We conducted a retrospective cohort study using a nationwide administrative in-patient database in Japan approved by the Ethics Committee of Yokohama City University (F220300054; approved July 22, 2022). This study adhered to the ethical standards of the responsible committee on human experimentation (institutional or regional) and the 1975 Helsinki Declaration. Informed consent from individual patients was waived because of the anonymous nature of the data, and the study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement [18].
Data source
We obtained relevant data from the Japanese Diagnosis Procedure Combination (DPC) in-patient database, which came to include discharge abstracts and administrative claims data for ~ 1200 acute-care hospitals as of 2019, covering ~ 90% of all tertiary-care emergency hospitals in Japan [19]. At hospital discharge, the attending physician recorded the following clinically relevant data that the database captured for each patient: age, sex, diagnoses, daily procedures (Japanese medical procedure codes), drugs administered daily, and admission and discharge statuses. The database categorizes six diagnostic groups, each limited to specific recordable diseases, using the International Classification of Diseases, Tenth Revision codes (ICD-10). Diagnoses are coded under the four classifications “main diagnosis”, “admission-precipitating diagnosis”, “most resource-consuming diagnosis”, and “second resource-consuming diagnosis”. Additionally, up to four diagnoses may be coded as “comorbidities present at admission” or “conditions arising after admission”. It is essential to assess whether the disease names recorded in the DPC database correspond with clinical diagnoses. Various validation studies of the DPC database have shown high sensitivity and specificity for documenting procedures and high specificity with moderate sensitivity for diagnoses [20, 21]. The sensitivity for the diagnosis of respiratory diseases was 22–100%, whereas specificity consistently exceeded 95% [22].
Study population
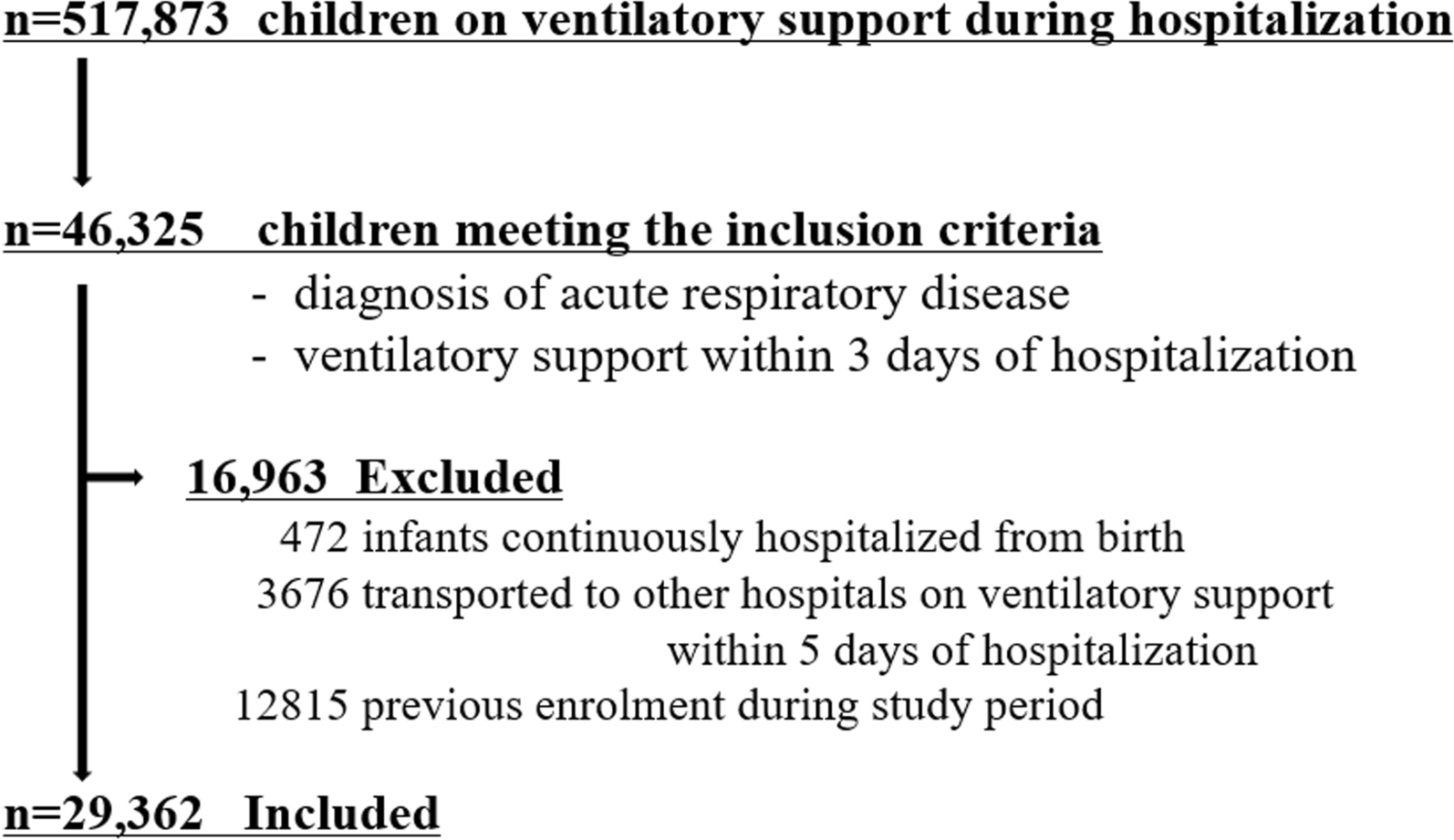
Patients discharged between April 1, 2016, and March 31, 2020, were screened for inclusion. The inclusion criteria included (i) mechanical ventilation (MV) for 4 consecutive days within the first 7 days of admission and (ii) a diagnosis of acute respiratory diseases with possible bilateral lesions (recorded in “main diagnosis”, “admission-precipitating diagnosis”, “most resource-consuming diagnosis”, “second resource-consuming diagnosis”, or “comorbidities present at the time of admission”, see Table S1 for a list of diagnostic codes). A 4-day duration of MV was used as a surrogate for severe hypoxemia due to the DPC data limitations that offered no details beyond 4 days and were supported by previous acute respiratory distress syndrome research [1]. Disease names indicating possible bilateral lesions were clinically determined and manually extracted from the ICD-10 codes. In clinical practice, it is often challenging to diagnose a single definitive cause of severe respiratory failure, and the past ARDS diagnostic criteria did not require the identification of an underlying disease aside from congestive heart failure. Based on these considerations, all types of acute respiratory failure diseases were included in our study. The exclusion criteria included (i) age < 18 years, (ii) cardiopulmonary resuscitation on the first day of MV, (iii) diagnosis of heart failure or congestion (recorded in “main diagnosis”, “admission-precipitating diagnosis”, “most resource-consuming diagnosis”, or “second resource-consuming diagnosis”, see Table S1 for a list of diagnostic codes), and (iv) any surgery performed other than tracheostomy. Postsurgical cases were excluded due to the DPC data's lack of specific reasons for MV, addressing potential non-respiratory failure-related MV needs.
Exposure variables
Patients treated at a hospital with a board-certified intensive care training facility were included in the certified group. Patients in the certified group were not necessarily treated at the ICU, even if they were admitted to that hospital. Accreditation of board-certified intensive care training facilities by the Japanese Society of Intensive Care Medicine (JSICM) during the study period required at least one full-time intensivist in an ICU with a minimum of four beds, regardless of the treatment modalities provided. Board certification status was determined by referencing the annual report in JSICM’s domestic journal [23].
Covariates
We collected data, including age, sex, body mass index, emergency admission, ambulance use, smoking status, diagnosis of acute respiratory disease, and 17 diagnoses for the Charlson Comorbidity Index [24]. We also collected the use of vasopressors and extracorporeal membrane oxygenation on the first day of MV to assess the severity of respiratory and circulatory failure.
Treatment after mechanical ventilation initiation
We collected data on treatments administered within the first week of MV, including sedatives (dexmedetomidine, propofol, midazolam), opioids (fentanyl, morphine), neuromuscular blockers (rocuronium, vecuronium), vasopressors (noradrenaline, dopamine, arginine vasopressin), inotropic agents (dobutamine, phosphodiesterase inhibitors, adrenaline), sivelestat (approved in Japan for acute lung injury), methylprednisolone categorized by dosage (high-dose ≥ 500 mg, low-dose ≤ 200 mg), antibiotics, and antifungal drugs. For sedative drugs, opioids, neuromuscular blockers, and vasopressors, the collected information on the first day of MV was excluded to avoid confusion with medications used for intubation. Additional data collected included bronchoalveolar lavage during hospitalization, early enteral nutrition (defined as implementation within 48 h of MV initiation), enteral nutrition within 7 days, parenteral nutrition within 7 days, early rehabilitation (defined as implementation within 72 h of MV initiation), extracorporeal membrane oxygenation during hospitalization, renal replacement therapy during hospitalization, ICU admission, and high-care unit (HCU) admission. The ICU was defined as a separate unit for critically ill patients staffed with at least one onsite physician around the clock and a nurse-to-patient ratio of 1:2. The HCU is a separate unit with at least one in-hospital physician available 24/7 and a nurse-to-patient ratio of 1:4 or 1:5. A critical care unit admission was defined as any case in which a patient was admitted in either the ICU or HCU.
Outcome variables
The primary outcome was in-hospital mortality, and secondary outcomes included reintubation within 7 days of extubation, tracheostomy during hospitalization, total MV duration, ICU stay length, HCU stay length, and overall hospital stay. Additionally, for survivors, MV dependency was assessed at discharge, which was defined as ongoing invasive MV.
Statistical analysis
The study results are presented as median (interquartile range [IQR]) or number (%), as appropriate. Missing data for four baseline characteristics—weight in 4856 cases (7.3%), height in 6215 cases (9.3%), ambulance use in 71 cases (0.1%), and smoking status in 10,510 cases (16%)—were assumed to be missing at random and were imputed by the missForest algorithm [25, 26], using all variables except timing of tracheostomy and CCU length of stay listed in Tables 1, 2, 3, and sTable 2 as predictors. This method, which is based on a random forest, iteratively handles missing data [25, 26]. It starts with the column with the fewest missing values, filling other columns with mean values to use as predictors. This process is repeated for each column until a stopping criterion is met. In our study, a single dataset created using this method enabled the main analysis, sensitivity analysis, and subgroup analysis to be conducted. We performed propensity score matching to adjust for confounding by indication and the potential baseline differences between the certified and non-certified groups [27, 28]. The propensity score for treatment at a hospital with a board-certified intensive care training facility was calculated using the logistic regression model confounders listed in Table 1 and Table S2 (age, sex, body mass index, emergency admission, ambulance use, smoking status, diagnosis of acute respiratory disease, 17 diagnoses for the Charlson Comorbidity Index, and the use of vasopressors on the first day of MV, and extracorporeal membrane oxygenation on the first day of MV). Propensity score matching was used to balance the two groups in a 1:1 ratio without replacement. This was achieved using the nearest neighbor algorithm with the caliper width set to 0.10 of the standard deviation of the logit of the propensity scores. Group balance was assessed using the absolute standardized difference. Covariates with absolute standardized differences < 0.10 were considered well-balanced. All reported P-values were two-sided, with a P-value of less than 0.05 considered statistically significant. Owing to the potential for type I errors from multiple comparisons, findings from secondary outcomes and subgroup analyses were considered exploratory. Missing data imputation was performed using R (version 4.1.0; R Foundation for Statistical Computing, Vienna, Austria), and all other statistical analyses were performed using STATA version 16.1 (StataCorp, College Station, TX, USA).
Table 1 Baseline characteristics of patients with severe respiratory failure on mechanical ventilationTable 2 Interventions for patients with severe respiratory failure on mechanical ventilationTable 3 Outcomes of patients with severe respiratory failure on mechanical ventilationSensitivity and subgroup analyses
To avoid sample size reduction due to the propensity score-matched analysis and estimate the average treatment effect, we performed two sensitivity analyses using the stabilized inverse probability of treatment weighting method [28] with propensity score and logistic regression analysis for in-hospital mortality in the original cohort. In the logistic regression model, we included the same variables used in the propensity score calculation. The results were presented as median differences or odds ratios with 95% confidence intervals (CIs).
We also performed subgroup analyses according to age (≥ 80, 79–70, 69–60, or ≤ 59 years), use of vasopressor on the first day of MV, and admission to critical care units. We assumed that the impact of intensivists on patient care varies according to patient age, severity of illness, and treatment location, therefore, selecting these subgroups. These subgroup analyses were performed in the original cohort using the logistic regression model for in-hospital mortality. We also tested for an interaction between each subgroup and the certified group. Finally, we analyzed the interaction between each subgroup and the certified group. The interaction term for age was modeled with age as a continuous variable.



Comments (0)