
Remember me

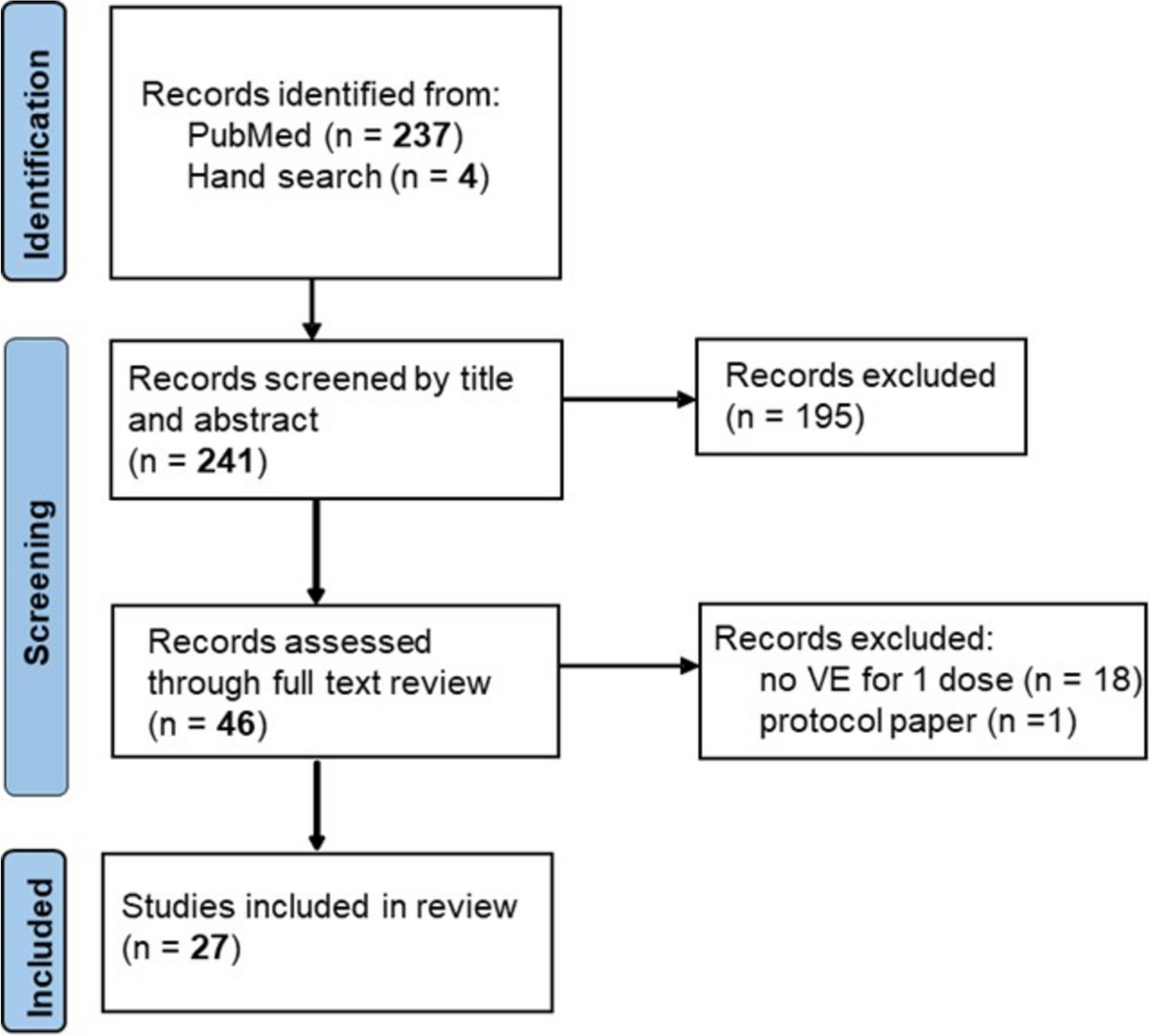

Anti-SARS-CoV-2 S assay data were available for 1,294,571 subjects during the study period and, of these, 489,933 could be successfully linked with their insurance claim records. After applying the exclusion criteria, 268,844 subjects were included in the primary analyses (Fig. 1c). Baseline demographics are shown in Table 1.
Over the 15-month study period, the overall SARS-CoV-2 antibody levels increased significantly (Supplemental Fig. 2); the introduction of vaccines and the emergence of the Omicron variant is reflected in this increase.
Fig. 2
Risk of severe infection in participants with various SARS-CoV-2 antibody levels compared with a non-reactive result
Antibody Level and Risk of SARS-CoV-2 InfectionAmong subjects with non-reactive results (< 0.8 U/mL), 40.3% developed symptomatic SARS-CoV-2 infection and 4.1% developed severe outcomes within 12 months of their antibody test. Within the same timeframe, only 11.1% of subjects with reactive antibody levels developed symptomatic SARS-CoV-2 infection and only 0.6% developed severe forms of the disease.
The risk of symptomatic and severe infection following infection with SARS-CoV-2 within 12 months of testing decreased as observed antibody levels increased. After inverse probability weighting, subjects with antibody levels of ≥ 0.8 and < 100 U/mL had a 42% reduced risk of symptomatic infection (HR = 0.58, 95% CI [0.55, 0.61]) compared with those who had non-reactive results (< 0.8 U/mL). Subjects with antibody levels between 100 and < 2500 U/mL and ≥ 2500 U/mL had 53% and 62% reduced risk of symptomatic infection (HR = 0.47, 95% CI [0.45, 0.49] and HR = 0.38, 95% CI [0.36, 0.39]), respectively. The risk of severe infection was also reduced by 59%, 79%, and 87%, respectively (0.41 [0.36, 0.48], 0.21 [0.18, 0.23], and 0.13 [0.11, 0.15]) at these antibody levels compared with a non-reactive result (< 0.8 U/mL) (Table 2; Fig. 2).
Table 2 Unweighted and weighted Hazard Ratios (HRs) for SARS-CoV-2 symptomatic and severe infectionOlder and Immunocompromised SubjectsIndividuals aged 65 years and over were more likely to have had a prior infection and/or a vaccination compared with those aged under 65 years. This observation fitted to a lower proportion of non-reactive results for the older age group compared with the younger (4.9% vs. 10.2%) and a higher proportion had the highest level of antibody ≥ 2500 U/mL (45.7% vs. 37.1%) (Supplemental Table 3), both likely resulting from advanced vaccination and booster schemes in this age group.
In total, 75,793 (28.2%) subjects were categorized as immunocompromised and 193,051 (71.8%) as non-immunocompromised. The proportion of individuals with immunocompromised conditions who developed COVID-19 outcomes was higher than those without (14% vs. 13.4% [p < 0.001] for symptomatic infection, 1.3% vs. 0.7% for severe infection [p < 0.001]).
The associations between antibody level and the subsequent COVID-19 outcomes had a similar trend across the sub-cohorts (under 65 years, 65 years and over, and immunocompromised and non-immunocompromised cohorts) as with the main analysis set: elevated antibody levels were associated with a stronger reduction in the risk of subsequent negative COVID-19 outcomes. However, when comparing individuals with and without immunocompromised conditions, increased antibody levels provided less effective protection against COVID-19 outcomes for those with immunocompromised conditions (Fig. 3).
Fig. 3
Risk of negative outcomes in participants with varying SARS-CoV-2 antibody levels stratified by age, immunocompromised status and variant subtype in those with symptomatic (a) and severe (b) COVID-19 infection. CI confidence interval, HR hazard ratio
Unweighted HRs for all subgroups are presented in Supplemental Table 4.
Variant AnalysisIn total, 4982 (4.4%) and 7486 (7.3%) symptomatic infections within 6 months of the antibody test were attributed to Delta and Omicron variants respectively. Reactive antibody results were associated with a reduced risk (79–90%) of symptomatic SARS-CoV-2 infections for the Delta variant cohort [HR = 0.21, 95% CI (0.19, 0.24) for antibody levels between 0.8 and < 100 U/mL, 0.16 (0.15, 0.17) for ≥ 100 and < 2500 U/mL, 0.1 (0.09, 0.11) for antibody level ≥ 2500 U/mL]. For the Omicron variant, a smaller reduction in risk (46‒72%) was observed [HR = 0.54, 95% CI (0.47, 0.62) for antibody levels between 0.8 and < 100 U/mL, 0.47 (0.42, 0.52) for ≥ 100 and < 2500 U/mL, 0.28 (0.25, 0.31) for antibody levels ≥ 2500 U/mL], compared with antibody level < 0.8 U/mL. Similarly, the risk of developing severe infection decreased by over 86% for Delta variant infections in all subjects with a reactive antibody level (≥ 0.8 U/mL), whereas in an Omicron setting, this strong level of risk reduction was only observed at the highest antibody titer level (≥ 2500 U/mL) (Fig. 3).
Sensitivity AnalysisThe association between antibody levels and subsequent COVID-19 outcomes was found to be consistent among individuals with continuous insurance enrolment during 181 days prior to the index date compared with the main cohort (Supplemental Tables 5 and 6).
Comments (0)