Traditional WHO classifications for tumors of endocrine organs and the digestive system conventionally defined MiNEN in which each component comprises at least 30% of the lesion [9, 10]. However, the threshold was set arbitrarily without concrete evidential support [2]. In certain organs, such as the esophagus, stomach, and colorectum, the WHO classification has not established a specific minimum percentage for defining MiNEN [10]. The current case has been diagnosed as MiNEN according to traditional WHO classifications. This diagnosis is supported by the fact that both NEN and non-NEN components each constitute more than 30% of the lesion. Three theories have been proposed to explain the origins of MiNENs, as the pathogenesis remains a subject of debate. The first theory suggests that NEN and non-NEN components develop from distinct cells and eventually merge. The second theory postulates that both components originate from a common pluripotent stem cell progenitor, which undergoes differential differentiation during carcinogenesis. The third theory assumes a shared monoclonal origin for both counterparts, but the NEN counterpart evolves from the non-NEN cells, driven by the progressive accumulation of genetic abnormalities [11]. The findings from our case suggested the third theory, as a part of conventional SCC was considered to obtain undifferentiated morphology and neuroendocrine properties.
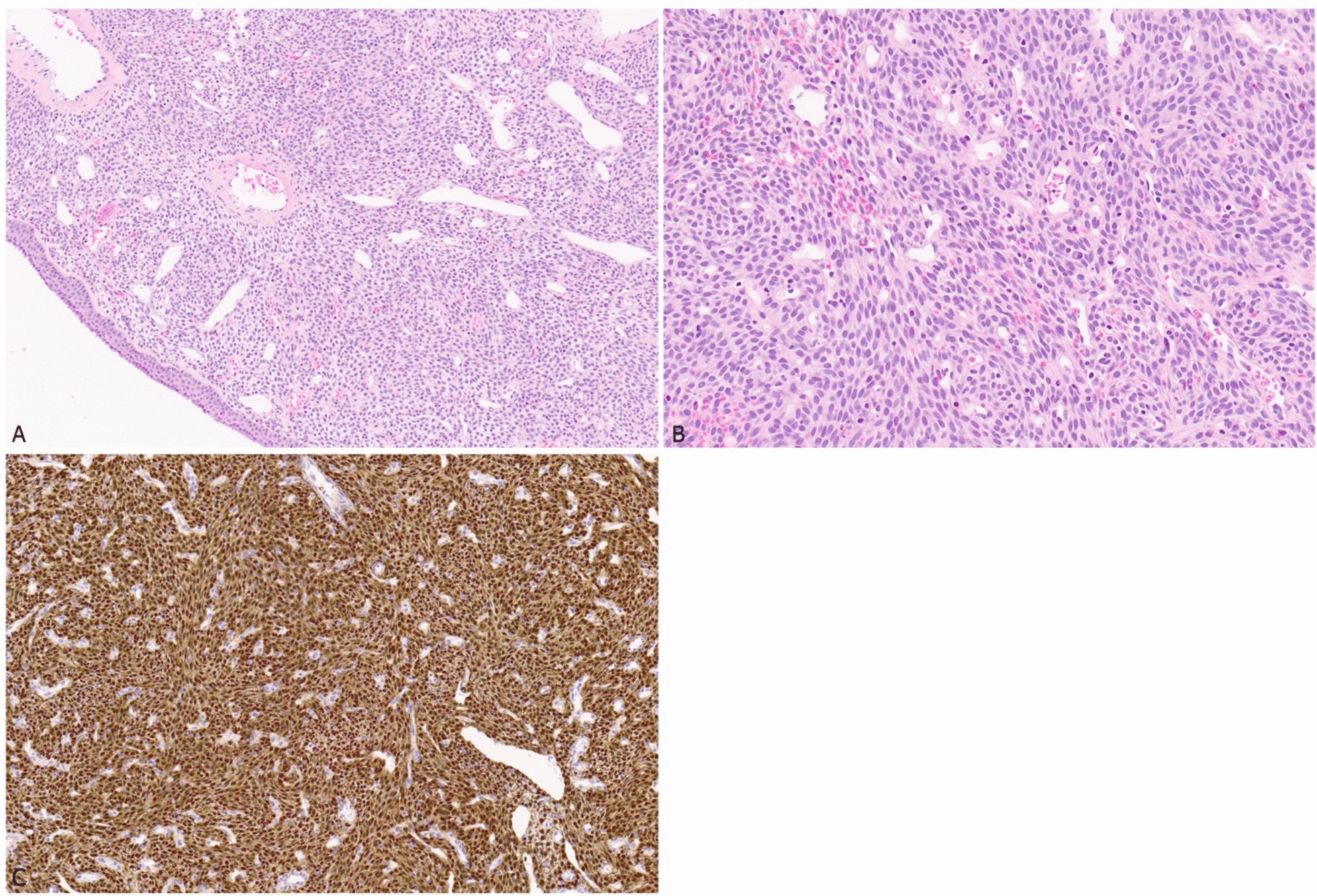
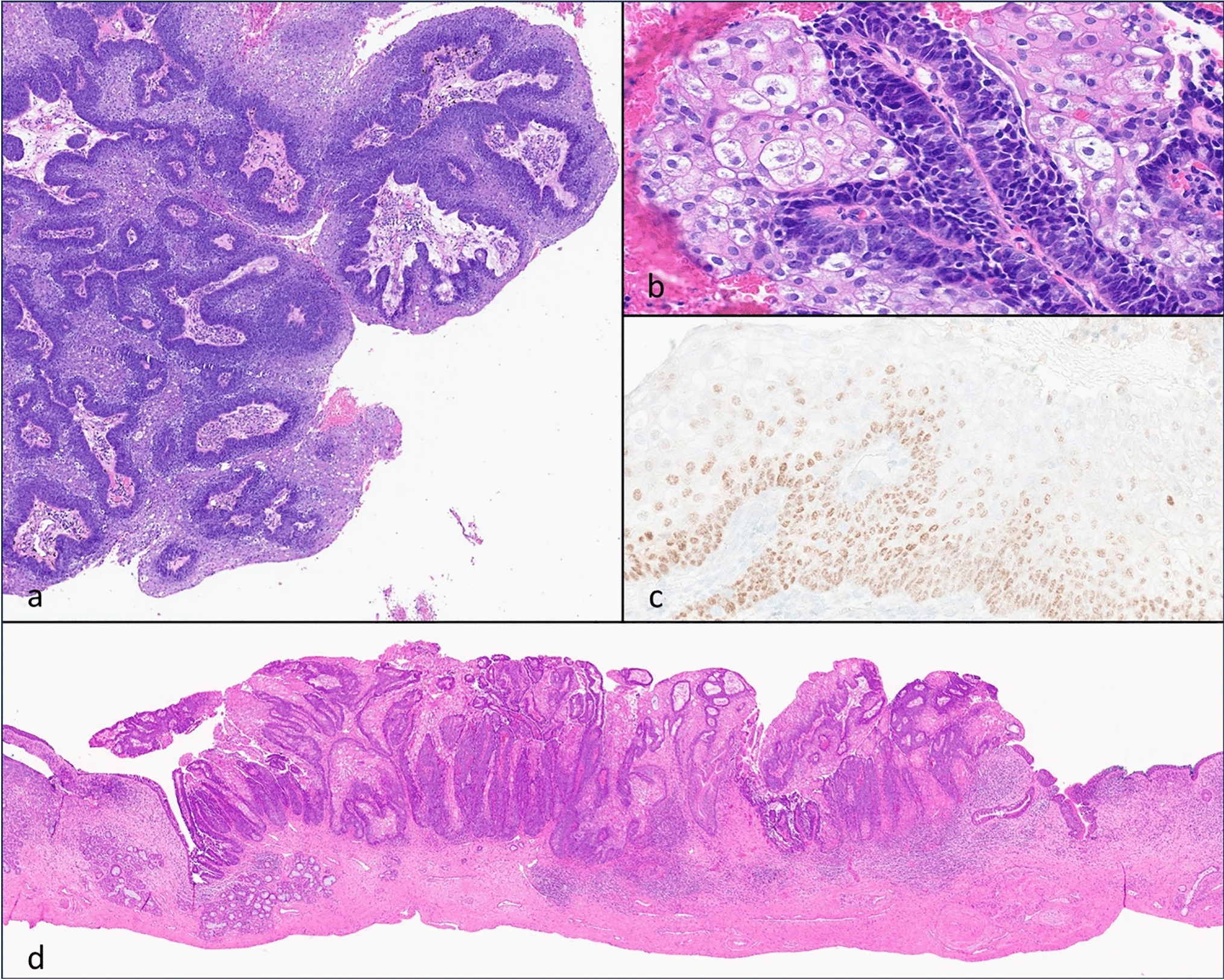
Diagnosing MiNEN necessitates a comprehensive evaluation throughout the tumor tissue, given the varied possibilities in proportions of NEN and non-NEN components. Consequently, it is not infrequent to miss the diagnosis on small diagnostic biopsies, only to discover MiNENs on examination of excised samples [2]. Intriguingly, the initial biopsy was able to identify mixed histopathological features in only a third of cases [11]. To confirm the presence of NEN elements with neuroendocrine differentiation, immunohistochemical markers including synaptophysin, chromogranin A, and INSM1 are highly recommended. Although CD56 is used in specific contexts, caution is advised in its interpretation. ISL1 has also been proposed for NEN identification [9]. In our case, there was positivity for all mentioned markers, albeit with varying degrees. Additionally, immunohistochemistry for tumor suppressor proteins, including p53 and Rb1 can be useful in detecting gene abnormalities, which is common in NEC [9]. Our case revealed overexpression of p53 and focal positivity of Rb1, consistent with prior studies on NEC in the head–neck region [12]. P16 staining is typically considered evidence of HPV-related oncogenesis, but its overexpression may not be HPV-related, as Alos et al. found no HPV DNA in p16-overexpression head–neck NECs [13]. Although the precise HPV status by in situ hybridization in our case could not be analyzed, p16 immunostaining behavior was not interpreted as typical HPV-related lesion. Besides, these molecules expression did not show difference between NEC and SCC parts. In summary, our case exhibited two distinct components positive for neuroendocrine markers and marked positivity for squamous cell differentiation markers, leading to a diagnosis of MiNEN.
Given the limited number of cases available, uncertainty persists whether the prognosis of MiNEN aligns more closely with that of NEN or its non-NEN constituents. Recent review have proposed that the biological behavior of MiNENs is predominantly influenced by the NEN component, which tends to be poorly differentiated and often found in distant metastatic sites [11]. In the context of head and neck region, the cancer-specific survival (CSS) rates for patients with NEC at 5 years were reported at 43% [14], whereas CSS for patients SCC in the head and neck region stood notably higher at 63% [15]. These findings underscore that the prognosis of NEN, especially NEC, is notably poorer than that of SCC. In our case, the Ki-67% labeling index for the NEC component was 71%, whereas the SCC component showed a lower index of 54.2%. This suggests that the biological behavior of the NEN counterpart is more active than its non-NEN counterpart. Notably, patients with MiNEN faced a poorer outcome as compared to those with pure NEC in the small intestine and appendix, although there were no significant survival differences between NEC and MiNEN in other parts of the gastrointestinal system [16]. This raises the possibility that the prognosis of MiNEN may be more aggressive than NEC, although it could potentially be site specific. In the reviewed cases of oral MiNENs [4,5,6,7,8], a high proliferation index (over 50%) did not seem to correlate with poorer outcomes, suggesting that proliferation rate may not be the key determinant of outcomes. Also, in our case, the patient underwent surgical treatment alone and remained in good health during the 6-year follow-up period.
In addition to our presented case and the cases reviewed, there have been reports of potential MiNEN cases in head and neck, including nasal cavity, sinonasal tract, oropharynx, palatine tonsil, larynx, hypopharynx, and parathyroid [17,18,19,20,21,22,23,24,25]. Notably, data from these studies consistently point to SCC as the predominant non-NEN component [4,5,6, 8]. Nevertheless, this observation aligns with the fact that SCC is the most common cancer in the head and neck region, ranking the sixth most common cancer worldwide [26]. MiNEN associated with SCC have gained recognition across the following anatomical sites: sinonasal tract, oropharynx, larynx, lung, esophagus, cervix/vagina, and skin [9]. However, the precise characterization of MiNEN in oral and other head and neck locations remains undefined. We believe that establishing an understanding of this entity is advisable. With the absence of treatment guidelines, reported oral MiNENs typically undergo surgery, with or without adjunctive radiotherapy. While the prognosis appears favorable, uncertainties persist, prompting the need for further research to clarify its clinical course and outcomes.



留言 (0)