
Remember me



A total of 107 NH residents, aged 50 years or older and vaccinated during the primary COVID-19 vaccination series, were enrolled into this observational study; 18 from a nursing home in the northwest of the Netherlands (single location) and 89 from ten locations in the south of the Netherlands. Nursing home doctors determined if residents were mentally competent and able to provide informed consent themselves. If not, medical ethical approval for study participation was not allowed.
All residents received BNT162b2 (Comirnaty, Pfizer/BioNTech) homologous vaccination series of two doses which were given about four weeks apart (January-March 2021). NH residents also received a third (November-December 2021 or February 2022 for five (5%) SARS-CoV-2 individuals) and a fourth BNT162b2 vaccination (March 2022 or May/June 2022 for 24 (22%) SARS-CoV-2 individuals), which was followed by a fifth BNT162b2 bivalent (WT/OMI BA.1) vaccination in October 2022.
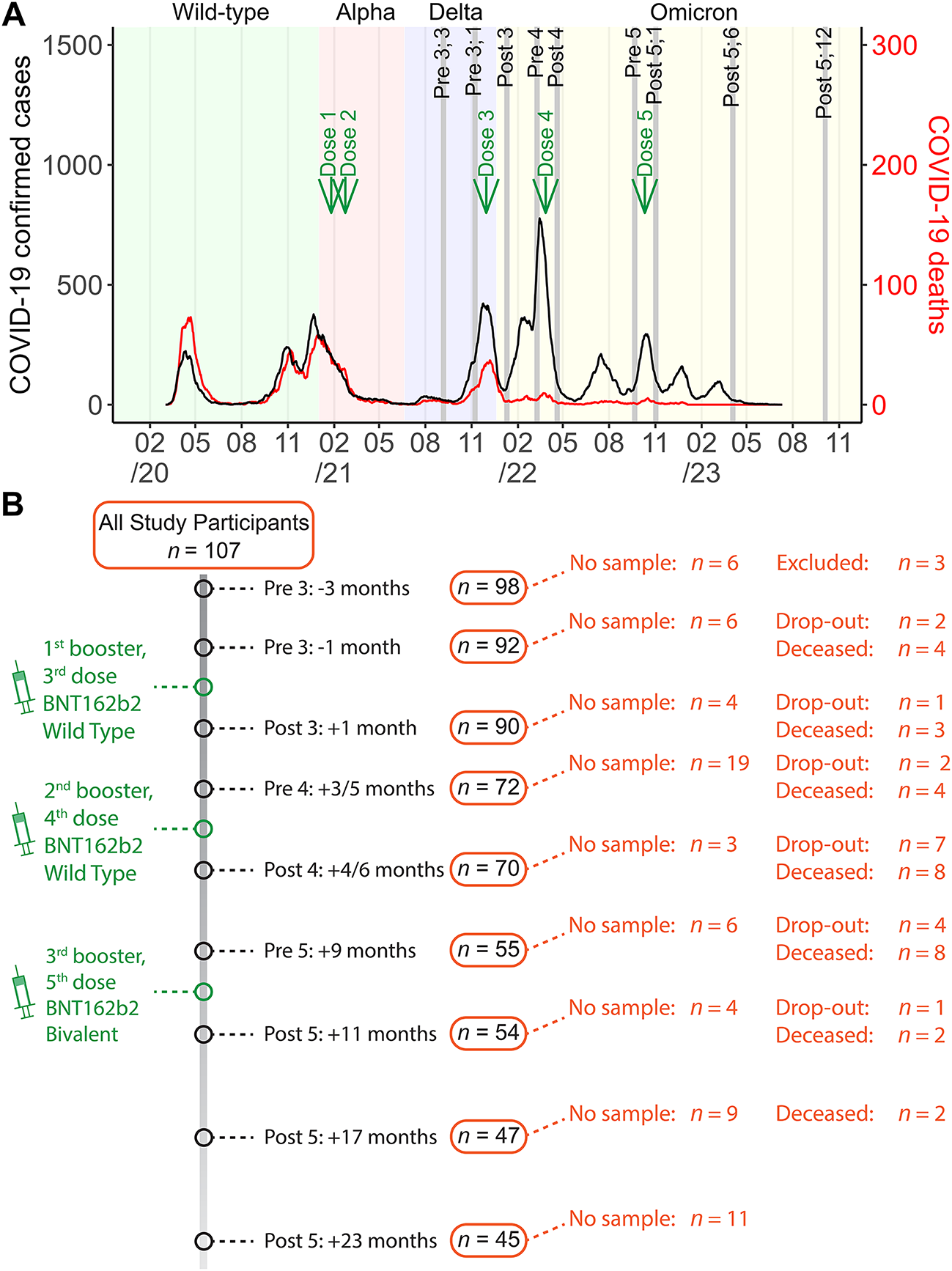
The nursing home clinicians decided which residents of their homes were eligible for possible participation on a somatic basis. Nursing home residents filled in a participation card. The duration of the study was 2 years and one month, starting in September 2021 with the last sampling timepoint in October 2023. The first sampling timepoint was six months after completion of the primary vaccination series and three months before the first booster dose. Afterwards, sampling timepoints were one month before and after the administration of a vaccine dose. Additionally, samples were collected six and twelve months after the bivalent vaccine as the fifth vaccine dose (Fig. 1A).
Fig. 1Study design with number of study participants, vaccine and sampling timepoints, and the different dominant SARS-CoV-2 variant periods. (a) Information on the number of COVID-19 confirmed cases and deaths of older adults aged 70 years or over who live in a nursing home in the Netherlands. Data was collected until the 11th of July 2023 and obtained from data.rivm.nl/covid-19/. Additionally, information on vaccine dose administration, sampling timepoints, and circulating SARS-CoV-2 variants of concern have been indicated in the graph. (b) A flowchart depicting vaccine dose administration and sampling timepoints together with information on the number of study participants per timepoint
Blood and data sampling nursing home residentsAt each timepoint, a fingerprick whole blood sample was drawn in MiniCollect® serum/gel tubes of 0,5 ml/0,8 ml with a clotting activator (Greiner Bio-one Netherlands) at the nursing home locations by a dedicated study nurse. In addition questionnaires covering demographic factors, comorbidities, COVID-19 vaccination brand and dates and, if applicable, information on SARS-CoV-2 confirmatory testing (PCR testing of a nose/throat swab) were filled in by the nursing home clinicians. By fingerpricks a volume of 200–400 ul whole blood was sampled. Samples were kept at RT and transported to the laboratory. After centrifugation the tubes for 10 min at 3000 rpm, a serum volume of about 100–200 ul per sample have been stored at -20 °C. The volume of just a few blood samples resulted in serum volumes lower than 100 ul or even too low for further analysis.
SARS-CoV-2 infection-related clinical data nursing home residentsClinical data of NH residents from eight locations in the south of the Netherlands with a test-confirmed SARS-CoV-2 infection (n = 35) were collected by the nursing homes clinicians until the end of the study and independently reviewed by two healthcare workers. This included use and duration of dexamethasone, fraxiparine, oxygen, and IV fluids. Data regarding the presence and duration of fever (> 37.5 °C), maximum temperature recorded during the fever episode (measured every morning and evening) were also recorded, together with the date(s) of positive COVID-19 test(s) and the duration of isolation periods. These data were grouped based on circulating SARS-CoV-2 variants (Fig. 1A); WT (before the primary series), Delta (timepoints before the third dose), or Omicron (timepoints after the third dose until one year after the fifth dose). None of the participants had a SARS-CoV-2 infection when the SARS-CoV-2 Alpha variant was dominant.
.
Cohort of community-dwelling older adults from the general populationFingerprick blood samples of participants of the general population and part of the Doetinchem Cohort Study (DCS) [17] who were 50 + years of age and also received either three, four, or five BNT162b2 vaccination doses, similar to the NH residents, were included in the community-dwelling older adult cohort18(n = 32). Participants of the general population indicated the specific vaccine received at every study timepoint in the questionnaires. In addition, vaccination was controlled by the national vaccination registry (CIMS). Timepoints of blood and data sampling completely matched that of the NH cohort, only the sampling timepoint before the fourth vaccine dose was not available due to logistical constraints. Questionnaires covering demographic factors, comorbidities, COVID-19 vaccination brand and dates and, if applicable, information on SARS-CoV-2 confirmatory testing (PCR testing of a nose/throat swab) were filled at every study timepoint.
The age of all study participants was the age in years at first BNT162b2 vaccination and sex is defined as the sex assigned at birth.
Antibody detectionAnti-SARS-CoV-2 Spike S1 (S1)-, Nucleoprotein (N)-, and Spike protein receptor binding domain (RBD)-specific immunoglobulin G (IgG) antibody concentrations against the WT strain were measured using a previously described multiplex bead-based assay [19]. In short, serum samples (25 µl) diluted in SM01 buffer (Surmodics, Eden Prairie, MN, USA) containing 2% fetal calf serum were mixed with beads coated with either SARS-CoV-2 WT monomeric spike S1 (40591-V08H), RBD (40592-V08B), or N (40588-V08B) proteins or recombinant SARS-CoV-2 B1.1.529.1, also referred to as BA.1, (Omicron) Spike S1 (40591-V08H41) or RBD (40592-V08H121) proteins (all Sino Biological, Beijing, China) and incubated for 45 min at room temperature in the dark while rotating (750 rpm). Thereafter, samples were washed three times with phosphate-buffered saline, incubated with phycoerythrin-conjugated goat anti-human IgG (Jackson ImmunoResearch, West Grove, PA, USA) for 30 min, and, thereafter, washed and analyzed with an LX200 (Luminex, Genk, Belgium). Concentrations were interpolated using a 5-parameter logistic fit using pooled sera calibrated against the WHO international standard (NIBSC 20/136) for WT antigens and expressed as binding antibody units per ml (BAU/ml). The threshold for seropositivity was set at 10.1 BAU/ml for S120, 14.3 BAU/ml for N [18], and 30.0 BAU/ml for RBD [20]. Anti-Omicron antibody concentrations were expressed as arbitrary units per ml (AU/ml).
SARS-CoV-2 infection status definitionIndividuals were classified as either infection-naïve or SARS-CoV-2-infected. Participants were considered to have had a SARS-CoV-2 infection when a positive test was reported in the questionnaire, when their concentration of anti-N antibodies exceeded the cut-off value of 14.3 BAU/ml or were re-infected when this anti-N antibody concentration was four-fold higher than the previously reported concentration. Infections scored at a given timepoint took place before the given timepoint. A naïve participant who became infected got switched to the SARS-CoV-2-infected group during the further study follow up. Eleven participants were infected twice with SARS-CoV-2 during the study. Individuals that had anti-N antibody seroconversion without reported SARS-CoV-2 infection at the first timepoint were excluded from the study given that the exact date of the infection was unknown. As the period in which the infection occurred was known, the dominant SARS-CoV-2 variant (WT, Delta, or Omicron) of that period was also known from the information on the number of COVID-19 confirmed cases and deaths of older adults aged 70 years or over who live in a nursing home in the Netherlands. Data was collected until the 11th of July 2023 and obtained from data.rivm.nl/covid-19/ (Fig. 1).
Statistical analysesStatistical analyses and visualization were performed in R 4.4.0 and R studio 2024.04.1. The distribution of the data was assessed with a Shapiro-Wilk test and QQ-plots. When the data did not pass these checks or had a small group size, a non-parametric statistical test was used. Anti-WT and anti-Omicron antibody concentrations were both expressed in AU/ml for the Omicron versus WT S1-IgG ratio calculations. A non-parametric Kruskal-Wallis ANOVA with a Dunn’s multiple comparison corrected post-hoc test (Holm’s method; Rstatix v 0.7.0) was used to assess differences in antibody concentrations or ratio’s. Significant differences of discrete clinical data were evaluated with a pairwise chi-square test (Rstatix).
We constructed two linear mixed effects models (LMEMs) to investigate covariate influence on the log10-transformed anti-S1 antibody concentrations in infection-naïve and infected individuals separately (lme4 v1.1-30). Using these models potential associations between clinical data of the NH residents collected by the nursing homes clinicians (Table S2) and antibody concentrations at all study time points were further assessed. For both models, the fixed effects were specified as age, sex, using prednisone, and whether someone had diabetes, cancer, rheumatoid arthritis, or any lung, bowel, immune, kidney, cardiovascular, neurological, skin, or mental disease. Participant numbers and sampling timepoints were specified as random effects both models model. For the LMEM of infected individuals, an additional random effect was specified as the timepoint that an individual became infected. A forest plot was generated displaying the coefficient estimates and multiple comparison testing adjusted p-values (Holm’s method) for each model (sjPlot v2.8.11).
LMEMs were also constructed to assess changes in log10-anti-S1 antibody concentrations following the third, fourth, and fifth vaccine dose in infection-naïve and infected individuals separately. Only individuals that received a third, fourth, and fifth vaccine dose were included in the models. For these antibody decay and increase LMEMs, we excluded the study participants who had an SARS-CoV-2 infection during the analyzed time period. In the constructed LMEMs, the time since the vaccine dose was specified as a fixed effect and the number of participants was specified as a random effect. Differences between infection-naïve and previously infected individuals in antibody decay rates and rates in which antibody levels increased were assessed with a one-way ANOVA (lmerTest v3.1-3). Antibody half-life, in time in days since the last vaccine dose, was calculated with the predicted anti-S1-antibody concentrations of the fitted LMEM. Differences between slopes was tested with a Welch modified two-sample t-test (BSDA v1.2.2).
Other R packages that were used for data analysis and visualization were; dplyr v1.0.10, tidyr v1.2.1, tidyverse v1.3.2, reshape2 v1.4.4, zoo v1.8-10, and janitor v2.2.0 for data manipulation/organization, gglot2 v3.4.0, RColorBrewer v1.1-3 and ggh4x v0.2.3 for data visualization, and qwraps2 v0.5.2 for generating tables.
Analyses with p-values of < 0.05 were considered statistically significant.
Ethical approvalEthical approval and oversight was carried out by the Medical Research Ethics Committee (METC) NedMed, Utrecht (METC number: 21/056, study number: NL76551.041.21, EudraCT: 2021-001976-40). All participants provided written informed consent.
Role of the funding sourceThe funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Comments (0)