
Remember me


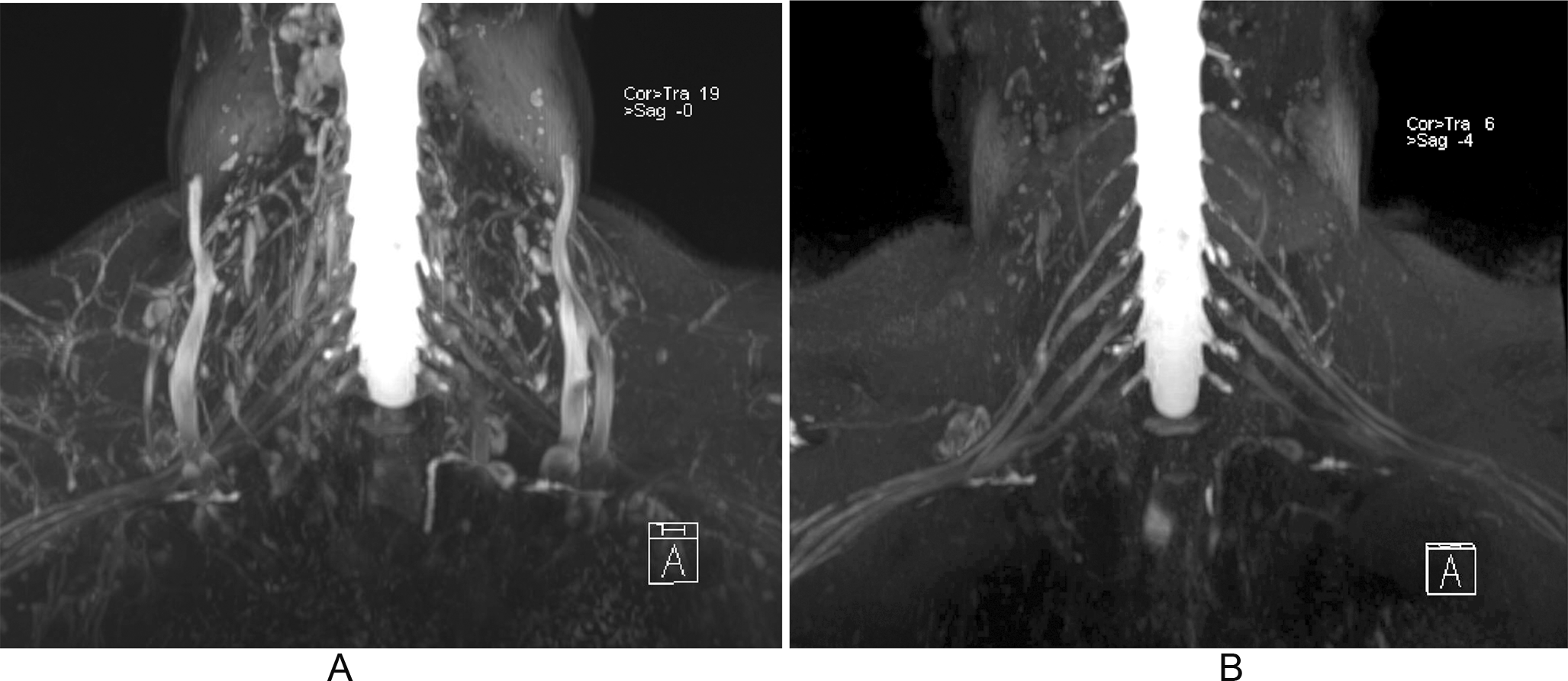

In this study we presented that MPR MRI measurement of the anterior glenoid lesions is valuable for some measurement and but has some limitation for more complex assessment. It has very good reliability for linear parameters, but does not seem very good for assessing the glenoid defect area (and therefore Pico index). MRI imaging, due to its obvious benefits and improved quality, is becoming a valuable alternative to CT imaging in orthopedics even for bone evaluation. Some studies show that both may have comparable quality for assessing the glenoid bone loss, thus making MRI a radiation-free alternative to preoperative shoulder scans [6, 8, 19]. Yet some still have concerns regarding this method [20] (Fig. 3).
Fig. 3
Example of difference in measurements between two investigators on the same MRI scan
Generally speaking, imaging techniques reflect reality better than 2D. Studies on glenoid measurements using CT showed that 3D imaging has excellent reliability for all studied glenoid parameters, while 2D had acceptable results only for some of them [7]. 3D imaging appears to facilitate proper glenoid plane alignment and more accurate measurements. Results for MRI are less conclusive. We couldn’t find any studies directly comparing 3D and 2D MRI for glenoid assessment. Some conclusions can be drown from the studies comparing MRI and CT. A study comparing 2D MRI and 2D CT showed that both techniques have almost similar results for glenoid width, anterior straight line length and glenoid bone loss [21]. Comparison of 3DMR and 3DCT measurements showed that there is no significant difference between the two techniques for some glenoid parameters - surface arena, height and width (although very small number of images were studied, only 7, with artificially created bone loss - cadaveric study) [22]. The MPR MRI used in our study, although not a full 3D reconstruction, allows proper positioning of the glenoid. Measurements using this technique do not require special software and time-consuming reconstruction
Our results suggest that linear measurements, such as superior-inferior height or anterior-posterior width, are characterized by very high reliability. They are easy to learn, even for inexperienced researchers, to measure accurately. The problem arises with more complex, area measurements such as the Circle area or Eroded area, which directly influence the Pico index. Although the technique for performing these measurements seems simple, significant differences between researchers arise. There seem to be a lot of room for arbitrary and subjective assessment of best fit circle based on not very sharp contrasts on MR scan. This problem was observed in previous studies, which showed that additional steps (such as extending a line perpendicular to the midpoint of the supraglenoid tubercle across the glenoid) can be added to improve the reliability of Pico measurements [23]. Moreover, our study suggests that the accuracy of glenoid measurement depends on experience with this technique. This was also observed in a previous study, where authors stated that the were reliability differences between more and less experienced radiologists [24].
When we compare our results with available literature, partially similar results were obtained in a study by Gyftopoulos et al., which measured glenoid loss using standard 2D MRI. Although limited in sample size (only 18 cadaveric glenoids), the authors showed that for the circle method (Pico), inter-observer reliability is only moderate while intra-observer reliability is excellent. Other parameters were not described in the study [23]. Interestingly, the authors also underline the effect of learning on the accuracy of measurement. This corresponds with our results, which clearly show that experience plays a crucial role in glenoid measurement. Interesting study by Sgroi et al. showed that 2D MRI, for both linear and surface area parameters have very good inter-rater and intra-rater reliability, with no significant difference to CT. The differences between our results may be due to the different approach and technical differences. Study by Sgroi et al. used standard 2D MRI while we used MPR reconstruction. Also observers in cited study started real measurements only when the respective intrarater reliabilities were good. In our study we did not assess the reliability of the researchers' measurement before the actual measurements were taken. Another study by Gyftopoulos et al. discussed the usefulness of 3D MRI for the evaluation of glenoid bone loss. The authors used the 3D-T1W-FLAShaveH sequence, and two observers measured images of 15 patients. The results showed that ICC for PICO inter-observer reliability was very good, which is a better result than what was obtained in our study. The difference might arise from the fact that the authors of the study used "real" 3D reconstruction, while in our study we used MPR MRI, which is a less advanced technique. For other parameters than PICO, we found a study by de Mello et al. which showed excellent inter and intra-rater reliability for glenoid width using 3D MRI. Although the study group comprised only 10 patients, these findings are consistent with our results [25].
Our study seems to be the first one with a relatively large study group (80 patients) and six observers. Most of the studies that we found were based on 20 images or fewer, which should not be overlooked when drawing conclusions. Based on our results, we suggest that MPR MRI should be used cautiously when it comes to glenoid defect measurement using the PICO method. "Real" 3D MRI is a more complex but definitely a better alternative.
MPR MRI seems to be a compromise between 2D and 3D MR imaging. On the one hand, it does not have all the benefits of 3-dimensional imaging, but on the other hand, it is much simpler to produce. There are important differences between MRI and CT techniques that potentially affect the reliability of glenoid measurements. CT images often have higher spatial resolution than MRI images for bone structures. An additional difficulty is the inferior differentiation between bone and soft tissue on MRI. This difference affects measurement reliability and makes MRI more difficult to masters. We think that it might be especially important for young clinicians, who do not have vast experience in glenoid measurements. The reliability of measurement is not independent of the researcher's experience. Although it seems to be less important for 3D imaging [8]. Therefore, we believe that especially young clinicians should have access to 3D techniques that are easier to assess. This conclusion is supported by other researchers [7, 26]. It seems that in the future, limitations in the reliability of glenoid measurements might be solved by machine learning models [27]. Advancements in technology could mitigate the human factor, which appears to be a significant limitation.
Our study has limitations. We have no direct comparison to the gold standard of 3D CT. Such comparison would allow for deeper validation yet would include exposing patients for radiation and at the stage was avoided for the project. The observers involved in the study were not experienced doctors but medical students who underwent previous training on glenoid measurement. Yet on the other hand that allows us to really assess the value of measurement that could be questioned if done be not experienced evaluator. Secondly, the observers were focused on finding glenoid defects, which sometimes might not be present in the images. This could potentially lead to confirmation bias. Yet this was based on set of consecutive instability patients, that represents clinical scenario. In our study we used high resolution, 3 Tesla MRI, with Volumetric interpolated breath-hold examination (VIBE). This is possible only on certain MRI machines. Another limitations of the study and technique of measurements is time of whole process. The procedure is time consuming. That clearly is dependent on the experience of the evaluator. We have not measured the average time of the measurements and that seemed rather obvious. We also believe that in the future machine learning and artificial intelligence will facilitate the whole process. So can be probably achieved with 3D reconstructions based on MR, as we have proven 3D measurement superiority over 2D one.
Comments (0)