
Remember me





Gastric cancer is the fourth most common cancer globally, with the number of people suffering from it rising each year, and the second leading cause of cancer death worldwide. To date, surgical resection is one of the most effective treatments of resectable cancers, and research on the prognosis of patients after surgery is ongoing (1,2). Although many researchers have tried to use some new biomarkers to predict the postoperative outcome of patients with gastric cancer in recent years, the clinical prediction of patients' postoperative outcomes is still inadequate (3,4). Therefore, there is an urgent need to discover new and more representative markers and predictive models to improve postoperative survival or recurrence prediction.
Circulating tumor cells (CTCs) are tumor cells disseminated in the peripheral blood of patients with tumors. The current technology for monitoring CTCs is mature, and the presence of CTCs has been detected in different cancer types. The presence of CTCs symbolizes a poor prognosis for patients (5,6). A meta-analysis by Rahbari et al (7) concluded that CTC plays an essential role in predicting the prognosis of patients with colorectal cancer. Currently, CTC is essential to predict the prognosis of patients with gastric cancer after surgery. No investigator has used CTCs to build predictive models to predict overall and recurrence-free survival (RFS) after surgery for resectable gastric cancer. This study aims to establish a nomogram based on CTC—a marker of importance—and validate it with a validation group and finally use the nomogram to establish a risk scoring system to stratify the management of patients with resectable gastric cancer.
METHODS Patient selectionData were collected from one center from 258 patients with resectable gastric cancer who underwent surgery between January 2012 and June 2017 and were called the training group. Data from 133 patients with resectable gastric cancer who underwent surgical treatment were collected from another center. We used strict inclusion criteria, and the inclusion criteria were as follows: (i) postoperative tumor histopathology determined to be gastric cancer by 2 experienced pathologists; (ii) patients' TNM stage was strictly determined according to the eighth edition of the American Joint Committee on Cancer, mainly by postoperative pathology; (iii) American Society of Anesthesiologists (ASA) score ≤II; (iv) Eastern Oncology Collaborative Group (ECOG) physical status score ≤2; (v) normal liver and kidney function; (vi) the tumor was found for the first time and had not undergone endoscopic mucosal resection or endoscopic submucosal dissection before surgery; and (vii) postoperative pathology was reported by 2 pathologists to be negative for cut margins. Patients at both centers underwent a uniform standardized treatment protocol. In principle, patients with preoperative lymph node metastases are recommended to undergo chemotherapy. However, the centers fully respect the patient's wishes, and the final decision on whether to undergo preoperative chemotherapy largely depends on the patient's wishes. This retrospective study was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, and the Ethics Committee of Zhongshan People's Hospital and followed the Declaration of Helsinki.
SurgeryThe tumor is assessed for invasion of surrounding organs and vital blood vessels and for distant metastases by a specialist team of gastroenterologists and imaging experts. When the tumor invades the hilar region, pancreas, aorta, and mesenteric root vessels, it is an indication for surgical nonresection (8). Preoperative tests such as red blood cell count and liver and kidney function tests are routinely performed to assess the suitability for surgery. The location of the tumor in the stomach determines the extent of gastrectomy: total gastrectomy for tumors growing in the upper third; total gastrectomy for tumors growing in the body of the stomach or distal gastrectomy, depending on the case; and distal gastrectomy for tumors growing in the distal part of the stomach (sinus). An experienced surgical team performs all surgical procedures.
Detection of CTCsOne week before the gastrectomy, we first took approximately 5 mL of peripheral blood and standardized the removed samples according to the company's instructions. CTC was detected using the Cyttel method (Jiangsu, China), which consists of the negative immunomagnetic particle method and immunofluorescence in situ hybridization. The former mainly uses immunomagnetic particles as a carrier to remove leukocytes from blood and isolate rare cells in vitro by the principle of antigen-antibody reaction combined with the centrifugation technique. The samples are fixed on slides, dehydrated with ethanol, dried, and hybridized with Chromosome Adhesion Probe 1 and Chromosome Adhesion Probe 1. Finally, 4-diamidino-2-phenylindole was added to stain the closed specimens, and CTCs were observed and counted under fluorescence microscopy. Based on previous studies and multicenter discussions, it defined CTC counts ≥1 as CTC-positive (9,10).
Follow-upWe followed up with all patients every 3 months during the first year after discharge, and every 6 months after the first year. Imaging examinations, such as abdominal ultrasound, enhanced computed tomography, and abdominal magnetic resonance imaging, and laboratory tests, such as liver function and kidney function, were performed at each follow-up visit. For patients undergoing surgery, overall survival (OS) was defined as the time from postoperative day 1 to death; RFS was defined as the time from postoperative day 1 to the first imaging finding of tumor or metastasis. The follow-up period was ended October 30, 2021.
Data analysisThe χ2 or Fisher exact test was used to compare all categorical variables. The Kaplan-Meier method was used for the comparison of OS and RFS of diseases. The log-rank test was used for the comparison of survival rate. Univariate and multivariate analyses were performed for OS and RFS after gastrectomy using the Cox proportional model. Variables with P < 0.05 in univariate analysis were included in multivariate regression analysis. Receiver operator characteristic curves were used to assess the model's discrimination, and calibration curves were used to assess the calibration of the model. A risk scoring system was then established based on the total score of each patient in the training cohort (sum of the scores of each variable given by the column line graph), and patients were divided into 3 risk groups—low, medium, and high—with a similar number of cases in them.
All statistical analyses were performed using SPSS 25.0 (IBM, Armonk, NY), and P values <0.05 (both sides) were considered statistically significant. R software (version 4.0.5; R Project for Statistical Computing, Vienna, Austria) was used to generate the Kaplan-Meier curves, receiver operator characteristic curves, and calibration curves. X-tile software (version 3.6.1) determined the cutoff value of the scores in the training cohort. The sample size was calculated using PASS (version 11.0) before conducting the study. We set 2-sided alpha = 0.05 and beta = 0.1 (sample power = 0.9).
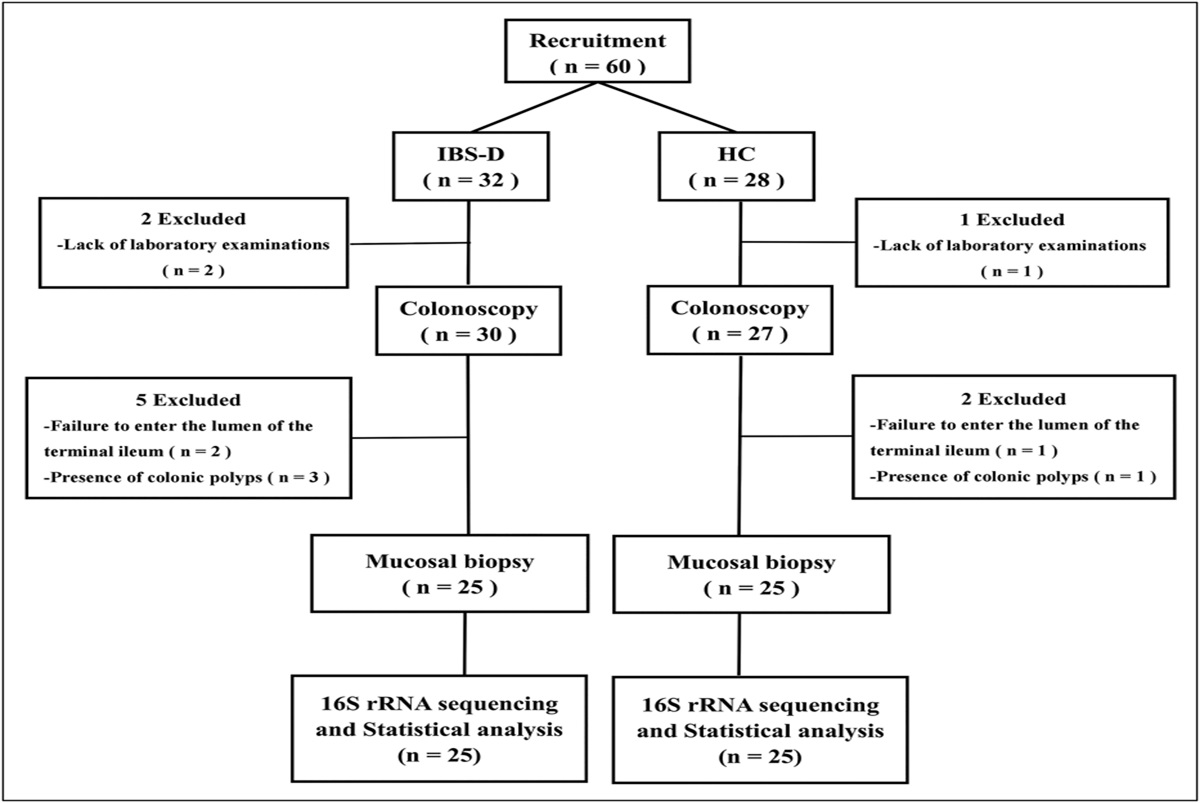
RESULTS Characteristics of the patients with gastric cancer in the training cohort and validation cohortThe inclusion and exclusion flow charts for the training and validation cohorts are shown in Supplementary Figure 1 (see Supplementary Digital Content 1, https://links.lww.com/CTG/A907). There were a total of 258 patients in the training cohort and 133 patients in the validation cohort; in the training cohort, there were 215 male patients (83.3%), 111 (43.0) older than 60 years, and 50 CTC-positive patients (19.4%); in the validation group, there were 111 male patients (83.5%), 65 (65) older than 60 years (48.9%), and 34 patients (25.6%) were CTC-positive. Nearly 20 percent of the patients at both centers received preoperative chemotherapy. None of the variables was statistically different between the 2 groups (Table 1).
Table 1. - Baseline characteristics of patients with gastric cancer undergoing gastrectomy in the training cohort and validation cohort (n = 391) Training cohort (n = 258) Validation cohort (n = 133) P value Sex, n (%) 1.000 Male 215 (83.3) 111 (83.5) Female 43 (16.7) 22 (16.5) Age, n (%) 0.285 <60 yr 147 (57.0) 68 (51.1) ≥60 yr 111 (43.0) 65 (48.9) ASA, n (%) 0.446 I 217 (84.4) 116 (87.9) II 40 (15.6) 16 (12.1) ECOG PS, n (%) 1.000 0 203 (78.7) 105 (78.9) 1 55 (21.3) 28 (21.1) Depth of tumor invasion, n (%) 0.388 T1 48 (18.6) 28 (21.1) T2 23 (9.0) 14 (10.5) T3 123 (47.7) 71 (53.4) T4 64 (24.8) 20 (15.0) N status, n (%) 0.124 N0 62 (24.0) 25 (18.8) N1 70 (27.1) 28 (21.1) N2 57 (22.1) 37 (27.8) N3 69 (26.7) 43 (32.3) TNM stage, n (%) 0.432 I stage 86 (33.3) 50 (37.6) II stage 88 (34.1) 48 (36.1) III stage 84 (32.6) 35 (26.3) Preoperative chemotherapy 0.529 No 196 (76.0) 105 (78.9) Yes 62 (24.0) 28 (21.1) Differentiation 0.436 Well + moderately 52 (20.2) 32 (24.1) Poorly 206 (79.8) 101 (75.9) Operation performed 0.718 Total gastrectomy 77 (29.8) 45 (33.8) Distal gastrectomy 168 (65.1) 82 (61.7) Others 13 (5.1) 6 (4.5) Extent of lymphadenectomy 0.636 D1 51 (19.8) 29 (21.8) D1 + D2/D3 207 (80.2) 104 (78.2) Lymphatic invasion 0.653 No 72 (27.9) 40 (30.0) Yes 186 (72.1) 93 (70.0) Tumor number, n (%) 0.556 Single 248 (96.1) 130 (97.7) Multiple 10 (3.9) 3 (2.3) Tumor size, n (%) 0.054 <5 cm 114 (44.2) 73 (54.9) ≥5 cm 144 (55.8) 60 (45.1) Vascular invasion, n (%) 0.369 No 92 (35.7) 41 (30.8) Yes 166 (64.3) 92 (69.2) Ki-67, n (%) 0.522 <50% 134 (51.9) 74 (55.6) ≥50% 124 (48.1) 59 (44.4) CTC, n (%) 0.193 Negative 208 (80.6) 99 (74.4) Positive 50 (19.4) 34 (25.6)TNM stages are according to the American Joint Committee on Cancer, Eighth Edition.
ASA, American Society of Anesthesiologists; CTC, circulating tumor cell; ECOG, Eastern Cooperative Oncology Group; PS, performance status.
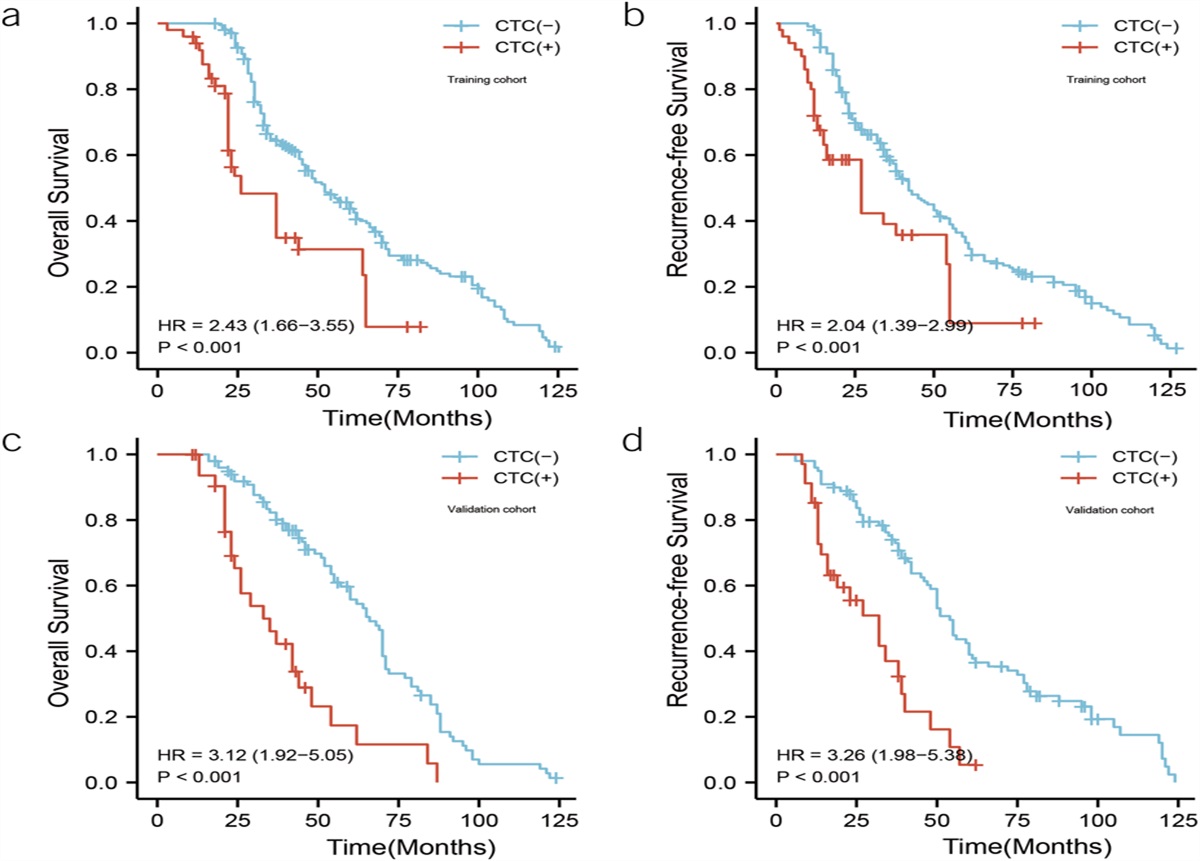
In the training group, the prognosis of CTC(+) patients was worse than that of CTC(−) patients. The 1-, 3-, and 5-year OS of CTC(+) patients was 94.1%, 47.2%, and 23.0%, respectively, with a median survival time of 26.0 months; the 1-, 3-, and 5-year OS of CTC(−) patients was 100.0%, 64.7%, and 44.0%, respectively, with a median survival was 52.0 months, with statistically significant differences in OS curves between the 2 groups (hazard ratio [HR] = 1.43 [1.66–3.55], P < 0.001). The 1-, 3-, and 5-year RFS for CTC(+) patients was 70.6%, 38.3%, and 8.8%, respectively, with a median time to relapse of 27.0 months; CTC(−) patients had RFS of 98.6%, 58.8%, and 33.5% at 1, 3, and 5 years, respectively, with a median time to recurrence of 42.0 months, with statistically significant differences in RFS curves between the 2 groups (HR = 2.04 [1.39–2.99], P < 0.001). In the validation group, CTC(+) patients were also worse than CTC(−) patients in overall survival and RFS (Figure 1).
 Figure 1.:
Figure 1.: Impact of positive or negative circulating tumor cells (CTCs) on overall survival and recurrence-free survival of patients after surgery. (a) Overall survival of CTC(+) vs CTC(−) in the training cohort. (b) Recurrence-free survival of CTC(+) vs CTC(−) in the training cohort. (c) Overall survival of CTC(+) vs CTC(−) in the validation cohort. (d) Recurrence-free survival of CTC(+) vs CTC(−) in the validation cohort.
Univariate and multivariate Cox regressions as prognostic factors in patients with gastric cancerIn the training cohort, we included the statistically significant screening obtained from the univariate Cox regression analysis into the multifactorial regression analysis based on P < 0.05. TNM stage (HR = 1.678 [1.238–1.881]), Ki-67 (HR = 2.150 [1.512–2.876]), differentiation (HR = 1.645 [1.234–2.121]), extent of lymphadenectomy (HR = 0.568 [0.389–0.912]), lymphatic invasion (HR = 1.674 [1.112–2.431]), and CTC (HR = 2.345 [1.756–3.567]) were considered as prognostic factors affecting patients' OS (Table 2); TNM stage (HR = 1.432 [1.198–1.744]), Ki-67 (HR = 1.879 [1.438–2.510]), differentiation (HR = 1.687 [1.152–2.342]), extent of lymphadenectomy (HR = 0.668 [0.588–0.973]), lymphatic invasion (HR = 1.777 [1.287–2.347]), and CTC (HR = 2.213 [1.675–2.887]) were also considered as prognostic factors affecting patients' RFS (Table 3), and a nomogram was created based on these 3 variables obtained from the training cohort (Figure 2a and b)
Table 2. - Univariate and multivariate analyses of overall survival in patients with gastric cancer who underwent gastrectomy in the training cohort Univariate analysis Multivariate analysis P value HR 95% confidence interval P value HR 95% confidence interval SexTNM stages are according to the American Joint Committee on Cancer, Eighth Edition.
ASA, American Society of Anesthesiologists; CTC, circulating tumor cell; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; PS, performance status.
TNM stages are according to the American Joint Committee on Cancer, Eighth Edition.
ASA, American Society of Anesthesiologists; CTC, circulating tumor cell; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; PS, performance status.
 Figure 2.:
Figure 2.: Column plots of predicted overall survival (OS) and recurrence-free survival (RFS) based on the results of multivariate Cox regression analysis and plotting of time-dependent receiver-operating characteristic (ROC) curve. (a) and (b) Nomograms of predicted OS and RFS, respectively. (c) and (d) 1-, 3-, and 5-year ROC curves in the training cohort and their area under the curve (AUC), respectively. (e) and (f) 1-, 3-, and 5-year ROC curves in the validation cohort and their AUC, respectively.
Test the discrimination and calibration of the nomogramIn the training cohort, a time-dependent receiver-operating characteristic (ROC) curve showed that the patients' areas under the curve (AUCs) for 1-, 3-, and 5-year OS were all more than 0.80, at 0.916, 0.829, and 0.813, respectively. Similarly, the time-dependent ROC showed that the patients' AUCs for 1-, 3-, and 5-year RFS were 0.900, 0.884, and 0.839, respectively. AUC of 0.900, 0.884, and 0.839, respectively; using the validation group, essentially all 1-, 3-, and 5-year AUCs for OS and RFS were more than 0.800.
The calibration curves were plotted to evaluate the 2 newly created models. In the training cohort, the actual 3- and 5-year OS and RFS are in good agreement with the 3- and 5-year OS and RFS predicted by the nomogram (Figure 3a–d). In the validation cohort, the actual 3- and 5-year OS and RFS are also in good agreement with the 3- and 5-year OS and RFS predicted by the nomogram (Figure 3e–h).
 Figure 3.:
Figure 3.: Calibration curves of the predicted nomogram for overall survival (OS) and recurrence-free survival (RFS). (a) and (b) 1-, 3-, and 5-year calibration of the nomogram for OS in the training cohort. (c) and (d) 1-, 3-, and 5-year calibration of the nomogram for RFS in the training cohort. (e) and (f) 1-, 3-, and 5-year calibration of the nomogram for OS in the validation cohort. (g) and (h) 1-, 3-, and 5-year calibration of the nomogram for RFS in the validation cohort.
Generate a risk scoring system based on the nomogramIn the training cohort, we used X-tile software to determine the cutoff values based on the total score given to each patient in the nomogram and classified the patients into low, medium, and high groups. In the low-risk group, the patients' 1-, 3-, and 5-year OS was 100.0%, 94.6%, and 73.4%, respectively; the median survival time was 82.0 months. In the medium-risk group, the patients' 1-, 3-, and 5-year OS was 100.0%, 64.0%, and 38.3%, respectively, with a median survival time of 48.0 months; in the high-risk group, patients had an OS of 96.9%, 28.7%, and 11.5%, respectively, for 1, 3, and 5 years, with a median survival time of 29.0 months, with a significant prognostic difference between the 3 groups (P < 0.01). The validation group also had a significant prognostic difference between the low, medium, and high-risk groups (Figure 4).
 Figure 4.:
Figure 4.: Overall survival in the training and validation sets for the low, medium, and high-risk groups.
DISCUSSIONSurgical resection is the first-line treatment of gastric cancer, especially resectable gastric cancer, which is often curable. However, the 5-year survival rate after surgery is still poor, and disease progression such as recurrence can occur. Some researchers (11–13) have used tumor markers such as CEA and CA19-9 to predict patients after surgery, but these markers are limited and often negative. In the meantime, some investigators have developed models to predict the prognosis of patients with gastric cancer after surgery, but they are often unsatisfactory, with relatively low predictive efficacy (14,15). Therefore, there is a need for effective biomarkers to predict postoperative survival and the risk of recurrence and predictive models and stratification of postoperative patients for more refined management.
CTCs are a type of tumor cell present in the circulating blood system (16). Recently, an increasing number of articles have demonstrated the prognostic role of CTCs in predicting patients with different types of cancers (17–19). Our study assessed the prognostic role of CTCs in patients with resectable gastric cancer after surgery and showed that positive CTCs were associated with a poorer prognosis in both OS and RFS, and the same results were found in the validation group. Meanwhile, multivariate Cox regression analysis also indicated that CTC was a significant prognostic factor affecting OS and RFS. Nowadays, studies on the prognostic role of CTC in gastrointestinal tract tumors are actively being conducted. Zhang et al (20) compared the changes in CTC values in preoperative and postoperative patients with gastric cancer and concluded that increased postoperative CTC might increase hematogenous recurrence; Ito et al (21) concluded that recurrence is closely related to the number of patients with CTC , and a meta-analysis by Gao et al (22) similarly suggested that CTC could identify patients with worse prognosis of gastric cancer and showed more robust and more stable predictive value in advanced disease. Thus, considerable evidence also suggests that CTC is important in predicting patient prognosis, and we are the first study to use CTC to predict postoperative prognosis in patients with resectable gastric cancer and develop a prognostic model based on CTC.
All patients with early gastric cancer (Tis or T1aN0M0) included in our cohort were treated surgically. However, the current treatment modalities for early gastric cancer are mainly surgical and endoscopic, which are somewhat controversial. Pourmousavi et al (23) analyzed a sizeable population-based database from 1998 to 2014 and found an increasing trend in endoscopic treatment of superficial gastric cancer compared with surgery. Patients who underwent endoscopic treatment vs surgery had comparable long-term cancer-specific mortality. Similarly, a meta-analysis by Sun et al (24) identified 9 retrospective studies that showed endoscopic resection might be a feasible and safe treatment strategy compared with gastrectomy. At present, careful endoscopic testing is needed to ensure good results and validation in large-scale randomized controlled studies from different countries. However, the trend toward endoscopic treatment of early gastric cancer is slowly expanding.
We established a nomogram for predicting OS and RFS after resectable gastric cancer. Previously, Yu and Zhang (25) constructed a nomogram to predict the prognosis of gastric cancer in young patients with a C-index of 0.688, which is lower than the C-index of our nomogram. Additionally, other researchers have constructed nomograms to predict gastric cancer survival by combining multiple genes (15,26), and Zhu et al (27) predicted early death in metastatic gastric cancer by Surveillance, Epidemiology, and End Results. However, these studies suffer from insufficient sample size and sample size from public databases. Our nomograms were composed of TNM stage, Ki-67, and CTC and were validated by the validation group. TNM staging is a vital staging system with different prognostic survival assessments for patients with different stages of gastric cancer. However, TNM has certain limitations. For example, the treatment at different stages is not agreed upon, and combining it with CTC can provide the opportunity to go beyond the individualized risk assessment determined by TNM staging only (28). There is also some inter-relationship with the TNM stage, with stage III and IV tumors exhibiting greater ease of detection of CTCs. Notably, Ki-67 also has a solid predictive role, and in our multivariate Cox regression analysis, the variable Ki-67 was highly weighted in the model. Ki-67 has also received attention from researchers in recent years because it has long been recognized as a value-added marker for tumors and also has strong potential as a diagnostic marker for gastrointestinal tract tumors, as suggested by Yang et al (29). The Ki-67 index was negatively correlated with tumor differentiation, and the CTC index was not correlated with the Ki-67 index. The 2 markers were independent of each other. Ki-67 also has a vital role in predicting the prognosis of patients with cancer, and a meta-analysis by Jung-Soo Pyo (30) showed that a high Ki-67 index was associated with a poorer prognosis of pati
Comments (0)