Identifying the issues faced by the young workforce is an essential step towards improving the satisfaction of all subspecialties and improving the willingness to not only get involved but also to continue an active career in the field of radiation science. Despite physicians comprising the largest of the subspecialties according to the overall number of employees in Germany, it was especially biologists and physicists with a very high participation in the survey [2]. The overall high involvement during a rather short period of 6 weeks in comparison to similar studies [23, 24] indicates that there is potential, ambition, and interest among the younger employees to identify problems and improve the field of radiation oncology and radiation research over the next decades.
Our study revealed that each of the subspecialties has distinct problems (e.g., the contractual situation for biologists), while other factors are present cross-disciplinarily and thus need to be addressed by the societies as a whole.
Subspecialties specific problemsBiologists
Radiation biology, despite not being present in all departments, makes a tremendous contribution to the field of radiation oncology and radiation protection by providing knowledge of dose fractionation, tumor hypoxia, tissue weighting factors, and radiation quality [25, 26] as well as regarding the optimized use of combination therapies. Radiation biologists have helped to define parameters needed for risk and exposure assessment, thus establishing dose limits and offering mechanistic explanations for outcomes observed in radiation epidemiology that provide the pivotal translation of laboratory data into human applications. Insights gained by radiation biologists are used in clinical work for radiation protection, diagnosis, risk assessment, and treatment. While our survey reports that most participants see only mediocre career options and about 40% even worse career opportunities than in other biological fields (Fig. 4), one has to point out that the insights and knowledge gathered can be used not only in the public health domain but also for military purposes, space exploration, environmental stewardship, and national security, and also provide biological and biophysical information on radiation response to federal agencies setting exposure limits for workers and the general public. This can of course be used for creating job opportunities, and the gathered knowledge can be used as a transition into other scientific fields or jobs outside of the field of radiation oncology. In these cases, career seminars might be helpful in order to point out alternative career options for biologists working in radiation research. In this way, well-trained high-potential staff will not get lost to other disciplines or subjects but will find ways to remain in radiation research outside of the medical field. An uncontroversial fact is that securing research funding, which is often challenging to obtain, places a significant burden on employees, as it is an essential element for maintaining a position and providing the potential for career advancement, especially in biological research [14]. The probability of funding, on the other hand, is strongly determined by strong mentorship, establishment of a collaborative network of scientific and clinical expertise within the host department, and scientific input from related departments both within the host department and from external institutions. Besides typical support with data analysis, biostatics, literature, and article writing, intensified help in preclinical animal studies with exceptionally hard and complex legal and ethical regulations should be considered [9]. At the moment, the majority of postdocs are forced to cover their position using grant money, which basically makes them cheap, smart, and highly educated labor [27]. Short-sighted hyper-competitive environments potentially even slow down scientific innovation and productivity and favor fabrication and publication of immature data, thereby wasting valuable resources. High expectations and success—despite the low probability of success in the whole research environment, ranging from grant applications to hiring decisions and career progression—strongly depend upon publications, which encourages scientific dishonesty [28]. Improvement can be achieved by preparing trainees for different potential career paths, teaching training skills that can be used outside of the academic world, creating communication platforms, and giving postdocs more visibility and thus possibilities to be more proactive about their career. Another approach could be to optimize the postdoc salary with cost-of-living adjustments [29]. Improvements need to be made towards individual grant application by postdocs and improving grant evaluation for younger researchers with lesser-known names and reputations, thus enabling high-potential scientists to focus on research instead of writing grants [28]. The harsh working conditions are very well reflected by the low percentage of participants in our survey who would choose radiation biology again. In combination with the mediocre career options and even worse-perceived employment options overall compared to other biological research fields (Fig. 4), attracting high-potential biologists to the field is becoming more challenging. However, as a high number of individuals in our survey are unsure about whether or not to remain in radiation research, it is evident that adequate measures can aid in keeping these individuals rooted in radiation research.
(Medical) physicists
Physicists represent the second largest cohort of employees involved in the field of radiation oncology. A regulatorily required number of (medical) physicists is of utmost importance for the safety of patients and the quality of radiation treatment. Important tasks carried out by physicists range from administrative and clinical services to informatics, equipment maintenance, and performance evaluations, as well as research, teaching, and training. The past has shown that implementation of new techniques like intensity-modulated radiotherapy (IMRT) leads to an increased demand for physicists [19, 30, 31]. Despite being of such great importance, very few new academic positions are being created in research and education in health care physics and medical physics overall [32]. Nevertheless, the profession will likely continue to further increase in importance, mostly due to the vast amount of new technology that will need to be implemented into current treatment protocols. In the present survey, physicists show the highest willingness to leave academia and transition into industry, while private practices are the employers least favored by physicists, which could be biased as participants of the survey are mostly employed at university hospitals. However, the fear of less challenging and versatile cases as well as repetitive daily tasks in peripheral institutions could also be a reason for this. As well-trained physicists can easily transition into other work fields, it is an essential task to better include these specialists in the society and keep these individuals in the field of radiation oncology in order to remain competitive in the years to come, as inadequate staffing will inevitably lead to loss of quality and safety in the long run. One possible way to achieve long-term commitment could be an increase in the permanent contracts offered by institutions. Physicists represent the subspecialty with the highest percentage of permanent contracts in the survey, which seems to reflect the particular need for long-term integration of well-trained personnel into workflows of the respective departments to ensure consistency and reliability, but also the legal requirements for the presence of MPEs. It remains unclear why a large percentage of (medical) physicists are not members of a society (Fig. 8). It may be possible that bachelor’s/master’s students, due to their early career stage, and non-scientific MPs may not see any representation of interests in a scientific society. As there is a lack of a professional association for clinically working medical physics experts in Germany, the offer of (interdisciplinary) education and interaction for this group should eventually be further expanded within the existing scientific associations. At the same time, this may increase interest and active participation in the societies and strengthen interdisciplinary and translational cooperation between research and clinical settings. In general, the cohort of physicists seems to be rather satisfied with their career choice, reporting the highest percentage of participants who would choose the same specialty again and high satisfaction rates regarding the support offered by the employer (Fig. 3). Only the subjective workload in science tends towards being higher compared to the physician cohort.
Physicians
Physicians are the largest cohort and also represent the subspecialty with the highest visibility due to the direct patient contact. In our survey, the most prominent fear among physicians is high economic pressure followed by a lack of work–life balance and compatibility of career and family (Fig. 4). Regarding the general economic situation, lower financial reimbursement combined with higher costs for personnel, energy, and maintenance cause significant economic stress in the different departments. Profit targets set by the hospital administrations are a balancing act between the economic situation and a reasonable treatment for patients. In Germany, a large cohort of patients undergo treatment within private practices, which due to newer rules, regulations, and alterations in billing could possibly put those practices under significant economic pressure in the future, especially as insurance companies try to cut costs overall [4]. Another significant point defining employee satisfaction is the subjective or perceived workload. The present survey shows that especially physicians have the highest subjective workload among all subspecialties (Figs. 5 and 6). Recent studies report that a continuously high workload can lead to depression and loss of workforce in the long term, resulting in a negative public perception of the field [33,34,35]. As especially research work outside of regular working hours can contribute to the workload, protected research time needs to be implemented using specialized programs or research grants.
Common problems in the younger workforceWork–life balance
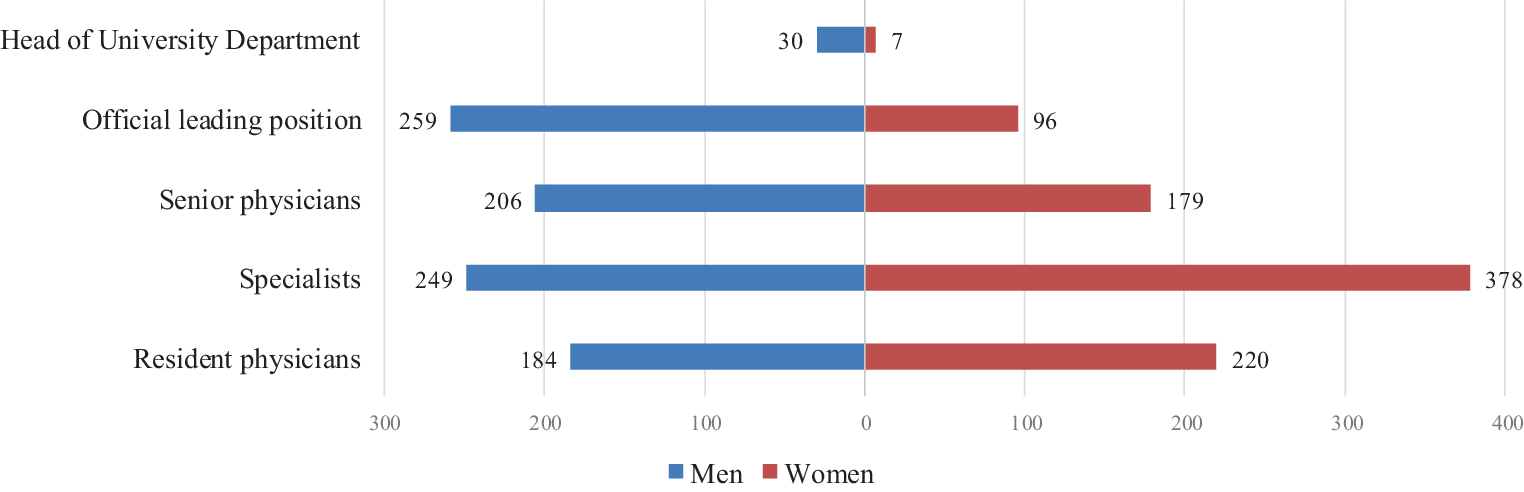
Another topic that needs to be addressed for all subspecialties in the future is the creation of a job environment with an adequate work–life balance, as this is one of the major concerns of the physician and physicist cohorts in our survey. Compatibility of career and family, especially with a higher number of female professionals (Fig. 1), paired with significant changes in classical family roles, is also increasing in importance. The possibility of working part-time is an essential factor, facilitating better adaptation to private circumstances such as nursing a family member or taking time out for childcare. Another possible solution is implementing the concept of a 4-day working week that is currently discussed [36, 37] and even being tested in some clinics in Germany. While the biologist cohort shows a fair number of employees working part-time, this is rather unusual for the physician group, which shows the highest rate of full-time employment (Figs. 5 and 6). However, as doctoral candidates in biology or medical physics are employed part-time while usually working full-time, an in-depth analysis of these factors will need to be carried out in the future. Thus, this is in most cases only a pro-forma part-time contract, while PhD students actually work full-time. True part-time contracts might, however, increase the attractiveness of the field through improved work–life or work–family balance. The high percentage of full-time-employed participants in the physician group could possibly be explained by the need of finishing a residency program as the final step of their education. In the future, more liberal part-time models should be offered and will be inevitable as more and more female employees strive into the field. Working part-time in general needs to become more accepted by supervisors independent of gender to enable contemporary gender-equal divisions of labor and non-classical family roles.
Working environment
The most favored form of employment in this survey is academia among all subspecialties (Fig. 4). One possible explanation could be that academia combines clinical, scientific, and teaching work, in contrast to non-academic clinics or private practice, and offers the chance to work in a cutting-edge and up-to-date environment that is usually less economically driven. University hospitals offer, besides a basic education, the possibility to acquire further scientific education, helping to implement new results into daily work as paradigm changes can occur very fast in modern medicine [38, 39]. However, the structure of universities overall will not make it possible for all participants to pursue a career in academia. Further considerations discouraging long-term academic careers include academic pressure, declining support for research, and increased bureaucracy [17, 40, 41], as also visible in the present study (Fig. 4).
Potential points of improvement
A survey by Krug et al. about the young radiation oncology workforce showed that only 4% of participants reported a complete separation between clinical work and research and/or teaching activities. Among these, physicians reported the lowest number (9%) of protected time to carry out research or teaching in their regular working hours on a regular basis [2], suggesting that most of the time, teaching and research are carried out outside of regular working hours. This can potentially become problematic, as the quality of research and teaching but also of clinical work might suffer when tasks are mainly carried out outside of regular hours and during overtime [42].
Research
One possible point for improvement is the creation of easier options for entry into scientific work. While the volume and intensity of research will differ significantly between facilities, barriers impeding participation in research have to be clearly addressed. Obstacles that are frequently mentioned range from lack of time, limited access to statistical analysis through insufficient mentoring, and variable support from superiors, to great variability in research productivity at the department level, partially due to metafactors such as the size and composition of the department, advanced technology capability, limited access to funding, and the numbers of patients and degree of engagement with specialist medical research institutions [43]. The present survey confirms that especially employees in the physician cohort lack protected research time (Fig. 7). Combined with the fact that overtime in work covering the clinical routine is becoming the rule rather than the exception, this makes it virtually impossible for clinicians to engage in high-quality and pioneering research [4, 44]. Furthermore, according to our survey, physicians and physicists are less frequently involved in the supervision of doctoral students compared to biologists. This can be attributed to a higher level of clinical involvement and responsibilities; likewise, it is possible that these groups are more involved in the supervision of bachelor’s or master’s theses. As scientific work is time consuming, an approach to include mainly clinically working personnel in research, thus giving them an overview of current trends and developments outside of their daily work, could be to involve them in the reviewing process of scientific work after respective training. Other countries require medical candidates to complete mandatory scientific work before their final examination. In the case of clinical medical physicists in training, completion of a scientific project or an additional study before becoming eligible for certification could be obligatory—an approach that has been successfully implemented in the model medical study course in Cologne, Germany [45,46,47]. Another recent improvement in this regard is the introduction of young scientist scholarships, enabling physicians to take protected research time as a clinician scientist [48], which could significantly improve the situation. This is especially important as fundamental research on combining radiation therapy with other treatment modalities like surgery and chemo-/immunotherapy will become more and more important in the future. Intensifying translational work cooperations will be an inevitable component of this.
Teaching
Likewise, lectures on physics and biology have to be implemented into standard residency programs to generate a basic understanding of the mode of operation of, e.g., immunotherapies, and to foster awareness of possible cooperations and interactions between subspecialties [49]. Furthermore, the satisfaction of trainees with their occupational training is of utmost importance for choosing a certain career path. Participants from the medical field that were asked about their educational quality in our study, however, report a broad range of satisfaction, with a median of 65/100 (Fig. 3). There is a significant number of participants that seem to be highly satisfied with their education versus 29% of participants reporting satisfaction rates of below 50. One option could be to hold written and oral examination on the topics of radiation biology and radiation physics early during residency, following the example of the radiation protection course. These results could also give more feedback to the teaching institutions from an educational standpoint [50]. Cooperations between biologists and physicists also need to be intensified, as new radiation-generating devices show increasing complexity, requiring formal training in basic principles of radiation dosimetry and measurement for research.
Our survey further reports that the involvement of physicians and biologists in teaching is higher than that of the subcohort of physicists (Fig. 2). While medical physics most likely will continue to grow in importance due to increasing numbers of cancer cases as well as further scientific improvements leading to advanced technologies that increase the demand for well-trained professionals [51], the high number of participants not involved in either teaching or scientific work is problematic and needs to be improved in the future.
Mentoring and networking
One quarter of participants indicate insufficient support for their career goals, potentially causing them to leave the field in the long term. Among the participants, the cohorts of biologists and physicists seem to be a lot less prone to communicating their potential career goals to their employers (Fig. 3), which could be interpreted as either being less career oriented or as being less informed regarding the possibilities in the field. Here, career courses could be an option to inform and train staff to better identify and communicate their goals. Another possibility might be a widespread implementation of mentoring programs that pair young professionals with those more experienced in the field who often have a more widespread network and can offer pivotal guidance in personal, clinical, and academic growth. Especially mentoring has been frequently mentioned during the current survey. The supervision by mentors could help to create a meaningful timeline for reaching certain milestones and complementary educational achievements such as a basic education in health care economics, as often required for higher positions [52], especially as mentors can give advice independently of the department’s own interests. Recently, the young scientist groups have reacted to this topic and offered a mentoring program for all three subspecialties involved in radiation oncology, highly supported by older members of the society in Germany.
Future developments and generational change in radiation oncology
Another point that needs to be discussed is how the clinical demand will change as a response to growth in the cancer incidence (approximately 2.5% per year), the impact of new technologies with possible acceleration of treatment-related workflows due to artificial intelligence, but also possible slowing of processes due to more adaptive and individualized treatment regimens [3]. While future developments cannot be entirely foreseen, technical progress, which holds great potential for improvements in treatment overall, is not seen as a significant problem, neither by the physicist nor by the physician cohort (Fig. 4). In contrast, new technologies can even lead to an increase in treatment time. Models and further predictions show that a 5% increase in overall workload could potentially lead to a significantly higher number of staff needed from all involved specialties [3]. One example is the increase in demand for medical physicists due to the introduction of new technologies and an increased number of treatment machines [19, 53, 54]. Combined with a general shortage of personnel due to aging of the existing workforce, which can only be compensated to a very limited basis, this could lead to a real decline in treatment capacity, safety, and overall quality. Limitations could be reduced through the extension of work contracts or consulting and by increasing the number of open clinical training positions for MPEs [30, 53, 54].
While a lack of potential employers is present for a large variety of specialties, overall competition for motivated and well-trained employees due to suboptimal working conditions and payment level compared to some other European countries is inevitable. Radiation oncology will probably not be given more attention in undergraduate life science education, thus limiting its visibility to potential future employees at that early stage of their career path. Therefore, advertising the field by offering good and diversified training programs with a wide range of additional offers could serve as a letter of invitation, convincing potential candidates to take their decision in favor of radiation oncology in the end. In contrast to a lack of potential employers, the generational change benefits investor-managed hospital and practice chains primarily focusing on increasing margins rather than prioritizing improving patient treatment.
Radiation oncology is underrepresented in oncological teaching in medical schools, which leads to underutilization and a lot of prejudices towards the field, while studies show improved knowledge with dedicated courses, especially favoring clinical exposure over dedicated lectures [37, 55, 56]. The lack of knowledge potentially even impedes multidisciplinary oncological care. Furthermore, a recent study demonstrates that the introduction of radiation oncology into the preclinical part of medical education is feasible [57], an idea that is generally well perceived by students [58]. This may aid in attracting more doctoral candidates and residents while improving overall knowledge in radiation oncology. Possibilities to teach radiation oncology outside of the existing curriculum include special lectures, seminars, and bedside training as well as the meaningful integration of e‑learning [59]. Teaching in biology and medical physics is generally less frequent [24]. The decision to choose a certain specialty is driven by different intrinsic (personal interest) and extrinsic (perceived prestige or potential income) as well as structural considerations like the influence of lifestyle, working hours, perceived stress from on-call duties, amount of time on-duty, and the possibility to work part-time. Although no one single factor can be seen as decisive, a beneficial combination of exactly these points could give the field of radiation oncology the edge, especially for students still undecided at the end of their studies [60]. Awareness and basic knowledge in these fields, however, also needs to be established amongst general practitioners to provide patients with adequate advice and information [24].
The role of societies
Another promising step towards improvement is the creation of networks among younger professionals within the framework of existing societies. The creation of internal groups linking young radiation oncology scholars has been successfully implemented in other European countries [9]. Structured collaboration between new and advanced professionals within the society can further address essential points such as the drafting of a good residential curriculum, including reliable long-term rotation plans covering all relevant aspects of clinical radiation oncology and naming individuals responsible for the supervision of residency training. Another possibility would be the creation of improved teaching including lecture series covering all the major relevant topics in oncology in a location-independent approach, ensuring that all residents can benefit from the knowledge of local specialists. Such a step was recently taken by the young DEGRO in Germany and has been met with a very positive response [42, 61].
Teaching, which is often not standardized throughout the different departments, has been further compromised by the COVID pandemic [42]. The young DEGRO group has implemented online courses covering different topics in physics, biology, and clinical radiation oncology. The courses so far have been very well received, inviting new aspiring scientists and clinicians to present a talk on their research focus. A similar program is found in the DGMP and young MP, while the young DeGBS focuses on online seminars covering topics such as how to set up a lab or introduction of committees. Points that have to be further addressed include more time for self-study; increasing support by the DEGRO, DGMP, and DeGBS; participation in meetings; improved educational quality; and an institutional training schedule that focuses more on the guidelines drawn up by the German medical council [61,



Comments (0)