This cross-sectional, retrospective, real-world study, conducted in one of the largest claims databases in the US, provides valuable insights into the use of Although asthma severity biologic therapies in patients with CRSwNP during a focused point in time when biologics were first gaining US approval for CRSwNP. Retrospective evaluation of treatment patterns during such a time is particularly useful as this is when new paradigms of care often emerge, allowing assessment of how newly approved biologics begin to fit into everyday clinical practice. Furthermore, these early observations provide the opportunity for the medical community to understand how onsite practice patterns compare with current treatment guidelines.
In line with current treatment guidelines on biologic intervention, this study identified asthma and prior OCS/doxycycline treatment as predictive factors of biologic use. [7, 9, 26]. The other predictive factors identified (allergic rhinitis, chronic rhinosinusitus, GERD, and age < 65 years) extend the profile of patients likely to use biologics. To the best of our knowledge, this is the first study to provide predictors of biologic use in patients with CRSwNP in a quantitative fashion using real-world data from clinical practice. To date, literature that includes patient markers has largely focused on understanding those that predicted response to biologics, rather than biologic use [27,28,29]. Publications that refer to markers in terms of patient suitability for receiving biologics do so qualitatively [30, 31]. Therefore, this study provides a unique perspective on the clinical use of biologics in CRSwNP, which may help clinicians better understand their patients’ therapeutic needs and the likelihood of them requiring biologics later in their treatment pathway. This could facilitate earlier determination of the appropriate multidisciplinary team input and treatment, monitoring and communication strategy required for patients with high unmet needs.
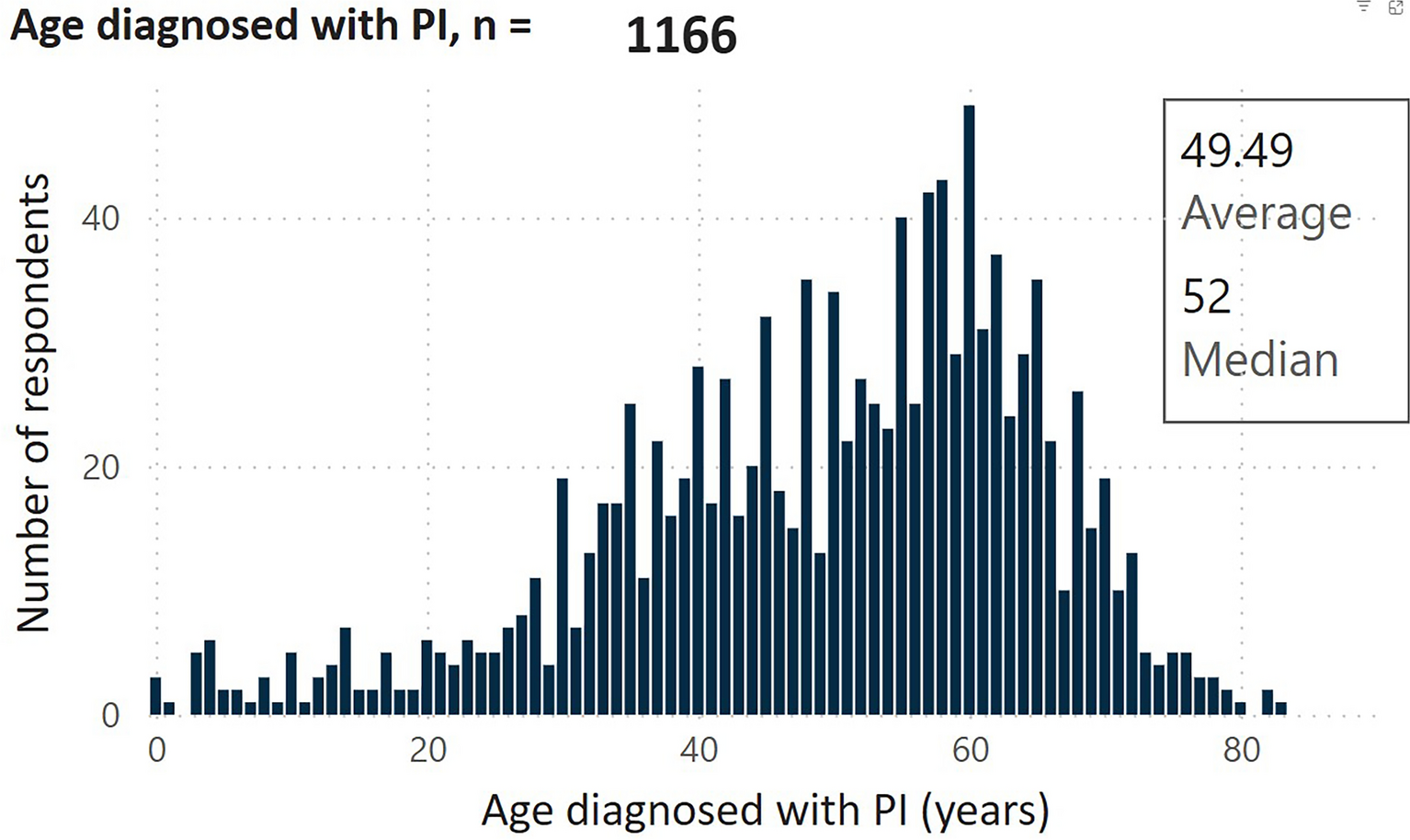
Patient demographics were similar to other database and clinical trials involving patients with CRSwNP [1, 10, 32,33,34,35]. There were a number of key demographic differences between biologic users and non-users. Patients under 65 years of age were over 50% more likely to use biologics than those aged over 65 years, and patients with Medicare Supplemental coverage had approximately 40% lower use of biologics than patients with commercial coverage, which could reflect caution from physicians in prescribing biologics to older patients[36] or differences in insurance coverage of medications in the Medicare Supplemental and Commercial populations. These differences may also explain why biologic users were more likely to live in urban areas and have claims captured in the Commercial database. For example, urban areas in the US frequently contain a greater proportion of people under 65 years of age than rural areas, while the Commercial database includes the under-65 working population versus Medicare, which includes retirees [37, 38]. Potential disparities in access to biologics within urban versus non-urban settings may also be a contributing factor [39].
In this study, biologic users more commonly had comorbid asthma and other clinical conditions than non-biologic users. Indeed, patients with comorbid asthma without biologic use during the study identification period were over fivefold more likely to receive biologics than those without comorbid asthma. This is in accordance with European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020, and ICAR 2021 criteria for biologic selection, which suggest consideration of the use of biologics in patients with comorbid asthma [7, 9, 26]. In addition, comorbid asthma could possibly be the primary indication for which patients were receiving the biologic, since the biologics included in this study are approved to treat one or more conditions, including severe asthma [16, 18,19,20,21]. Although asthma severity was not recorded in this study, the proportion of patients who had ≥ 2 asthma exacerbations provides an estimate of those with severe asthma, as per European Respiratory Society/American Thoracic Society guidelines, which include exacerbation criteria in their definition of severe asthma [40, 41]. As such, only 27% of biologic users had ≥ 2 asthma exacerbations, suggesting most biologic use was not for severe asthma. Beyond asthma, GERD was also identified as a predictor of biologic use, possibly relating to increased likelihood of type 2 inflammation (i.e., eosinophilia and high levels of interleukin-4/5/13) and therefore biologic selection, in patients with CRSwNP and GERD [7, 8, 42].
Biologic users more commonly used OCS and other CRSwNP-related treatments as well as drug-related services than non-biologic users; however, use of diagnostic services (e.g., endoscopy and sinus CT scan services) was lower in biologic users than non-users. OCS response can indicate the presence of type 2 inflammation and thus the likelihood of response to biologics which target the type 2 pathway (i.e., immunoglobulin E, interleukin-4/5/13) [7, 8, 26]. Furthermore, as per treatment paradigm/guidance recommendations, advancing to biologic treatment requires a confirmed diagnosis of uncontrolled severe disease for which a patient has received systemic corticosteroids in the previous 2 years [7, 26]. Greater diagnostic service utilization in non-biologic users versus biologic users could be related to more recent CRSwNP diagnosis requiring more frequent monitoring, such as value judgment [9]. Also, biologic users may have reduced need for diagnostics due to clinical response. Greater use of drug-related services in biologic users compared with non-users is potentially related to associated biologic prescriptions and administrations. Use of OCS and doxycycline, which were predictive factors of biologic use, indicates more severe disease, higher disease burden, and unmet need in biologic users. This aligns with ICAR 2021 guidelines that recommend use of biologics in severe CRSwNP in circumstances when other treatment options have failed, which would include OCS and doxycycline as short-term early interventions before considering biologics [9].
Aside from differences in additional treatments between biologic users and non-users, there were also variations in biologic use between patients with versus without sinus surgery. Although the mean number of biologic claims was similar between these two groups, patients with surgery had fewer days on biologic therapy, suggesting sufficient symptomatic relief and/or enhanced disease control compared with those without surgery. During the observation period less than 10% of all patients received sinus surgery, and only 12% of those that did used biologics. The low frequency of surgery observed may primarily reflect the limited observation period in this study; capturing only recent surgeries represents those with a more current and active burden of disease. This low incidence of surgery combined with low biologic use might suggest that when biologics were first being used for CRSwNP, they were less likely to be used in patients with a disease burden high enough to necessitate surgery, or that “salvage surgery under biological protection” was not routinely considered due to lack of empirical evidence to support this approach [7]. For patients who used biologics after surgery, they did so within a relatively short time (~ 3 months). This potentially reflects a failure of surgery, or early attempts to combine therapies. Therefore, biologic use within 6 months after surgery might mean these patients were having reoccurrence of NP, which is common in CRSwNP [15], or they are simply receiving biologics as an add-on maintenance therapy for inadequately controlled CRSwNP [18,19,20]. For non-biologic treatments, OCS and intranasal corticosteroid use were higher in biologic users versus non-users in the 30 days before surgery but not in the 30 days after surgery. Preoperative OCS use might have been a more common approach in biologic users versus non-users, possibly due to the higher disease burden that biologic users likely represent [8, 13]. Together, these findings suggest biologics are frequently used alongside OCS but less commonly with sinus surgery. In the cases where biologics and surgery were used together, biologics were used soon after surgical intervention, which could indicate a more aggressive approach to care.
This study had some limitations. Several relate to the use of databases, such as data entry errors and therefore potential underestimates, although provider reimbursement schemes minimize this risk. Similarly, the results are subject to data coding limitations, which might explain why the percentage of patients with chronic rhinosinusitus is low, considering NP without CRS is rare. Categorizing both acute and chronic respiratory conditions together when assessing the proportion of patients with multiple common respiratory conditions may have overestimated the proportion of patients with overlapping conditions, compared with if overlapping chronic inflammatory conditions had been assessed separately. There was an absence of patient data before the identification period, so patients recorded as having ‘no’ or ‘earliest’ biologic use, sinus surgery, or other CRSwNP treatments may have received these before the study period; a longer pre-study observation period would have allowed for the capture of these records. The source population receives private insurance, which may not reflect the general population in the US. There were no data on lifestyle factors or CRSwNP symptoms that might have influenced treatment decisions. Beyond database-related limitations, the exact reasons for biologic use were mostly unknown as several biologics reported in this study were not approved for CRSwNP during the study period. Despite this, biologics were likely prescribed for one of the comorbid conditions and less so for chronic idiopathic urticaria, atopic dermatitis, and Eosinophilic granulomatosis with polyangiitis (EGPA) that had low patient numbers. A similar limitation would apply to the CRSwNP-related OCS use, although we used a robust surrogate assessment to identify CRSwNP-related OCS use (e.g., OCS claims must be within ± 5 days CRSwNP-related inpatient claim) it is possible that some claims may have been inaccurately identified. In addition, the use of over-the-counter treatments, such as intranasal corticosteroids, was likely underestimated [43, 44]. A longer study period would have provided greater insights towards the relationship between biologics and SoC. As this study covered a time period close to the first approval of biologics for the treatment of CRSwNP, market factors, such as payer policies, may have influenced the study findings. However, it is worth noting that more recent data would potentially be subject to confounding from the COVID-19 pandemic; biologic use may have changed since the period described in this study.

Comments (0)