
記住我
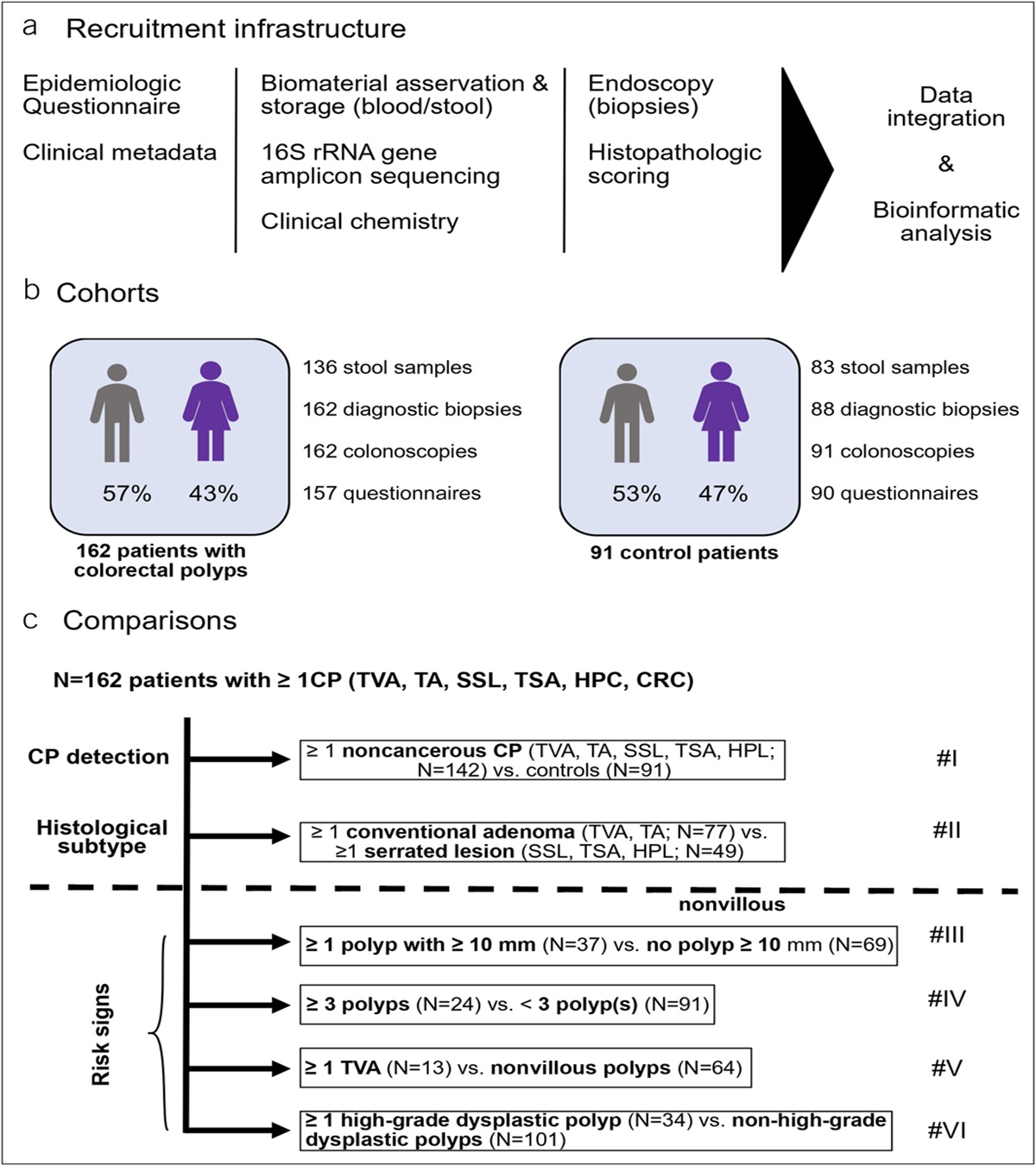
Gastric cancer is one of the most common malignancies worldwide and is the fourth leading cause of cancer-related death (1). China has a high incidence of gastric cancer (2,3). Early diagnosis and treatment greatly improve the survival rate and quality of life in patients with gastric cancer (4). Esophagogastroduodenoscopy (EGD) is an important tool for screening upper gastrointestinal cancer, especially for early-stage tumors. Foam, bubbles, and mucus often obstruct mucosal visibility during EGD, leading to missed lesions and misdiagnosis (5,6). To achieve better visualization, prescribing premedication to eliminate the mucus and foam is necessary (7,8). Currently, whether premedication is necessary and the choice of premedication in different endoscopic centers is not completely consistent (7,9,10). Pronase (mucolytic agent) and simethicone (defoaming substance) are commonly used premedications for conventional endoscopy with favorable results (11–15). However, whether a postural change is necessary for premedication with pronase or simethicone remains unclear. Few studies have examined the efficacy of a postural change on premedication with pronase and simethicone on mucosal visibility. Therefore, we conducted a prospective, single-center, randomized, controlled trial to examine the efficacy of using premedication of simethicone/pronase with or without a postural change on visualization of the mucosa before endoscopy. We aimed to provide new evidence to optimize the use of premedication with EGD.
METHODS PatientsWe enrolled a consecutive series of patients ranging in age from 18 to 70 years, who were referred to the Digestive Endoscopic Center of Tongji Hospital, Huazhong University of Science and Technology for EGD. Patients with any of the following conditions were excluded: (i) a contraindication for EGDs; (ii) pregnancy or breastfeeding; (iii) an allergy to pronase or simethicone; (iv) severe heart or respiratory condition, liver dysfunction, or other life-threatening diseases; (v) liver cirrhosis with esophageal and gastric varices; (vi) active gastrointestinal bleeding; (vii) a history of gastrointestinal surgery; (viii) severe gastric retention; (ix) refusal to participate in this study; and (x) current participation in other clinical trials and in the follow-up or drug washout period.
Informed consent was signed by all participants before enrollment. This clinical trial was approved by the Ethics Committee of Tongji Medical College, Hua Zhong University of Science and Technology (Approval Number: 2020-S303). The clinical trial is registered at the Chinese Clinical Trial Registry (registration number: ChiCTR-IOR-17010985).
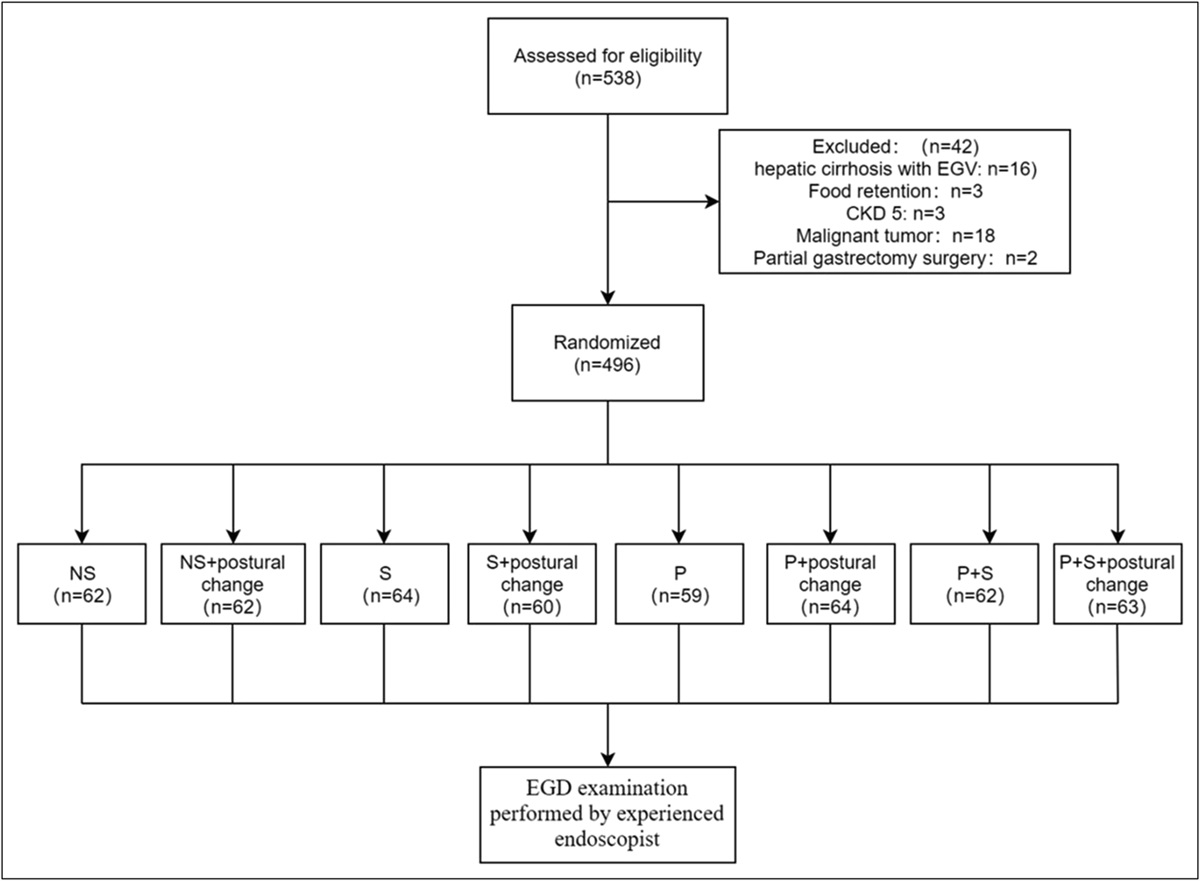
Premedication and endoscopic procedureWe allocated 496 patients into 8 groups by computer-generated random numbers before the endoscopic procedure (Figure 1). These groups were the (i) normal saline (NS) group, (ii) normal saline + postural change (NS + PC) group, (iii) simethicone (S) group, (iv) simethicone + postural change (S + PC) group, (v) pronase (P) group, (vi) pronase + postural change (P + PC) group, (vii) combined use of pronase and simethicone (P + S) group, and (viii) combined use of pronase and simethicone + postural change (P + S + PC) group. The premedication was administered orally approximately 25 minutes before endoscopy. In the NS group, patients received 10 mL of normal saline and 90 mL of warm water. In the S group, patients received 90 mL of warm water and 10 mL of simethicone (containing 40 mg simethicone in 1 mL of emulsion; Espumisan; Berlin-Chemie, Germany); In the P group, patients received 100 mL of warm water and 20,000 IU pronase granules combined with 1 g NaHCO3 to maintain the intragastric pH at 6–8 (Beijing Tide-Pharmaceutical Co., Ltd., Beijing, China). In the P + S group, patients received 90 mL of warm water, 10 mL of simethicone, and 20,000 IU pronase granules combined with 1 g NaHCO3. In the PC groups, the patients were asked to turn over (from the left lateral, supine, right lateral, and prone to upright position and remain in each position for 20 seconds). These movements were repeated several times, and the turn-over time was restricted to 5 minutes.
 Figure 1.:
Figure 1.: Study flowchart. CKD, chronic kidney disease; EGD, esophagogastroduodenoscopy; EGV, esophagogastric varices; NS, normal saline; P, pronase; S, simethicone.
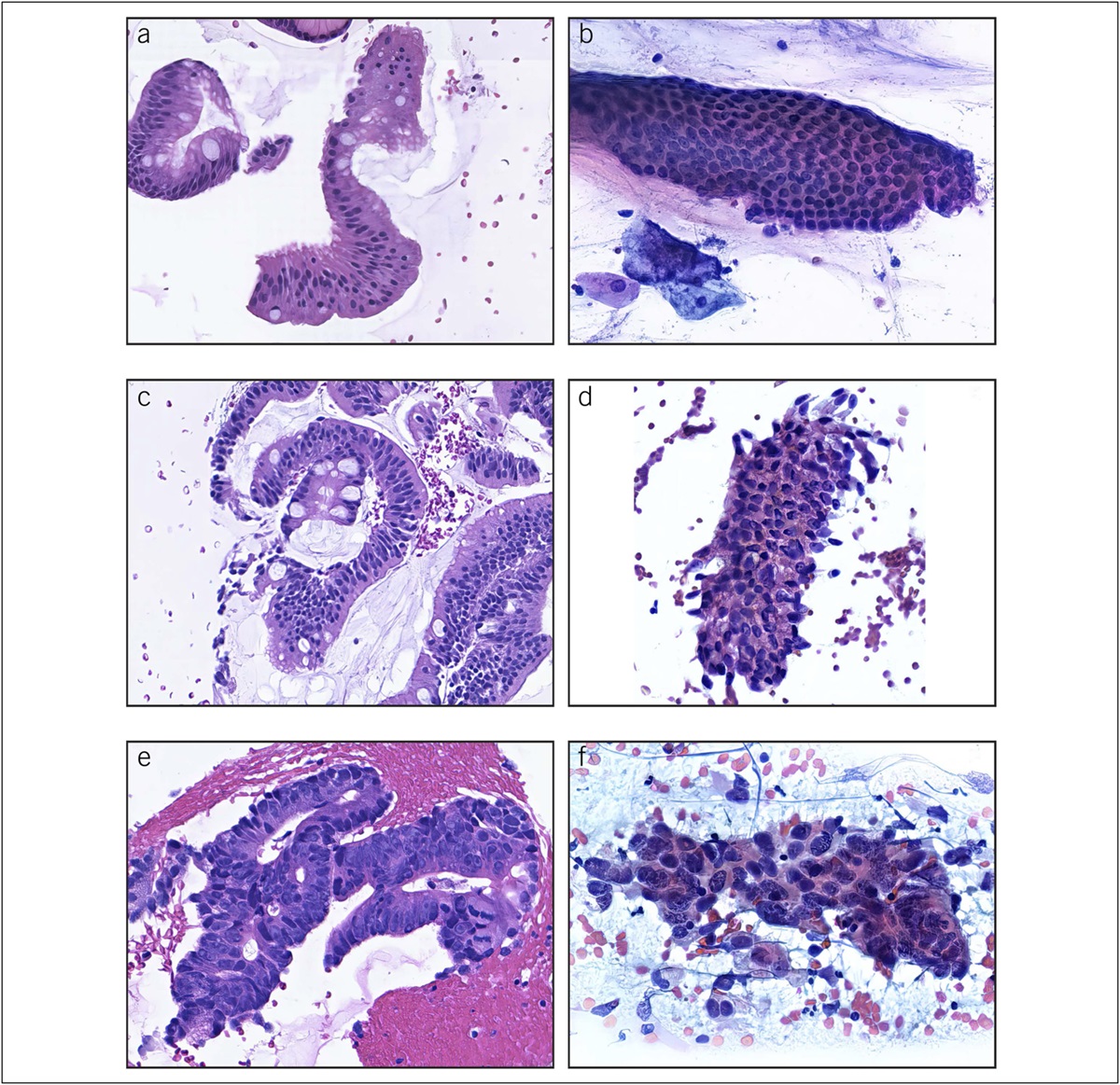
All enrolled patients were sedated and then 3 qualified endoscopists with experience of more than 6,000 EGDs performed EGD in the enrolled patients using a GIF-290 endoscope (Olympus, Tokyo, Japan). The endoscopists were blinded to the premedication used. The endoscopic images were taken separately at the esophagus, cardia, fundus, upper gastric body, lower gastric body, antrum, and duodenum by the endoscopists. A nurse recorded the amount of water consumed for mucosal cleansing, number and location of biopsies, procedure time, and number of diminutive lesions (lesions ≤5 mm) including early esophageal and gastric cancer detected. Adverse events, which were defined as symptoms or signs, such as nausea, abdominal distension, and vomiting, were monitored closely during the EGD procedure. Complications, such as hemorrhage, perforation, and asphyxia, were also recorded. After the procedure, 2 investigators reviewed the endoscopic images and assessed the mucosal visibility score (MVS), and investigators were blinded. The MVS was classified as 1–4 on the basis of standard classification as previously described; lower scores indicated better mucosal visibility (11). The criteria for each location are shown in Figure 2. The sum of the visibility scores for the abovementioned 6 locations was defined as the total visibility score (TVS), ranging from 6 to 24.
 Figure 2.:
Figure 2.: Mucosal visibility score. Score 1: no mucus and foam, clear vision, score 2: a little foam and mucus, clear vision, score 3: More foam and mucus, blurred vision, less than 50 ml of water for mucosal cleansing; score 4: a lot of foam and mucus, unclear vision, 50 ml or more of water for mucosal cleansing (The above figures were all from this study).
Statistical analysisStatistical analysis was performed using SPSS 23.0. Demographic characteristics were assessed using the χ2 test or Fisher exact test. The Shapiro–Wilk test was used to test the normality of quantitative data. The TVS and MVS are shown as the mean ± SD. The independent sample t test was used to compare the MVS and TVS of each area between the groups. Age, the procedure time, and the total amount of water flushing are shown as the median and interquartile range (IQR). The Mann–Whitney test was used for comparing these data between the 2 groups. The Kruskal–Wallis test and Dunn multiple comparison correction were used to compare different premedication groups before EGD. P < 0.05 was considered statistically significant.
RESULTS Demographic characteristics of the patientsWe enrolled 538 patients (275 women, 263 men) in the study. Forty-two patients were excluded in accordance with the exclusion criteria. Sixteen patients had a history of liver cirrhosis with esophageal and gastric varices, 3 had massive food retention, 3 had chronic renal failure, 18 had malignant tumors, and 2 had gastrointestinal surgery. The demographic characteristics of the groups are shown in Table 1. There were no significant differences in age, sex distribution, age, body mass index, histories of smoking, alcohol drinking, irregular dietary habits, hypertension, diabetes, or an indication for endoscopy among the 8 groups (P > 0.05). There were no complications or serious adverse events in any of the groups during the examinations.
Table 1. - Patients' characteristics and indications for EGD Variables NS NS + PC S S + PC P P + PC P + S P + S + PC P Value Patients (n) 62 62 64 60 59 64 62 63 Age (yr), median (IQR) 43 (33, 53) 49 (36, 54) 50 (38, 56) 48 (36, 56) 49 (40, 56) 47 (33, 56) 51 (37, 57) 49 (38, 55) 0.292 Sex, n (%) 0.998 Female 31 (50.0%) 33 (53.2%) 32 (50.0%) 30 (50.0%) 32 (54.2%) 32 (50.0%) 30 (48.4%) 33 (52.4%) Male 31 (50.0%) 29 (46.8%) 32 (50.0%) 30 (50.0%) 27 (45.8%) 32 (50.0%) 32 (51.6%) 30 (47.6%) BMI (kg/m2), median (IQR) 22.0 (20.0, 24.0) 22.1 (21.0, 25.2) 21.9 (19.6, 24.9) 23.8 (20.8, 25.1) 23.2 (20.9, 25.3) 23.7 (21.5, 26.0) 22.7 (20.5, 24.9) 22.6 (20.8, 25.1) 0.203 Smoking, n (%) 6 (9.7%) 10 (16.1%) 8 (12.5%) 9 (15.0%) 5 (8.5%) 8 (12.5%) 7 (11.3%) 10 (15.9%) 0.210 Alcohol drinking, n (%) 4 (6.5%) 3 (4.8%) 0 (0.0%) 4 (6.7%) 2 (3.4%) 6 (9.4%) 4 (6.5%) 4 (6.3%) 0.197 Irregular diet habits, n (%) 11 (17.7%) 7 (11.3%) 4 (6.3%) 8 (13.3%) 9 (15.3%) 12 (18.8%) 3 (4.8%) 7 (11.1%) 0.176 Hypertension, n (%) 4 (6.5%) 6 (9.7%) 9 (14.1%) 6 (10%) 8 (13.6%) 5 (7.8%) 9 (14.5%) 4 (6.3%) 0.614 Diabetes, n (%) 1 (1.6%) 1 (1.6%) 4 (6.3%) 0 (0.0%) 2 (3.4%) 1 (1.6%) 6 (9.7%) 1 (1.6%) 0.061 Indications for EGD 0.363 Screening, n (%) 13 (21.0%) 14 (22.6%) 12 (18.8%) 19 (31.7%) 15 (25.4%) 18 (28.1%) 24 (38.7%) 13 (20.6%) Dyspepsia, n (%) 32 (51.6%) 31 (50.0%) 36 (56.2%) 24 (40.0%) 34 (57.6%) 26 (40.6%) 20 (32.3%) 35 (55.6%) Regurgitation, n (%) 14 (22.6%) 13 (21.0%) 9 (14.1%) 13 (21.7%) 8 (13.6%) 9 (14.1%) 12 (19.3%) 12 (19.0%) Other, n (%) 3 (4.8%) 4 (6.4%) 7 (10.9%) 4 (6.6%) 2 (3.4%) 11 (17.2%) 6 (9.7%) 3 (4.8%)BMI, body mass index; EGD, esophagogastroduodenoscopy; IQR, interquartile range; NS, normal saline; P, pronase; PC, postural change; S, simethicone.
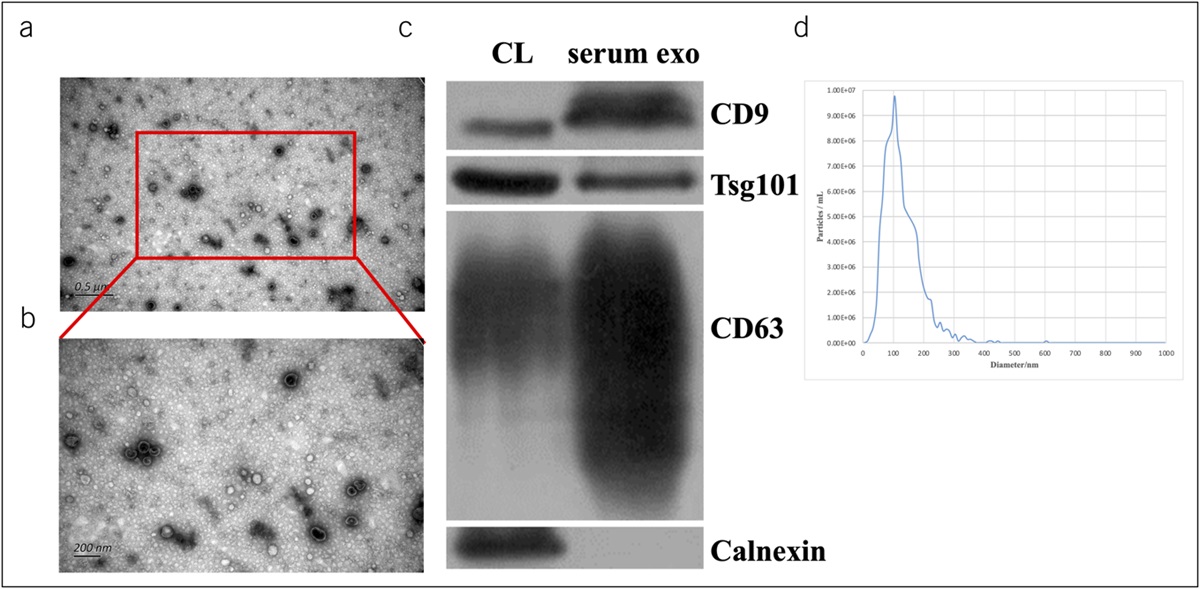
To determine the efficacy of each premedication, we compared the distribution of visibility scores between 2 groups (Table 2). The TVS was significantly better in the S and P groups than in the NS group (12.36 ± 2.93 in the S group vs 14.52 ± 2.57 in the NS group, P = 0.006; 11.86 ± 3.36 in the P group vs 14.52 ± 2.57 in the NS group, P < 0.001). The TVS was better in the P group than in the S group (11.86 ± 3.36 vs 12.36 ± 2.93, P = 0.037). Compared with group P, group S had better MVS for the esophagus and duodenum (1.72 ± 0.60 in the esophagus of group S vs 2.00 ± 0.64 in the esophagus of group P, P = 0.014; 1.31 ± 0.59 in the duodenum of group S vs1.58 ± 0.68 in the duodenum of group P, P = 0.022) but had worse MVS for the upper and lower gastric body (2.89 ± 0.86 in the upper gastric body of group S vs 2.37 ± 0.95 in the upper gastric body of group P, P = 0.002; 2.16 ± 0.96 in the lower gastric body of group S vs 1.85 ± 0.94 in the lower gastric body of group P, P = 0.049). The TVS was significantly better in the P + S group than in the S and P groups (9.81 ± 2.90 in the P + S group vs 12.36 ± 2.93 in group S and 11.86 ± 3.36 in group P, respectively, P < 0.001). The MVS was significantly better in the gastric antrum, fundus, and upper and lower gastric body in the P + S group than in the S group (1.48 ± 0.78 in the gastric antrum of group P + S vs 1.94 ± 0.87 in the gastric antrum of group S, P = 0.006; 1.82 ± 0.90 in the gastric fundus of group P + S vs 2.34 ± 0.86 in the gastric fundus of group S, P = 0.001; 2.06 ± 0.85 in the upper gastric body of group P + S vs 2.89 ± 0.86 in the upper gastric body of group S, P < 0.001; 1.71 ± 0.80 in the lower gastric body of group P + S vs 2.16 ± 0.96 in the lower gastric body of group S, P = 0.004). The MVS was also better in the esophagus, gastric fundus, upper gastric body, gastric antrum, and duodenum in the P + S group than in the P group (1.58 ± 0.64 in the esophagus of group P + S vs 2.00 ± 0.64 in the esophagus of group P, P < 0.001; 1.82 ± 0.90 in gastric fundus of group P + S vs 2.20 ± 0.87 in gastric fundus of group P, P = 0.016; 2.06 ± 0.85 in the upper gastric body of group P + S vs 2.37 ± 0.95 in the upper gastric body of group P, P = 0.045; 1.48 ± 0.78 in gastric antrum of group P + S vs 1.86 ± 0.97 in gastric antrum of group P, P = 0.023; 1.15 ± 0.40 in the duodenum of group P + S vs 1.58 ± 0.68 in the duodenum of group P, P = 0.010). Mucosal visibility scores at different parts of each group were shown in Figure 3.
Table 2. - Visibility scores at different sites in the 4 study groups Sites A (NS) B (S) C (P) D (P + S) P Value A vs B A vs C A vs D B vs C B vs D C vs D Esophagus 2.13 ± 0.67 1.72 ± 0.60 2.00 ± 0.64 1.58 ± 0.64 <0.001 0.281 <0.001 0.014 0.226 <0.001 Gastric fundus 3.00 ± 0.83 2.34 ± 0.86 2.20 ± 0.87 1.82 ± 0.90 <0.001 <0.001 <0.001 0.369 0.001 0.016 Upper gastric body 2.94 ± 0.67 2.89 ± 0.86 2.37 ± 0.95 2.06 ± 0.85 0.748 <0.001 <0.001 0.002 <0.001 0.045 Lower gastric body 2.29 ± 0.76 2.16 ± 0.96 1.85 ± 0.94 1.71 ± 0.80 0.387 0.005 <0.001 0.049 0.004 0.384 Gastric antrum 2.35 ± 1.03 1.94 ± 0.87 1.86 ± 0.97 1.48 ± 0.78 0.015 0.008 <0.001 0.661 0.006 0.023 Duodenum 1.81 ± 0.74 1.31 ± 0.59 1.58 ± 0.68 1.15 ± 0.40 <0.001 0.077 <0.001 0.022 0.127 0.010 TVS 14.52 ± 2.57 12.36 ± 2.93 11.86 ± 3.36 9.81 ± 2.90 0.006 <0.001 <0.001 0.037 <0.001 <0.001NS, normal saline; P, pronase; S, simethicone; TVS, total mucosal visibility score.
Values are given as mean ± SD.
 Figure 3.:
Figure 3.: Mucosal visibility scores at different parts of each group. NS, normal saline; P, pronase; P + S, pronase plus simethicone; S, simethicone.
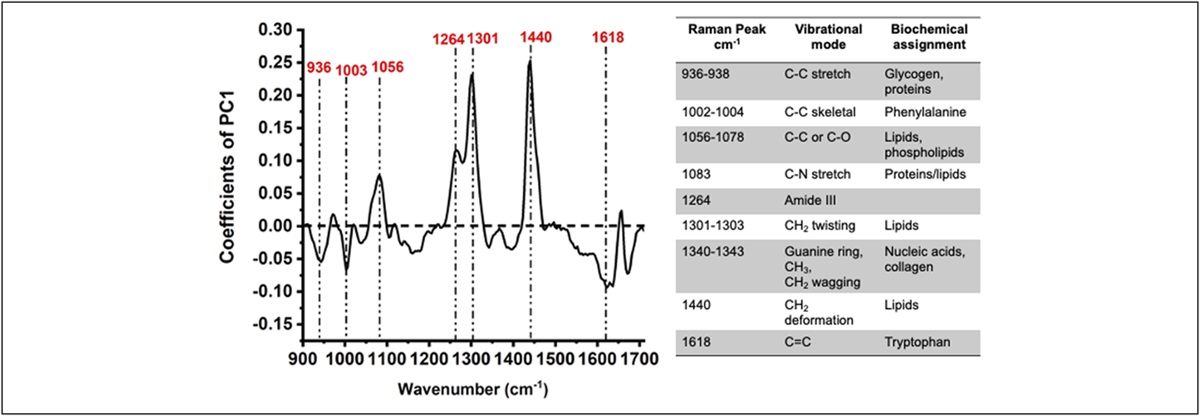
The comparison of the TVS and MVS between the PC and non-PC groups is shown in Table 3. There were no significant differences in the TVS or each separate score for the 6 sites of the upper gastrointestinal tract between the S + PC and S groups (P > 0.05). The MVS was significantly better in the upper gastric body in the P + PC group than in the P group (1.94 ± 0.81 vs 2.37 ± 0.95, P = 0.007), but there were no differences in the remaining 5 sites of the upper gastrointestinal tract between these 2 groups (P > 0.05). The TVS was significantly better in the P + S + PC group than in the P + S group (8.44 ± 2.10 vs 9.81 ± 2.90, P = 0.003). The MVS was significantly better in the gastric antrum, fundus, and upper and lower gastric body in the P + S + PC group than in the P + S group (1.21 ± 0.45 in the gastric antrum of group P + S + PC vs 1.48 ± 0.78 in the gastric antrum of group P + S, P = 0.016; 1.52 ± 0.67 in the gastric fundus of group P + S + PC vs 1.82 ± 0.90 in the gastric fundus of group P + S, P = 0.037; 1.65 ± 0.65 in the upper gastric body of group P + S + PC vs 2.06 ± 0.85 in the upper gastric body of group P + S, P = 0.003; 1.35 ± 0.60 in the lower gastric body of group P + S + PC vs 1.71 ± 0.80 in the lower gastric body of group P + S, P = 0.005), but it was not different in the esophagus or duodenum between these 2 groups (P > 0.05). The MVS of the stomach in the P + S + PC group and the P + S group were shown in Figure 4.
Table 3. - Visibility scores at different sites in the 6 study groups Sites A (S) B (S + PC) C (P) D (P + PC) E (P + S) F (P + S + PC) P Value A vs B C Vs D E vs F Esophagus 1.72 ± 0.60 1.80 ± 0.58 2.00 ± 0.64 1.83 ± 0.46 1.58 ± 0.64 1.54 ± 0.62 0.445 0.088 0.717 Gastric fundus 2.34 ± 0.86 2.32 ± 0.70 2.20 ± 0.87 2.08 ± 0.82 1.82 ± 0.90 1.52 ± 0.67 0.848 0.412 0.037 Upper gastric body 2.89 ± 0.86 2.60 ± 0.79 2.37 ± 0.95 1.94 ± 0.81 2.06 ± 0.85 1.65 ± 0.65 0.054 0.007 0.003 Lower gastric body 2.16 ± 0.96 2.10 ± 0.75 1.85 ± 0.94 1.72 ± 0.75 1.71 ± 0.80 1.35 ± 0.60 0.719 0.401 0.005 Gastric antrum 1.94 ± 0.87 1.90 ± 0.80 1.86 ± 0.97 1.69 ± 0.92 1.48 ± 0.78 1.21 ± 0.45 0.803 0.303 0.016 Duodenum 1.31 ± 0.59 1.22 ± 0.45 1.58 ± 0.68 1.47 ± 0.69 1.15 ± 0.40 1.17 ± 0.42 0.314 0.384 0.689 TVS 12.36 ± 2.93 11.93 ± 2.46 11.86 ± 3.36 10.72 ± 3.05 9.81 ± 2.90 8.44 ± 2.10 0.383 0.051 0.003NS, normal saline; P, pronase; PC, postural change; S, simethicone; TVS, total mucosal visibility score.
Values are given as mean ± SD.
 Figure 4.:
Figure 4.: The mucosal visibility scores of the stomach in the P + S + PC group and the P + S group. P + S: pronase plus simethicone, P + S + PC: Pronase plus simethicone combine postural change.
Procedure time, water flushes necessary to improve visibility, diminutive lesions, and a biopsy during EGD examinationsThe procedure time (7.4 ± 2.6 minutes, 7.9 ± 2.9 minutes, 7.8 ± 2.9 minutes, 7.7 ± 2.8 minutes, 7.4 ± 2.4 minutes, 7.1 ± 2.6 minutes, 7.8 ± 3.2 minutes, and 7.1 ± 2.1 minutes, P = 0.261), the biopsy rate (30 [48.4%], 34 [54.8%], 38 [59.4%], 36 [60.0%], 36 [61.0%], 43 [67.2%], 38 [61.3%], and 39 [61.9%], P = 0.589), and the detection rate of diminutive lesions, including early cancer of the esophagus and stomach (37 [59.7%], 48 [77.4%], 48 [75.0%], 40 [66.7%], 45 [76.3%], 39 [60.9%], 41 [66.1%], and 48 [76.2%], P = 0.173) (NS, NS + PC, S, S + PC, P, P + PC, P + S, and P + S + PC groups, respectively) were not significantly different among the 8 groups.
The amount of water flushed for satisfactory observation of the upper gastrointestinal tract was 55 (IQR: 18–110) mL in the NS group, 50 (IQR: 20–98) mL in the S group, and 40 (IQR: 0–70) mL in the P group. Fewer flushes were used during the procedures performed in the P + S group (0 [IQR: 0–33] mL) than in the other 3 groups (P + S vs NS, P < 0.001; P + S vs S, P < 0.001; P + S vs P, P < 0.01). The amount of water flushed for satisfactory observation of the upper gastrointestinal tract was also compared between each pair of groups (S + PC vs S, P + PC vs P, and P + S + PC vs P + S) to further examine the effect of postural change on it. However, there were no significant differences between these groups (Table 4).
Table 4. - Procedure time, mucosal cleaning water consumption, diminutive lesions, and biopsy for all study groups Variables NS NS + PC S S + PC P P + PC P + S P + S + PC P Value Patients (n) 62 62 64 60 59 64 62 63 Procedure time (min), mean ± SD 7.4 ± 2.6 7.9 ± 2.9 7.8 ± 2.9 7.7 ± 2.8 7.4 ± 2.4 7.1 ± 2.6 7.8 ± 3.2 7.1 ± 2.1 0.261 Water required for mucosal cleansing (mL), median (IQR) 55 (18, 110) 60 (30, 110) 50 (20, 98) 40 (0, 88) 40 (0, 70) 30 (0, 50) 0 (0, 33) 0 (0, 20) <0.001 Diminutive lesions, n (%) 37 (59.7%) 48 (77.4%) 48 (75.0%) 40 (66.7%) 45 (76.3%) 39 (60.9%) 41 (66.1%) 48 (76.2%) 0.173 Biopsy, n (%) 30 (48.4%) 34 (54.8%) 38 (59.4%) 36 (60.0%) 36 (61.0%) 43 (67.2%) 38 (61.3%) 39 (61.9%) 0.589IOR, interquartile range; NS, normal saline; P, pronase; PC, postural change; S, simethicone.
To date, there is no international agreement on premedication use for upper gastrointestinal endoscopy examinations. Our study showed that simethicone had a better effect than pronase on the esophagus and duodenum where there is little mucus attachment but more foam. In the stomach with a large amount of mucus secretion, especially the stomach body, the effect of pronase with mucolytic function was significantly better than that of simethicone. These results may be because the surface of the esophageal and duodenal mucosa is covered with relatively more foam and bubbles, but less mucus, whereas there is usually a lot of mucus in addition to foam in the stomach. Therefore, the effect of simethicone on the removal of mucus and that of simethicone on the removal of foam are different. Furthermore, the combination of preprocedural administration with simethicone and pronase achieved superior mucosal visualization compared with saline, simethicone, or pronase alone in patients receiving upper endoscopy, suggesting that a combination of simethicone and pronase should be recommend as routine use of premedication during EGD.
However, how to ensure best practice in the use of simethicone or pronase is poorly understood. To date, the evidence on whether a postural change is required after the use of simethicone or pronase before endoscopy is rare. Few studies have mentioned the scheme of postural change. Wang et al reported that a postural change was implemented by turning over 360 degrees (either to the left or the right), with a time ranging from 1 to 15 minutes. Too long a time for a postural change leads to poor compliance of patients, whereas too short a time may affect the uniform distribution of the drug across all parts of the upper digestive tract (16). Therefore, the protocol performed in this study involved maintaining movement in the horizontal position (around the axis of the body) for 5 minutes. We found that a postural change did not improve visualization of the mucosa with the administration of simethicone alone, but it improved visualization of the proximal gastric body with the administration of pronase alone. In addition, premedication with both pronase and simethicone combined with a postural change further improved the mucosal visibility of most parts of the stomach. These findings suggest that a postural change can optimize the efficacy of visualizing the gastric mucosa when applying premedication with pronase and simethicone.
Completing body rotation of the patient may be restricted by the different conditions of the individual endoscopic center, and it also depends on the patient's compliance to a certain extent. In this study, we set up 4 beds in a separate room, instructed the patients to lie on the bed, and completed body rotation after premedication was taken orally. Although this process may slightly increase the workload for the staff, we should still persuade patients to complete the maneuver to obtain clear images on the basis of the abovementioned findings.
A further interesting observation in this study is that, in the P + S + PC group, there was a significantly better MVS in the gastric antrum, gastric fundus, and the proximal and distal parts of the gastric body than in the P + S group. However, there was no significant difference in the MVS in the esophagus and duodenum between the 2 groups. A possible reason for this lack of difference in the MVS is that a postural change causes simethicone and pronase to be evenly distributed in all parts of the gastric cavity. This distribution increases the contact between the drug and foam and mucus on the surface of the gastric mucosa to obtain a clean endoscopic field of view. However, the lumen of the esophagus and duodenum is small, which results in a short time for the presence of medication, leading to little effect of postural change. These observations suggest that in lesions located in the stomach, rather than in the esophagus or duodenum, a postural change should be performed combined with premedication.
The ability to detect diminutive lesions, which are defined as lesions ≤ 5 mm, is vital for the diagnosis of early gastric cancer. A multicenter, randomized, controlled study conducted by Liu et al (17) showed that, although premedication with pronase and simethicone significantly increased the visibility of the upper gastrointestinal mucosa, it did not increase the detection rate of small lesions. This study showed a similar finding that there was no significant difference in the detection rate of small lesions or the biopsy rate among the different groups during an endoscopic examination. Even in the P + S group, which had a reduced number of water flushes, the endoscopic procedure time was not less than that in the NS, S, and P groups. However, the risk of aspiration due to excessive fluid accumulation in the upper digestive tract may be reduced in the P + S group. One probable explanation for this lack of finding is that the incidence of gastric cancer was relatively low in the population in this study. Furthermore, with better visibility of the gastric mucosa, more subtle details of mucosal changes can be detected, which may lead to longer time of observation and an accurate diagnosis. People at a high risk of gastric cancer (i.e., patients with premalignant conditions or with history of Helicobacter pylori infection) could be included to improve the detection of early gastric cancer in future studies.
There are several limitations to this study. First, the main results were TVS and MVS, which were scored by different reviewers; there may have been interobserver variation in judgment of the MVS score by different reviewers. However, all of the endoscopists and supervisors were provided with standardized instructions for the standard operation. Therefore, the possibility of bias was relatively small.
Second, this was a single-center study, and the sample size was limited. All patients were from the outpatient clinic, and most of them visited for a routine endoscopic examination, resulting in a relatively narrow disease spectrum, which may have affected the results. For example, there was no difference in the detection rate of diminutive lesions in this study, which may be related to the fact that the patients were non–high-risk groups of gastric cancer and the sample size was relatively small. Increased reliability of the data could be achieved by conducting multicenter studies and involving more populations in the future.
Finally, this study only compared premedication with simethicone and pronase, and some other agents, such as dyclonine hydrochloride and N-acetylcysteine, have not been evaluated. Dyclonine hydrochloride contains a local anesthetic component and antifoaming agent component, whereas N-acetylcysteine, which is an antimucous medicine, has also been used in clinical practice (18–21). Studies need to be performed to compare the effects of more agents in premedication use and to examine potential factors that affect a postural change.
In conclusion, our results found that the use of simethicone or pronase alone before EGD improved mucosal visibility during the procedure and that the combination of the 2 agents was superior to the use of the 2 agents alone. At the same time, the effect was better after added postural change on the basis of the combination of the 2 agents. However, in the past decades, scholars have mainly focused on the effects of premedication with different agents on mucosal clarity but have paid little attention to the role of a postural change in this situation. To the best of our knowledge, this study is the first to investigate the effect of a postural change combined with premedication on mucosal visibility during an EGD examination. Our results provide the latest clinical trial evidence for optimizing the use of pronase and simethicone before EGD and could improve the effectiveness and accuracy of gastroscopic screening. Moreover, a postural change is generally simple and feasible to obtain and does not increase any financial burden to patients. Therefore, we suggest that preoperative medication combined with a postural change as a conventional method should be recommended for wide clinical application to obtain better mucosal visibility and further improve the effectiveness of endoscopic procedures.
CONFLICTS OF INTERESTGuarantor of the article: Mei Liu, PhD.
Specific author contributions: M.L. and L.C.: study concept and design. L.C., F.Z., X.F., Z.Z., J.L., and M.W.: acquisition of data. L.C.: drafting of the manuscript. M.L.: revision of the manuscript. L.C., Q.G., and M.L.: study supervision.
Financial support: None to report.
Potential competing interests: None to report.
Study Highlights
WHAT IS KNOWN ✓ Prescribing premedication to eliminate the mucus and foam is necessary to achieve better visualization during upper endoscopy. ✓ Pronase and simethicone are commonly used premedications for conventional endoscopy. WHAT IS NEW HERE ✓ The combination of preprocedural administration with simethicone and pronase achieved superior mucosal visualization compared with saline, simethicone, or pronase alone in patients receiving upper endoscopy. ✓ Postural change maneuvers performed beforeendoscopy further improved the mucosal visibility in most parts of the stomach when used with preprocedural simethicone and pronase. ACKNOWLEDGEMENTThe authors thank the staff of the digestive endoscopic center at Tongji hospital.
REFERENCES 1. Machlowska J, Baj J, Sitarz M, et al. Gastric cancer: Epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int J Mol Sci 2020;21(11):4012. 2. Wang FH, Shen L, Li J, et al. The Chinese Society of Clinical Oncology (CSCO): Clinical guidelines for the diagnosis and treatment of gastric cancer. Cancer Commun 2019;39(1):10. 3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–32. 4. Yeoh KG. How do we improve outcomes for gastric cancer? J Gastroenterol Hepatol 2007;22(7):970–2. 5. Pimenta-Melo AR, Monteiro-Soares M, Libanio D, et al. Missing rate for gastric cancer during upper gastrointestinal endoscopy: A systematic review and meta-analysis. Eur J Gastroenterol Hepatol 2016;28:1041–9. 6. Menon S, Trudgill N. How commonly is upper gastrointestinal cancer missed at endoscopy? A meta-analysis. Endosc Int Open 2014;02(02):E46–50.
留言 (0)