Our nationwide web-based survey investigated current policies and practices of tube feeding in HNC patients among different treatment centers in Germany. It provides valuable insights into the characteristics and opinions of healthcare professionals, specifically radiation oncologists, medical oncologists, and ENT surgeons/otolaryngologists. More than 70% of our respondents stated that they neither conduct routine nutritional screening nor that they rely on SOPs concerning EN management. However, over 80% of the respondents support the insertion of prophylactic PEG tubes before planned CRT.
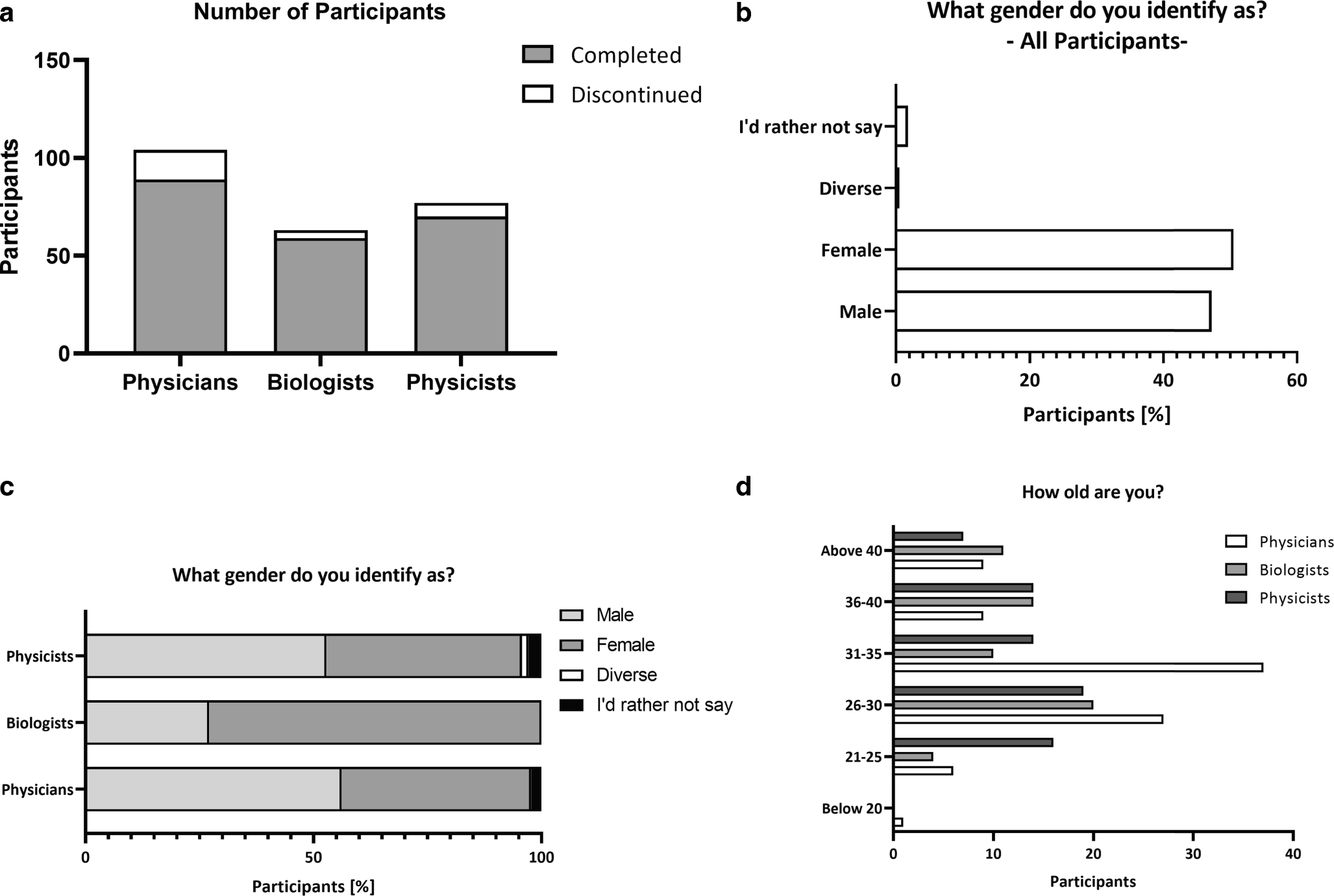
Our study included 70 physicians from various specialties involved in HNC care. Most participants worked at low- and intermediate-volume centers (with fewer than 50 or up to 100 HNC cases per year, respectively), and were mostly affiliated with university hospitals. This distribution reflects the diverse backgrounds of healthcare providers involved in the management of HNC patients and also underlines the structure of the German healthcare system: in addition to university clinics or hospitals that are certified cancer centers alone or in a network, outpatient treatment can also take place in specialist private practices. However, data have shown that the treatment of HNC patients at high-volume centers was associated with a survival benefit [22, 23]. Although the definition of a high-volume center varies across different publications, these data apply to surgical as well as to conservative (including radiotherapy) disciplines, emphasizing that interdisciplinary experience matters [24]. However, the importance of nutritional medical support or nutritional counselling services is not addressed in these analyses. The uneven distribution in terms of our participants’ patient volume (or cases/year) underlines the need for standardized protocols not only in oncologic treatment decision-making but also in the management of nutritional complications.
Our study revealed that a significant proportion of participants do not perform standardized nutritional screening before planned CRT. There are several studies that confirm the benefits of pretherapeutic nutritional screening [25, 26]. According to our experience, this non-performance of a pretherapeutic nutritional screening is not attributable to a general physicians’ rejection, but rather to workload compression and staff shortage in the German healthcare system.
Since dysphagia may lead to malnutrition, which, in turn, may negatively impact overall survival of head and neck cancer patients [27], radiation-induced dysphagia remains a focus of ongoing scientific research. Accordingly, there are not only several studies on its prevention [7, 8], but also on the correct timing of PEG tube insertion. The Swall PEG study is particularly noteworthy here [12]: as a randomized, controlled phase III study, its primary endpoint investigated patient-reported outcomes related to swallowing and patients’ health-related quality of life. The authors have announced their intention to publish their results in a peer-reviewed journal [12]. Other efforts address the avoidance of radiation-associated dysphagia by means of optimized radiation planning (dysphagia-optimized intensity-modulated radiotherapy) with dose constraints to the superior and middle pharyngeal constrictor muscle or inferior pharyngeal constrictor muscle up to a mean dose of 50 Gy. The results imply that this dose-sparing of the swallowing muscles leads to an improvement in patient-reported swallowing [7].
There is a preference for prophylactic PEG tube placement among most our respondents, which aligns with the notion that early placement may reduce the risk of malnutrition and hospital readmissions [28]. Yanni et al. performed a retrospective analysis of 152 patients undergoing surgery, radiotherapy, or chemotherapy due to HNC. These authors concluded that PEG tubes were advantageous regarding hospital readmissions, relative weight loss at 6 weeks, dysphagia, severe malnutrition, and the patients’ health status [28]. On the contrary, Madhoun et al. surveyed HNC patients between 2004 and 2006. They reported a high number of unnecessary PEG tube placements when feeding tube insertion was performed prophylactically. Thus, only 47.8% of their patients with prophylactic PEG tubes either did not use their feeding tube at all or used it less than two weeks [29]. Overall, the correct timing of PEG tube placement remains a controversial point of discussion that should be weighed individually depending on the existing nutritional risk factors. Of course, this presupposes that the risk factors are known or have been determined within the framework of an individual nutritional risk screening [26].
Interestingly, we noticed differences between radiation oncologists and other disciplines regarding the indication setting and the use of SOPs. The proportion of radiation oncologists using an SOP appeared to be lower compared to other specialties. Although this finding could be biased by the imbalance between the professional groups, possible reasons for this could lie in the dynamic field of radiation oncology: Rapid changes in treatment practices may outpace the development or updating of SOPs, leading radiation oncologists to rely more on evolving evidence and expert consensus rather than fixed SOPs. Therefore, the unique and individualized nature of radiation therapy, interdisciplinary collaboration dynamics, the evolving nature of treatment practices, and the absence of universally accepted guidelines in certain contexts may lead to a lower use of SOPs regarding the indication for enteral feeding tubes.
SOPs aim at identifying potential risks and outlining preventive measures. Risk management is recommended to ensure safety and quality in radiation oncology [30, 31]. Bearing in mind that available data are still limited on the topic of risk management in German radiation oncology, published data on the handling of enteral or parenteral feeding due to radiation-induced dysphagia are also very sparse. Although some of our respondents follow internal institute SOPs on this topic, the majority of our interviewed radiation oncologists do not use SOPs, thus implying a potential need for standardized guidelines to warrant consistent and evidence-based decision-making regarding radiation-induced swallowing complications.
Our respondents’ opinions on the use of PEG tubes varied, with the majority indicating that the use of feeding tubes should remain unchanged. Notably, radiation oncologists favored an increasing use of PEG tubes, possibly driven by concerns about treatment interruptions due to severe treatment-related toxicities. This viewpoint has been reflected by some studies suggesting that prophylactic PEG tube placement may reduce treatment interruptions [32] and improve outcomes [33].
Overall, the abovementioned perspectives reflect the ongoing debate in the literature regarding the appropriate use and timing of PEG tubes [29, 34]. A significant proportion of our participants reported severe complications associated with PEG tube placement. This underscores the necessity for careful consideration of risks and benefits before PEG tube insertion. Severe complications including infection and dislodgment as well as tube-related morbidity and (in rare cases) even mortality have been reported previously [14]. For decision-making, the EHNS-ESMO-ESTRO (European Head and Neck Society - European Society of Medical Oncology - European Society for Radiotherapy and Oncology) clinical practice guideline can be a source of support: in case of present malnutrition (defined by a weight loss of more than 10% over 6 months before diagnosis), an enteral feeding tube is recommended. When long-term feeding tube dependence is foreseeable, PEG tubes should be preferred over nasogastric tubes [35]. Moreover, there are some publications that at least provide information on other factors relevant for development of dysphagia and, thus, dependence on a feeding tube during ongoing therapy. These factors include the radiation dose to the swallowing muscles or the radiation volume [11, 36, 37] and the tumor localization [38], as well as weight loss at diagnosis [11] and age [11]. Although validated nutritional screening tools focusing on weight loss exist [9], there are no validated universal risk scores that combine radio-oncologic risks (e.g., radiation dose to the swallowing muscles) and clinical/nutritional risks (e.g., weight loss in the past 6 months).
The different perspectives are also reflected in the patient cases described: in question no. 13, our respondents were asked to decide whether they would rather have a PEG or nasogastric tube inserted if their patient presented with (otherwise uncontrollable) dysphagia 4 weeks after starting chemoradiotherapy. The same question about the chosen method of reactive tube feeding was asked in the Scandinavian survey by Ilmarinen et al. [17]. Their survey included otorhinolaryngology head and neck (ORL-HN) surgeons and oncologists (including medical oncologists and radiation oncologists). Most of their participants (> 65%) would have chosen a nasogastric tube over a PEG tube. Interestingly, 63% of our participants would have opted to have a PEG tube inserted. The tendency to use a PEG tube in this situation also prevailed in the interprofessional comparison in our survey. This discrepancy between the two studies may be due to the chosen subject collective. While in the survey by Ilmarinen et al., no explicit distinction was made between radiation oncologists and medical oncologists, radiation oncologists dominate in our survey. It is well known that side effects after chemoradiotherapy often persist for several weeks after the end of treatment. Therefore, we assume that this was the reason why our respondents decided to have a PEG tube inserted.
In question no. 16, our participants were asked which tube-feeding strategy they would choose in a 55-year-old male patient suffering from p16-positive squamous cell carcinoma of the base of the tongue (cT2 cN1 cM0) with a BMI of 25 kg/m2 and without significant weight loss, history of pain, or swallowing problems, when chemoradiotherapy is planned [17] (55% percent of our Scandinavian colleagues preferred a reactive nasogastric tube [17]). For a 65-year-old male patient with hypopharyngeal carcinoma (cT2 cN2b cM0) and swallowing difficulties, 67% of the Scandinavian respondents opted for a prophylactic PEG tube. For both situations, no differences were observed between head and neck surgeons and oncologists by Ilmarinen et al. [17]. In both cases, German physicians mostly preferred a prophylactic PEG tube (62.9 and 88.6%, respectively).
The third and last patient case described the case of a 59-year-old patient with right-sided oropharyngeal carcinoma (good general health, BMI of 23 kg/m2), who opted for a transoral resection with neck dissection. Participants were asked how to proceed regarding tube feeding. There was no clear trend regarding one option. We were surprised that a prophylactic PEG tube was also considered in 27.1%.
Although our survey on PEG tube placement in head and neck cancer patients undergoing CRT provided valuable insights, there are limitations to be acknowledged. Firstly, the study’s sample size, consisting of 70 respondents, may not fully represent the diverse range of German healthcare professionals involved in HNC treatment. Therefore, our findings may not be generalizable to all practice settings. Our survey is based on participant opinions and their practices, which does not guarantee guideline adherence. Accordingly, we were dealing with self-reported data and cannot exclude a recall bias. An important limitation is the disbalance between the professional groups: since radiation oncologists predominate in this case, conclusions drawn from the SUFFEETUBE project cannot be generalized automatically to other medical specialties. At the same time, we were able to show that an unequal approach to feeding tubes exists throughout Germany (irrespective of the professional group). This insight may provide an impetus for standardization and the development of guidelines. At the same time, it must also be emphasized that not all clinically active ENT physicians, oncologists, and radiation oncologists throughout Germany were contacted. Therefore, a selection bias cannot be ruled out.









Comments (0)