Study design and participants
We performed a retrospective cohort study using data from the Diagnosis Procedure Combination database in Japan. This database, based on the medical fee reimbursement system, contains discharge abstracts and claims data from over 1000 acute care hospitals [10]. This dataset represents more than half of Japan’s annual inpatient admissions, covering approximately seven million cases per year, including 24 of the 27 hospitals with PICUs. It includes patient characteristics, Japan Coma Scale scores [11], diagnoses, comorbidities, treatments, administrative information, and discharge outcomes. Diagnoses were recorded using International Classification of Diseases 10th Revision (ICD-10) codes. Studies validating the Diagnosis Procedure Combination data against medical chart reviews have shown a specificity of 93.2% and a sensitivity of 78.9% for primary diagnoses, with both specificity and sensitivity for recorded procedures exceeding 90% [10, 12]. The Institutional Review Board of the University of Tokyo approved this study (approval number: 3501-(5); May 19, 2021), and the requirement for informed consent was waived because of the use of anonymized data.
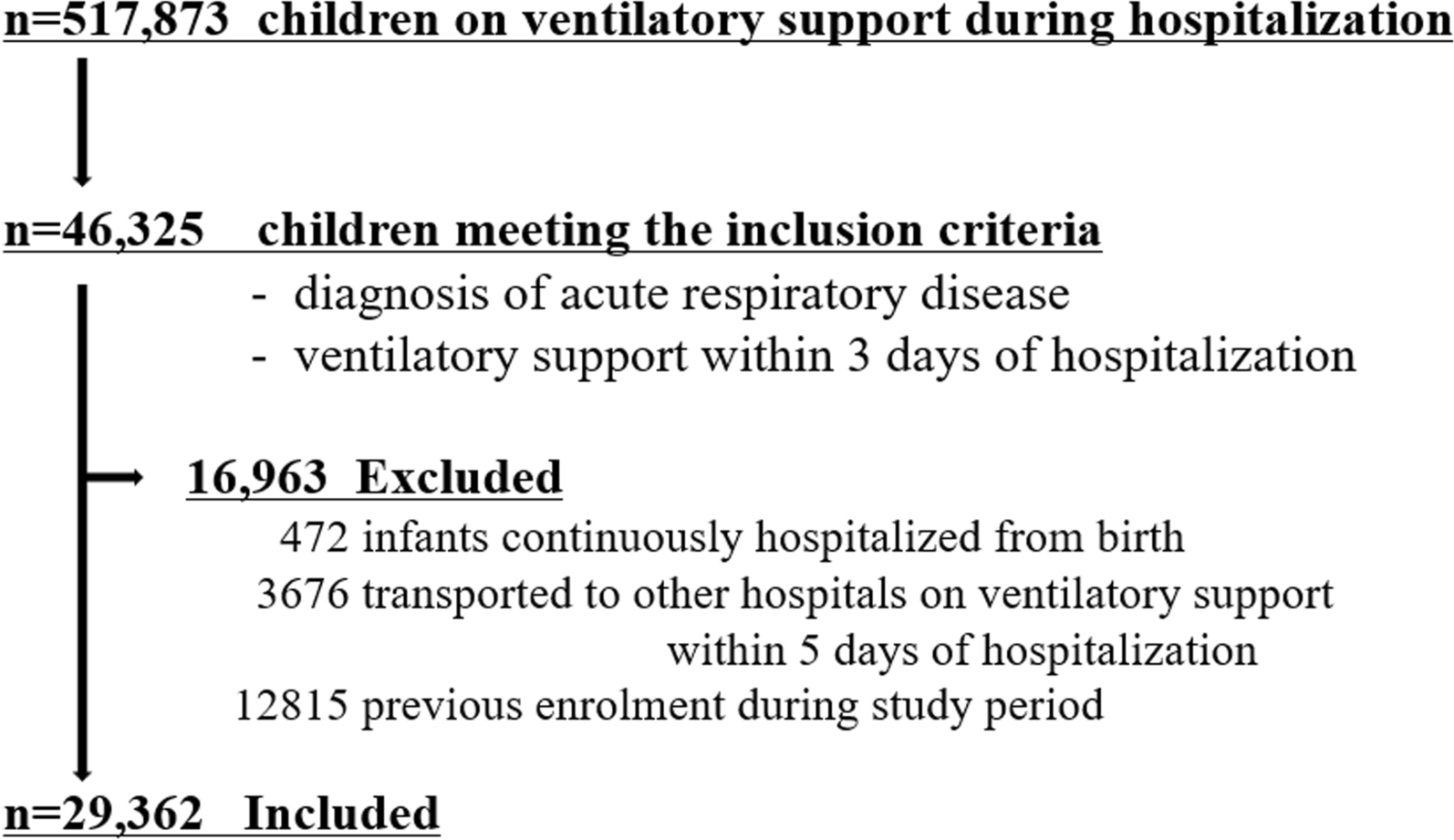
We included children aged < 20 years who were admitted to acute care hospitals with acute respiratory diseases under primary or admission diagnoses between July 2010 and March 2022, and who received ventilatory support, including invasive ventilation, non-invasive ventilation, and high-flow nasal cannula, within the first three days of hospitalization. The study included a range of respiratory diseases categorized as pneumonia (ICD-10, J09-J18, J69.0, J80, J96.0, J96.9, U04.9, U07.1), bronchiolitis (J20-J22, J40), asthma (J44-J46), and other diseases such as croup (J05), tracheitis (J04.1, J04.2), pertussis (A37), and lung abscess (J85, J86).
The following exclusion criteria were applied: (i) infants hospitalized continuously from birth, (ii) patients transferred to other hospitals on invasive ventilation within 5 days of admission, and (iii) previous enrolment during the study period.
Outcomes and covariates
The primary outcome was a composite of unfavorable outcomes, defined as in-hospital death or discharge with new comorbidities, specifically tracheostomy, home ventilation or oxygen therapy, tube feeding at discharge or the day before, gastrostomy during hospitalization, worsened neurological status based on the Japan Coma Scale score at discharge, and renal failure, defined as the need for renal replacement therapy within three days of discharge.
Other variables included patient characteristics and clinical data, such as age, sex, diagnoses, underlying conditions, clinical interventions, and administrative information. Microbiological diagnoses were categorized as viral, bacterial, aspiration, COVID-19, or no detection. We classified the underlying conditions according to complex chronic conditions using ICD-10 codes, and the presence of underlying conditions was defined based on the presence of any of the following conditions: neurological/neuromuscular, cardiovascular, respiratory, congenital/genetic, premature/neonatal, hematological/immunological, malignant, or transplant conditions [13]. Impaired consciousness was assessed using the Japan Coma Scale and categorized into three groups: severe, moderate, and mild, corresponding to scores of approximately 3–8, 9–13, and 14–15 on the Glasgow Coma Scale, respectively [11, 14, 15]. Patients were considered to have acute liver failure if their admission diagnosis included ICD-10 codes K72.0, K72.9, or K76.3, and thrombocytopenia/coagulopathy if they included ICD-10 codes D65, D68.9, D69.5, or D69.6 [16]. Hospital volume was defined as the number of eligible children in each hospital during the study period, and was categorized into tertiles (low, medium, and high). According to the Japanese administrative claims system, accredited intensive care units (ICUs) include PICUs, neonatal ICUs, general ICUs, emergency ICUs, and intermediate care units.
Statistical analyses
We used multivariable logistic regression models to identify early predictors of composite unfavorable outcomes and in-hospital mortality, using generalized estimating equations to adjust for clustering within hospitals. As studies reporting predictive factors for unfavorable outcomes in pediatric respiratory failure are scarce, studies including critically ill children were also referred to select study covariates. The study covariates included patient characteristics (age and underlying conditions), respiratory diagnostic category [8], therapies provided within three days of hospitalization (invasive ventilation, vasoactive drugs, corticosteroids, extracorporeal membrane oxygenation, renal replacement therapy, cardiopulmonary resuscitation, and surgery), and organ dysfunction on admission (level of consciousness, acute liver failure, thrombocytopenia/coagulopathy) [17,18,19]. We also included microbiological diagnoses (viral, bacterial, aspiration, COVID-19, no detection), transport from other hospitals, admission to accredited ICUs within the first 3 days of hospitalization, and hospital volume to adjust for pathogenic and administrative variables. The variance inflation factor was calculated for each covariate to evaluate the multicollinearity of the study covariates. To ensure the robustness of the primary analysis, we performed sensitivity analyses by (i) including only patients requiring invasive ventilation, (ii) excluding patients with bronchiolitis, and (iii) excluding patients with underlying neurological/neuromuscular conditions. All statistical analyses were performed using STATA 17 (StataCorp LLC, College Station, TX, USA).



Comments (0)