The success of chemoimmunotherapy as second-line treatment for advanced or metastatic ESCC, and even as the first-line standard treatment, has prompted research into the possibility of adding radiotherapy to triple therapy. The synergistic anti-tumor mechanism of radiotherapy and ICIs has served as the basis for combining radiotherapy with standard chemoimmunotherapy. In previous clinical studies on chemoimmunotherapy for advanced or metastatic ESCC, the reported incidence of pneumonitis was 7%, and the incidence of grade 5 pneumonitis was between 0 and 1%.
The patients included in the ATTRACTION-03 study and ESCORT study both had ESCC, among which 70 and 64% had received radiotherapy, respectively [3, 4]. In the ATTRACTION-03 study, the incidence of pneumonitis was 9.2 and 5.6% in the nivolumab group and chemotherapy group who received radiotherapy, compared with 7.0 and 7.6% in those who did not receive radiotherapy, suggesting that radiotherapy may increase the risk of pneumonitis after ICIs [3]. However, there is no secondary analysis in patients who have previously thoracic radiotherapy currently. The incidence of pneumonitis was 7.8% (6/77) in the Japanese subgroup treated with pembrolizumab and 6.5% (4/62) in the Chinese subgroup [20] in KEYNOTE-181 [19]. However, no study further analyzed squamous cell carcinoma patients who had previously received thoracic radiotherapy. These summative data reveal that there is lack of comprehensive analysis of pulmonary toxicity after thoracic radiotherapy combined with ICIs in Asian patients with ESCC.
After conventionally fractionated radiotherapy, the first radiological manifestation of radiation pneumonitis is expected to occur within 6 months, and approximately 15% of patients develop pneumonitis within 2 to 3 months [21, 22]. The median onset time of immune pneumonitis was 2.8 months after the initiation of ICIs [23]. However, for patients receiving thoracic radiotherapy combined with anti-PD‑1 mAbs, it is usually difficult to clearly distinguish between radiation pneumonitis and immune pneumonitis in clinical practice. Therefore, the endpoint of our study was TRP. A subgroup analysis of a meta-analysis that involved six clinical trials showed that the incidence of grade 3 or higher pneumonitis was 1.9% in patients with locally advanced esophageal cancer who were received concurrent and sequential CRT/RT and ICI [24]. However, the use of this combination therapy in trials may not reflect the real-world data. The results of this study corroborated the tolerable pulmonary safety of combined therapy. Although the incidence of pneumonitis was much higher than that reported in previous studies, it was mainly low grade. A secondary analysis of the phase I trial KEYNOTE-001 [13] showed that although thoracic radiotherapy increased the probability of pulmonary toxicity (12.5% vs. 1.4%), the incidence of high-grade pulmonary toxicity was similar (4.2% vs. 1.4%).
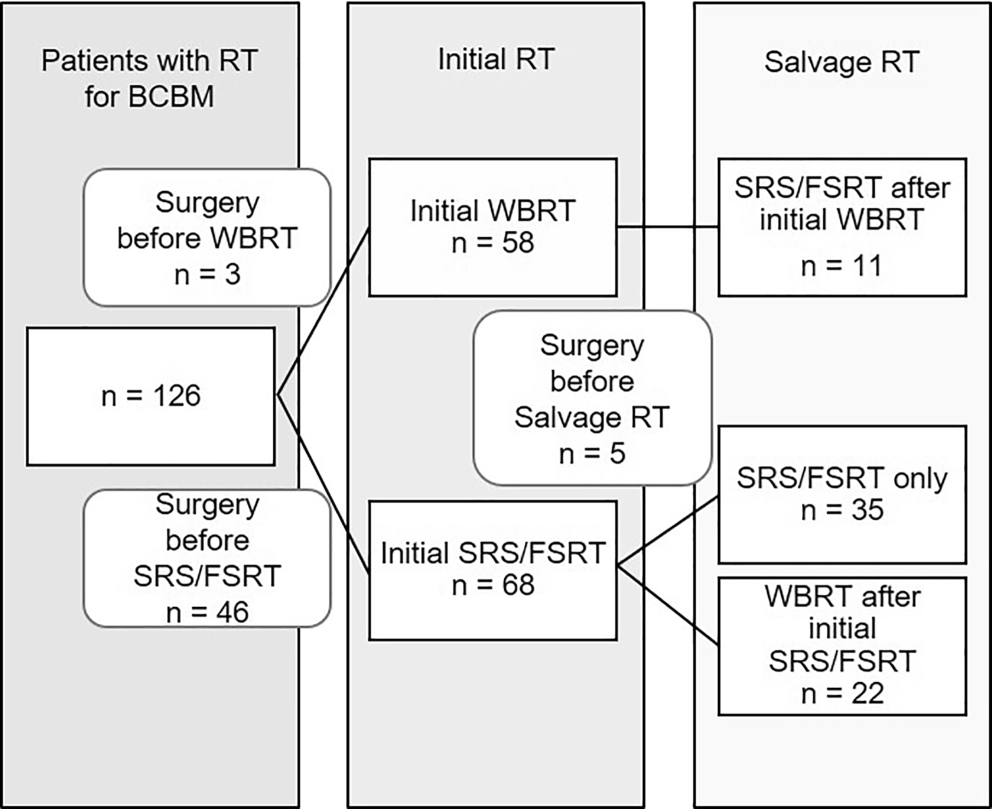
The primary novelty of this study pertains to include the patients who received concurrent radiotherapy/chemoradiotherapy plus anti-PD‑1 mAbs, which is very rare even compared to other analogous studies of lung cancer. In this study, 28 of 41 patients with stage IV ESCC received concurrent therapy. Chemoimmunotherapy is the standard treatment for stage IV ESCC. For this population, palliative RT could alleviate dysphagia. Additionally, some retrospective studies had shown that delivering RT to primary tumor could might improve survival [25, 26]. There were 13 of 56 patients with stage III ESCC also received concurrent ICI. The reason was that our institution has been involved in the ESCORT-CRT study since 2020, and we observed the acceptable toxicity in enrolled patients. Owing to the significant therapeutic effect of ICI in stage IV patients, some stage III patients wanted to receive standard CRT combined with ICI. Therefore, ICI was applied, and all patients signed the consents for this concurrent treatment. This retrospective study also serves to support the potentially practice-changing of the ongoing KEYNOTE-975, ESCORT-CRT, and RATIONALE-311 studies in confirming the pulmonary safety of definitive chemoradiotherapy combined with ICIs. It is worth noting that two published studies have explored concurrent radiotherapy/chemoradiotherapy plus camrelizumab as first-line treatment for locally advanced ESCC [27, 28], the incidence of pneumonitis was 11–15%, among which the incidence of grade 3 pneumonitis was 0–5%, and no grade 4–5 pneumonitis occurred, However, it was still limited to the small sample size (19 and 20, respectively) of phase Ib studies. It has been reported that the incidence of grade 2 radiation pneumonitis after definitive radiotherapy in esophageal cancer is 9.6–20.3%, and the incidence of grade 3 is 1.8–7.4% [29,30,31]. As compared to definitive radiotherapy, the addition of immunotherapy seems to maintain similar pulmonary toxicity rates. On the other hand, Zhang, et al. [32] reported that the application of anti-PD1 drugs before or during thoracic radiotherapy increased the incidence of radiation pneumonitis (27/45 vs 14/50, 60% vs 28%, P = 0.01). In fact, it is unclear whether there are toxicity differences between concurrent and sequential administration of RT/CRT in combination with ICIS in ESCC patients. More clinical trials and real-world data may be needed to confirm the concept. Our study showed that anti-PD‑1 mAbs administered concurrently with radiotherapy was associated with the incidence of grade ≥ 2 TRP. Although the incidence of grade 1–2 pneumonitis was considerably higher than existing data, the patients in our study received a prescribed PTV dose of 50.4–66 Gy, whereas the prescription PTV dose adopted by Zhang, et al. was 54 Gy [27, 28]. Overall, the pulmonary toxicity in patients with concurrent RT/CRT plus anti-PD‑1 mAbs in our study was tolerable, however, in clinical practice, close toxicity monitoring and follow-up should be conducted according to patients’ age, lung dose, lung function and the history of chronic lung disease, etc. in order to achieve longer survival benefits and better quality of life.
In the HOPE- 005 study [18], 41% (52/191) of patients with pneumonitis received corticosteroids, of whom 22 received immune rechallenge, and only 6 patients relapsed with grade 1–2 pneumonitis. Although the largest cohort reported that pneumonitis was associated with a higher recurrence rate (27.7%) than other types of irAEs [33], no severe recurrence of pneumonitis was observed in the HOPE-005 study. In our study, five patients underwent immune rechallenge, and only 1 patient developed grade 3 pneumonitis. Considering that treatment-related AEs of any grade were associated with higher ORR [34], and continuous application of ICIs for more than 1 year may improve clinical outcomes [35], immune rechallenge may be a viable treatment option.
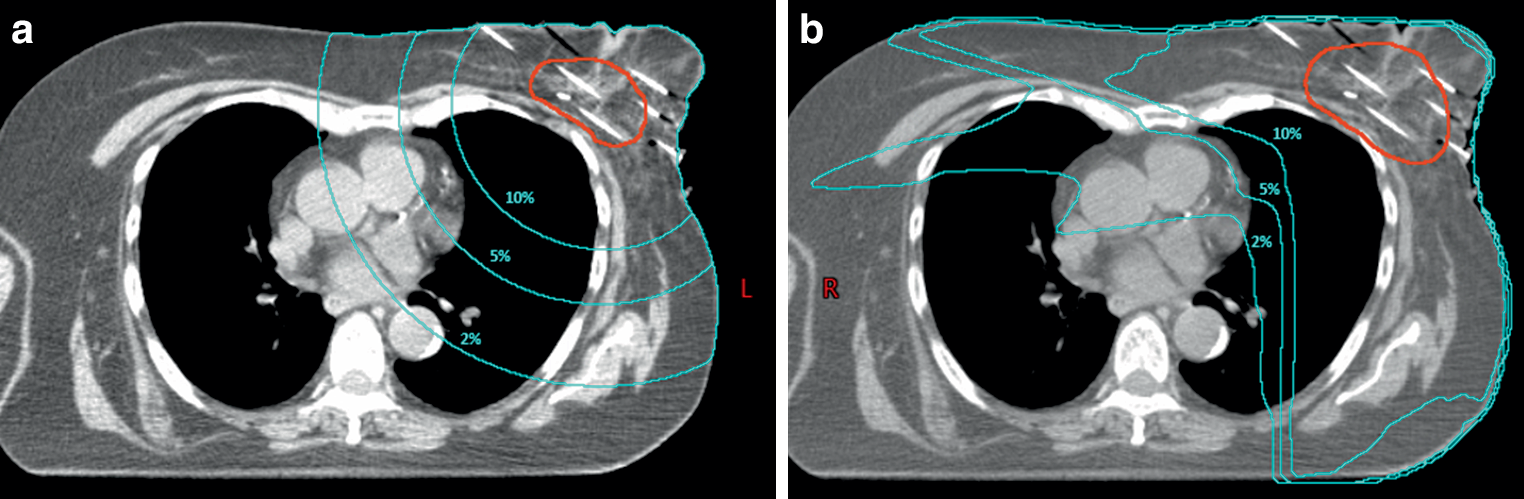
DVH parameters (e.g., MLD and V20) can predict symptomatic radiation pneumonitis in patients with esophageal cancer who receive definitive chemoradiotherapy. The combination of ICIs and thoracic radiotherapy may amplify the risk of pulmonary toxicity. Therefore, it is more urgent to formulate constraints based on dosimetric prediction factors in the era of ICIs. There is still a lack of correlation analyses between pneumonitis and DVH parameters in patients with ESCC treated with thoracic radiotherapy combined with ICIs. In the analysis of radiotherapy combined with immunotherapy for NSCLC, conclusions regarding the relationship between DVH parameters and TRP are inconsistent, and no specific threshold for DVH parameters is recommended. Several studies have reported that V20 and MLD are associated with TRP [17, 18, 36]. However, another retrospective analysis from Japan showed that the incidence and severity of pneumonitis in NSCLC patients receiving concurrent chemoradiotherapy followed by durvalumab consolidation therapy were not related to total lung V20 [37]. Similarly, Lu et al. [38] reported that V5, V20 and MLD were not associated with the occurrence of TRP in 196 patients who received thoracic radiotherapy prior to ICIs from Chinese lung cancer cohort. Because of the rare and controversial results of related studies, it is important to identify predictors of pneumonitis after combined therapy to provide reliable data references. To our knowledge, our study is the first to define dosimetric relationships between lung dose-volume parameters and TRP after thoracic radiotherapy combined with ICIs in Asian patients with ESCC. A major finding herein was that V5, V10, V15, V25, V30, V35, V40, and MLD were associated with grade ≥ 2 TRP and V5 was an independent risk factor. This implies that V5 is a noteworthy predictor in addition to high-dose region, which is inconsistent with the general lack of validation in the non-ICI setting. One of the hallmarks of IMRT is its ability to improve consistency in the intermediate- and high-dose region by spreading the low dose-irradiated volume, thereby increasing the lung V5 [39]. IMRT was associated with a better lung toxicity profile compared to 3D-CRT [40]. The larger low dose-irradiated area of IMRT did not appear to cause more severe lung injury. But the findings of this study indicate that the intensive low dose-irradiated volume appears to be more associated with TRP after adding ICIs. That novel finding maybe due to the fact that ICIs plus RT could activate the immune system, so that even a “low dose bath” could cause pneumonitis. In this study, all patients received IMRT. Therefore, both intermediate- and high-dose region and low dose region should be treated with caution under the premise of the combination of radioimmunotherapy. The overall lung toxicity will be determined by a tradeoff between these two trends. Through the aforementioned caveat, extra care should be taken to limit V5 to less than 55% in IMRT planning to reduce the incidence and severity of TRP.
There were some limitations in our study. First, this was a retrospective study which might have distorted the results due to unmeasured confounding factors, selection bias and heterogeneous populations. In this analysis, patients were enrolled in single institution, and the sample size was relatively finite. Second, this study did not include the population who received thoracic radiotherapy after prior ICIs due to the heterogeneities of patients as well as the small sample size precluding further stratification analysis. This remains an issue requiring further investigation. Third, although we found that V5 was an independent risk factor for G2+TRP, the AUC value of 0.722 implies medium predictive value, which may also be limited by the small sample size. Further analysis with an enlarge sample size is needed to confirm our observations. Fourth, the literature reported that the median onset time of ICI-related pneumonitis was 19.2 months [23], while the median follow-up time in our study was 12.3 months, which should be remedied by a longer follow-up. Therefore, it is possible that this study still underestimates the occurrence of overall TRP, along with the fact that death is a competing risk factor for TRP in the population with poor prognosis. Fifth, there was insufficient data in this study for a robust statistical assessment of immune rechallenge. Thus, the outcome of the immune rechallenge must be interpreted with caution.



Comments (0)