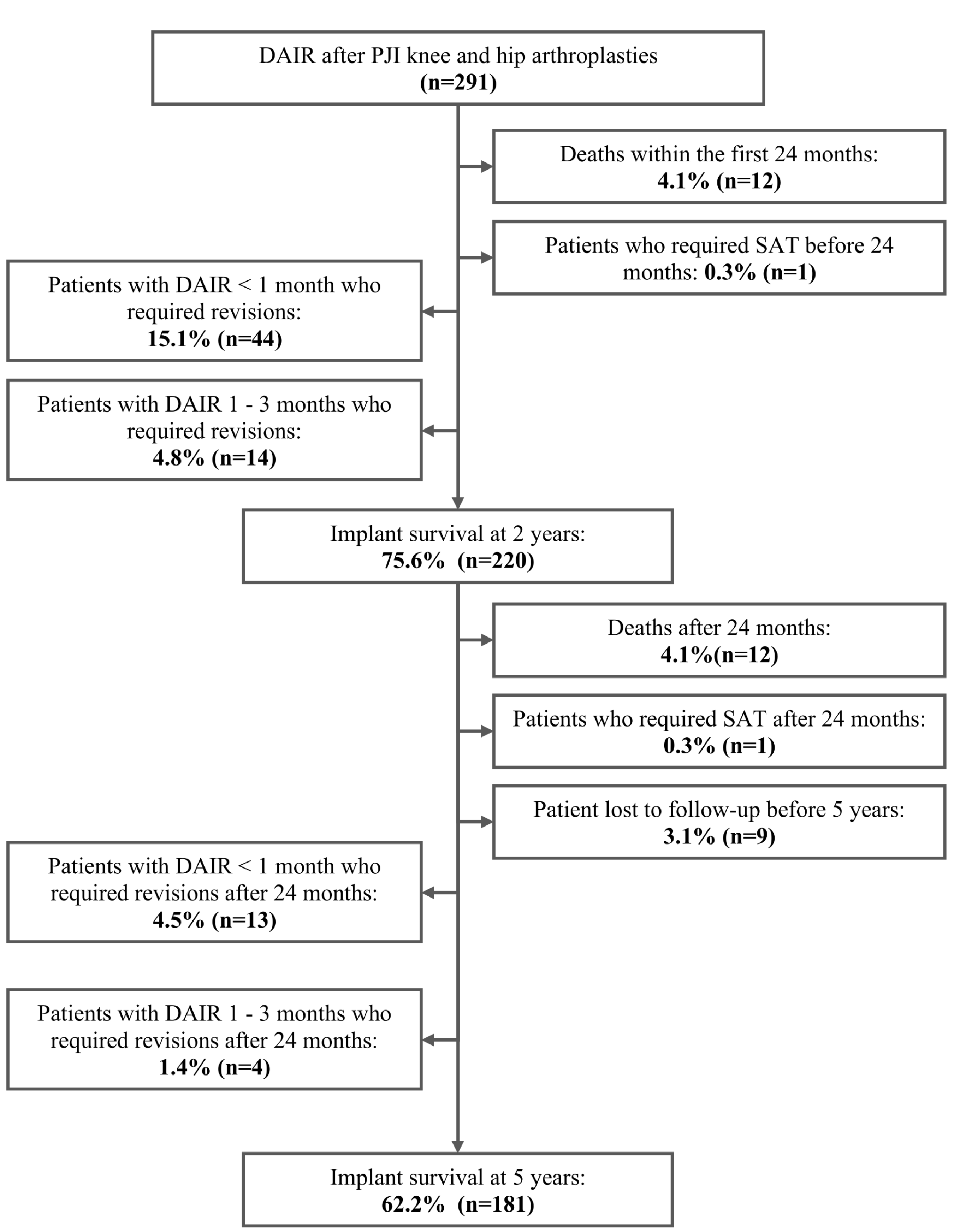
All the non-isolated Mason type-III RHF were excluded. Sixty-five type-III fractures remained. Four were treated more than 15 days after the injury, and seven patients were lost to follow-up. A total of 19 patients in group RHA, and 35 in group ORIF were included in the final analysis (Fig. 1).
Fig. 1
Workflow diagram with details of excluded associated injuries. TOFD: trans olecranon fracture dislocation, RHA: radial head arthroplasty, ORIF: open reduction and internal fixation
Surgical techniqueThe skin incision was centered on the lateral epicondyle. The RH was exposed through Kocher interval between anconeus and extensor carpi ulnaris muscles, allowing assessment of the lateral collateral ligament (LCL) [9]. There were five (26%) torn LCL in group RHA and three (8.5%) in group ORIF (p > 0.05), that were repaired by trans-osseous suture.
The management was done according to the surgeon’s preference. RHA was performed when the fracture was deemed unrepairable, and in three cases after intraoperative failure of ORIF. Three RHA were used: STANDARD in nine cases and RECON in seven cases rHead® SBI-Stryker (Morrisville, PA, USA), and bipolar Judet CRF II® (Tornier SA, Saint-Ismier, France) in three cases. The surgical technique was the same for the different implants: RH was cut a few millimeters under the distal part of the sigmoid notch. Progressive larger rasps were used to open the medullary canal to reach the right size of the prosthesis. Trials were done before definitive implantation.
Postoperative protocol and follow-upPostoperatively, patients had a sling for two to four weeks. Active and passive motion were allowed without strength during the first three months. Patients were evaluated at regular intervals (1 month, 3 months, and then yearly).
Clinical assessmentComputerized data were retrieved to collect demographics, and intraoperative details. All patients were contacted for a clinical and radiological follow-up by a single observer independent from the initial surgery. Patients were asked about their pain levels on a verbal analogical scale (VAS) and their subjective elbow value (SEV).
The clinical examination was bilateral. Active range of motion (ROM) in flexion-extension and forearm prono-supination were measured with a goniometer. Grip strength was measured using a hydraulic dynamometer (JAMAR®, Jackson, MI, USA) as well as forearm rotation strength (Inc. Elmsford, NY, USA). The mean measurement of three repeated trials on each side was reported. Elbow stability was assessed by dynamical maneuvers in valgus and varus.
The clinical examination allowed the calculation of two functional scores: the Mayo Elbow Performance Score (MEPS) [10]; and the Lyon Elbow Score (LES) assessing function, ROM and strength in flexion-extension, but also forearm prono-supination [11]. Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) [12] and Oxford Elbow Score (OES) were calculated [13]. All scores were quantified on a 100-point scale, 100 being the best score for SEV, MEPS, and LES; and 0 for QuickDASH and OES.
Failures were defined as surgical re-intervention if associated to symptomatic discomfort, including secondary resection of the RH with implant or material removal. All complications were recorded. Elbow was considered stiff if active ROM did not reach the functional level defined by Morrey et al. (lack of extension ≥ 30° and/or flexion ≤ 130°) [14].
Radiographic assessmentAt last follow-up, antero-posterior and lateral views were performed. In both groups heterotopic ossifications (HO) [15] and degenerative changes [16] were recorded. In group RHA, location of peri-prosthetic radiolucencies was reported as described by Chen et al. [17] (Fig. 2). Overlengthening was measured on the postoperative frontal view as described by Wegmann et al. [18], which differs from overstuffing. RHA was considered overstuffed when its diameter exceeded 140% of the native capitulum since RH is anatomically 120–140% larger than the capitulum [19, 20] (Fig. 3).
Fig. 2
Radiological location of peri-prosthetic radiolucencies. Division into 5 zones in (A) anteroposterior view (zones 1 to 5) and (B) lateral view (zones 6 to 10) respectively, according to Chen et al. [17]
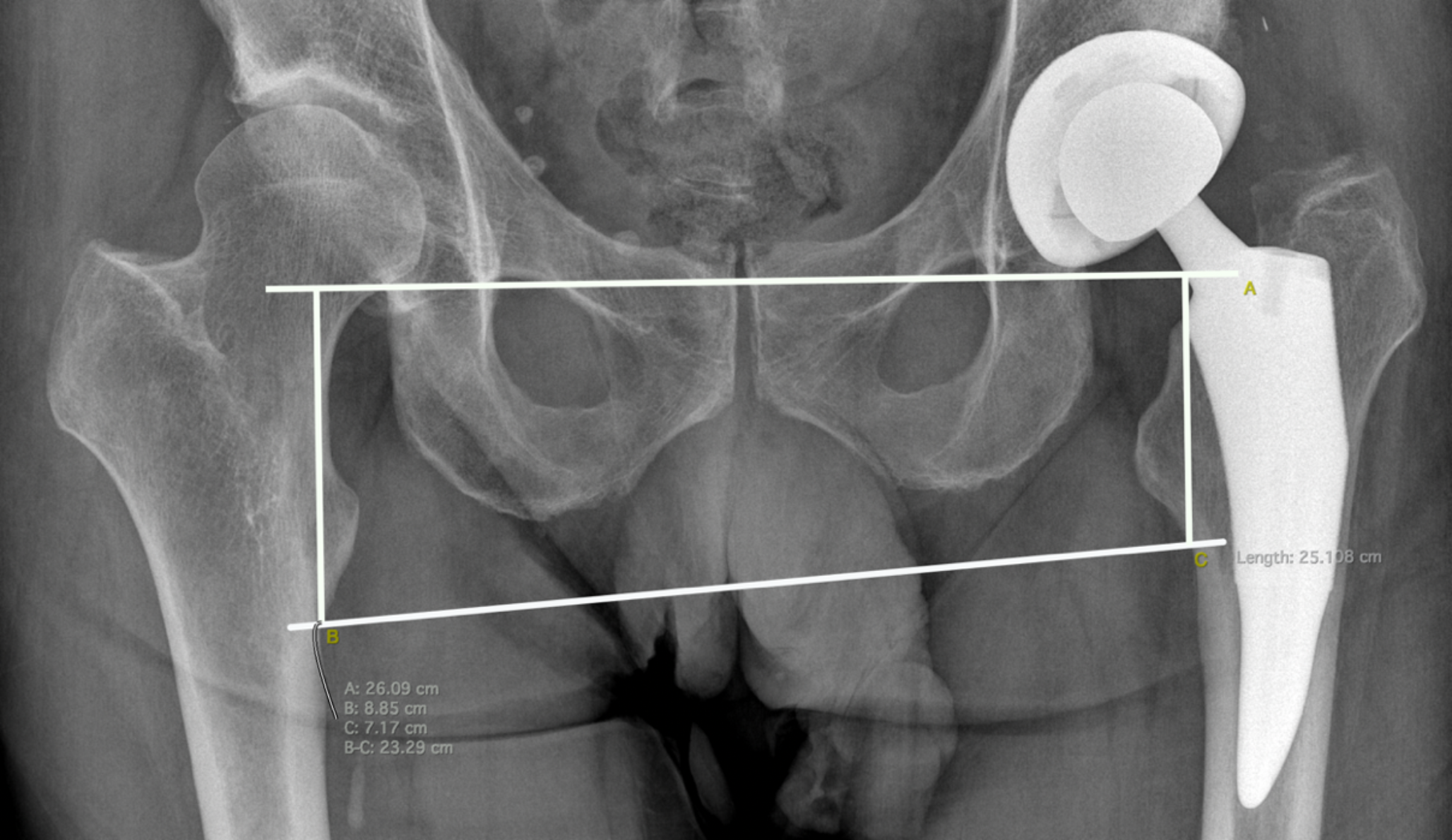
Fig. 3
Antero-posterior view of right elbow radiograph 13 years after RHA. Distinguish overlengthening (A) and overstuffing (B). Note erosion of capitulum with stable elbow (type IIB of Wegmann [18]). Subjective Elbow Value 80 and Lyon Elbow Score 81. (A) Overlengthening of 7 mm between the proximal edge of the lesser sigmoid notch (yellow dotted line) and radial head (black dotted line). (B) Overstuffing measured by dividing the diameter of the radial head (red arrow) by the capitellar width, the line joining the center of the capitulum and the trochlear groove (red dotted line) [19]
The number of RH fragments was retrospectively calculated on the preoperative CT-scan.
Statistical analysisStatistical analysis was performed using the XL-STAT software (Addinsoft, Paris, France). Continuous variables were reported as mean. Categorical outcomes were compared using Fisher’s exact test and chi-squared test. Normally distributed continuous variables were compared using the Student t-test. A p-value < 0.05 was considered statistically significant for all analyses. A post hoc power analysis was conducted using G*Power software (Dusseldorf, Germany).
EthicsThis retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board (IRB) approved this study in our institution on June 2024 (declaration 00012836). An information note and a non-opposition statement have been provided to patients.
This research received no funding.
Comments (0)