
Remember me





Nuclear protein in testis (NUT) carcinomas (NCs) are rare, clinically aggressive carcinomas that are characterized by a translocation involving the NUTM1 gene on chromosome 15q14 and, in most cases (~ 70–80%), the bromodomain-containing 4 (BRD4) gene on chromosome 19p13.1, resulting in a BRD4-NUTM1 fusion oncogene [4, 5]. Other variant rearrangements include the BRD3-NUTM1 fusion (~ 15–20%) [6] and NSD3-NUTM1 fusion (~ 6%) [7], among partner genes (zinc finger ZNF52, ZNF592 in ~ 2%) [8]. In a subset of malignant solid tumors from soft tissue and other organs of uncertain relationship to NCs, NUTM1 has been reported to be fused with other genes (YAP1, MXD1, MXD4, CIC, BCORL1, ATXN1, and MGA); these genes have been described to occur in high-grade sarcoma associated with a distinct pathogenetic pathway (reviewed in Moreno et al. [9]).
NCs are composed of undifferentiated basaloid cells with focal, often abrupt, squamous differentiation [10]. NCs can mimic other undifferentiated neoplasms, such as pediatric small blue cell tumors, germ cell tumors, Ewing sarcoma, lymphoma, or SNUC. NUT carcinomas have an epithelial immunophenotype and focally express keratin, p63, CK7, CK20, and CK34, which reflect varying degrees of squamous differentiation. An extensive panel of lineage immunomarkers (e.g., desmin, myoglobin, smooth muscle actin, muscle actin, chromogranin, synaptophysin, leukocyte common antigen, placental alkaline phosphatase, S100 protein, alpha fetoprotein, neuron-specific enolase, CD57, CD99, HMB45) are not expressed in NCs. Oncoviruses, such as Epstein‒Barr virus and HPV, have not been reported thus far in NCs; their presence would likely exclude this diagnosis. Demonstration of the NUT translocation is needed for definitive diagnosis of NCs; this can be achieved by karyotyping, reverse transcription polymerase chain reaction, fluorescence in situ hybridization (FISH), and next-generation sequencing (NGS)- or whole-exome sequencing (WES)-based approaches (reviewed in Moreno et al. [9]).
Immunohistochemistry for NUT represents an acceptable surrogate marker, with NCs showing a nuclear staining pattern. Immunostaining with a monoclonal antibody to NUT has a sensitivity of 87%, a specificity of 100%, a negative predictive value of 99%, and a positive predictive value of 100% in distinguishing NCs from other poorly differentiated sinonasal carcinomas [11]. Given the anecdotal favorable responses of NUTs to certain treatment regimens, including chemotherapy according to Ewing sarcoma protocols or docetaxel and radiotherapy [12, 13], the distinction of NCs from other sinonasal carcinomas appears to be of clinical relevance. Targeted therapy using small-molecule BET inhibitors has shown activity but no obvious survival benefits, most likely due to toxicity effects [14]. Any poorly differentiated midline carcinoma or head and neck tumor lacking lineage-specific differentiation markers should be considered for immunostaining for NUT or rearrangement testing.
MYC has been shown to be a downstream oncogene target of BRD4::NUTM1 that blocks NC cellular differentiation and maintains a proliferative state [15]. The transcription factor SOX2 (sex-determining region Y-box protein 2), which is essential for stem cell self-renewal and pluripotency, is also an oncogenic target of BRD4::NUTM1 [16, 17]. BRD4::NUTM1 has been shown to drive overexpression of SOX2 in NUT carcinoma cells, which induces an aberrant stem cell-like growth feature [17]. Sox2 expression is normally restricted to stem cells; its aberrant overexpression has been linked to the ability to promote tumorigenicity and a poorly differentiated morphology [18,19,20]. Sox2 expression and gene amplification have been identified as common events in the head and neck [21, 22]; in the sinonasal region, amplification and/or overexpression of Sox2 has been demonstrated in squamous carcinoma (SNSCC), sinonasal undifferentiated carcinoma (SNUC), adenoid cystic carcinoma (AdCC), and intestinal type adenocarcinoma (ITAC) [22,23,24]. Although the literature is controversial regarding SOX2 amplification/Sox2 expression, recent data highlight the driver role of SOX2 in stemness with Sox2 overexpression and poor outcomes in patients with solid tumors [25]. Sox2 expression is also associated with resistance to chemotherapy through a plethora of mechanisms, and as such is a promising target for anticancer therapy [22, 26].
Tumor-specific antigens (TSAs) and tumor-associated antigens (TAAs) have been discovered within recent decades [27]. TSAs may result from gene mutations or from the expression of alternative open reading frames, resulting from chromosomal rearrangements; normal tissues frequently carry TAAs, with the drawback of autoimmunity development in parallel to conferring tolerance to these antigens through vaccination and tumor recognition 27,28,29]. Preferentially expressed antigen in melanoma (PRAME) is a testis-selective cancer testis antigen with restricted expression in somatic tissues and re-expression in various cancers. PRAME has gained interest as a candidate target for immunotherapy [30]. PRAME plays a role in the acquisition of various cancer hallmarks, including replicative immortality or stemness, invasion, and metastasis [30]. In addition to supporting tumor features, PRAME has been implicated in the regulation of the immune response [31].
In a recent study that aimed to characterize the immune-oncology gene expression profile in sinonasal undifferentiated carcinomas (SNUCs) and other high-grade sinonasal carcinomas, PRAME was the top upregulated gene in SNUCs and SWI/SNF-deficient sinonasal carcinomas (fold change 8.40), and fold change half values (4.8) were observed for high-grade neuroendocrine carcinomas (HGNECs) [32]. PRAME protein overexpression has also been noted in some NUT carcinomas (D Bell unpublished observations).
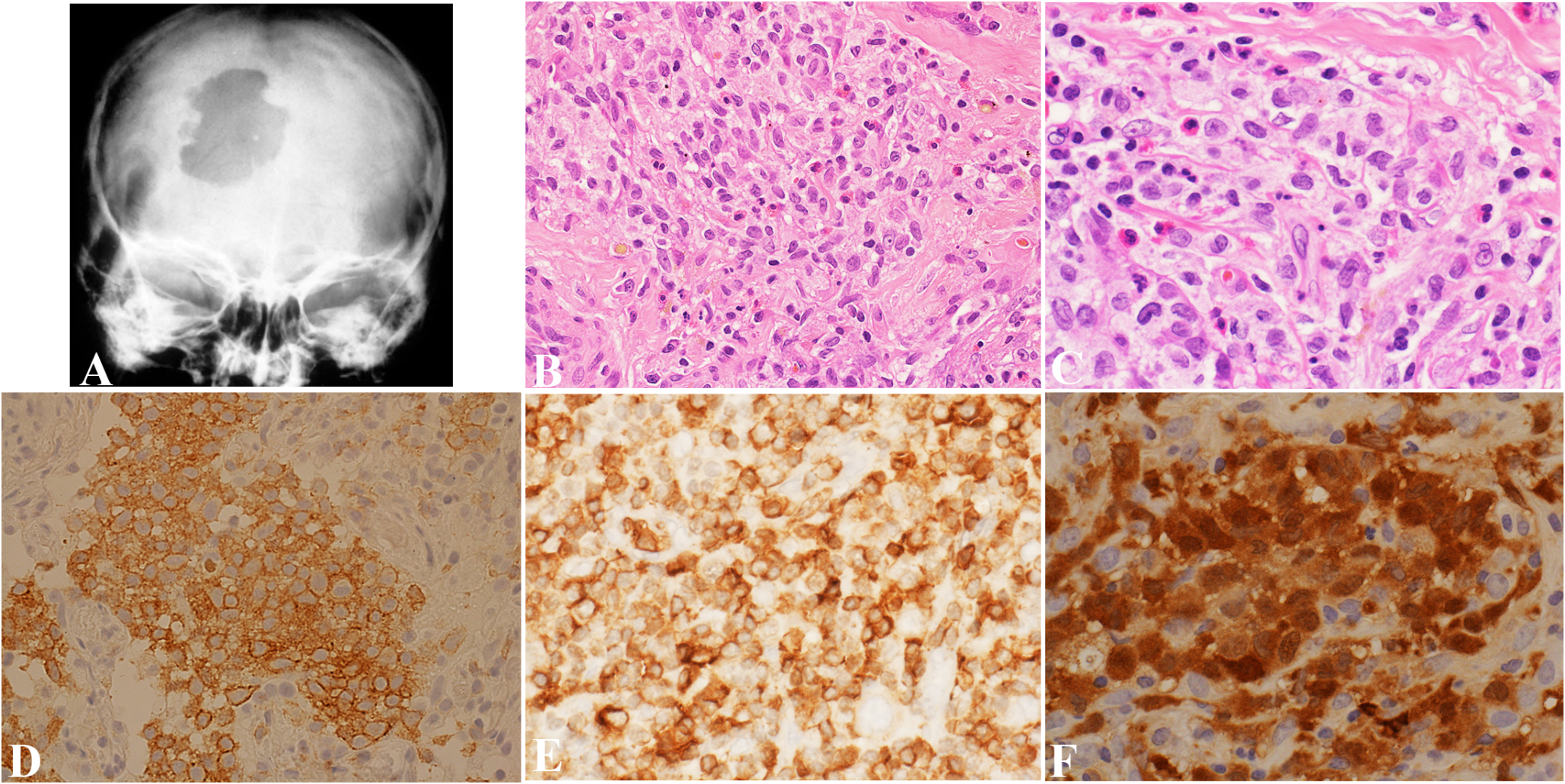
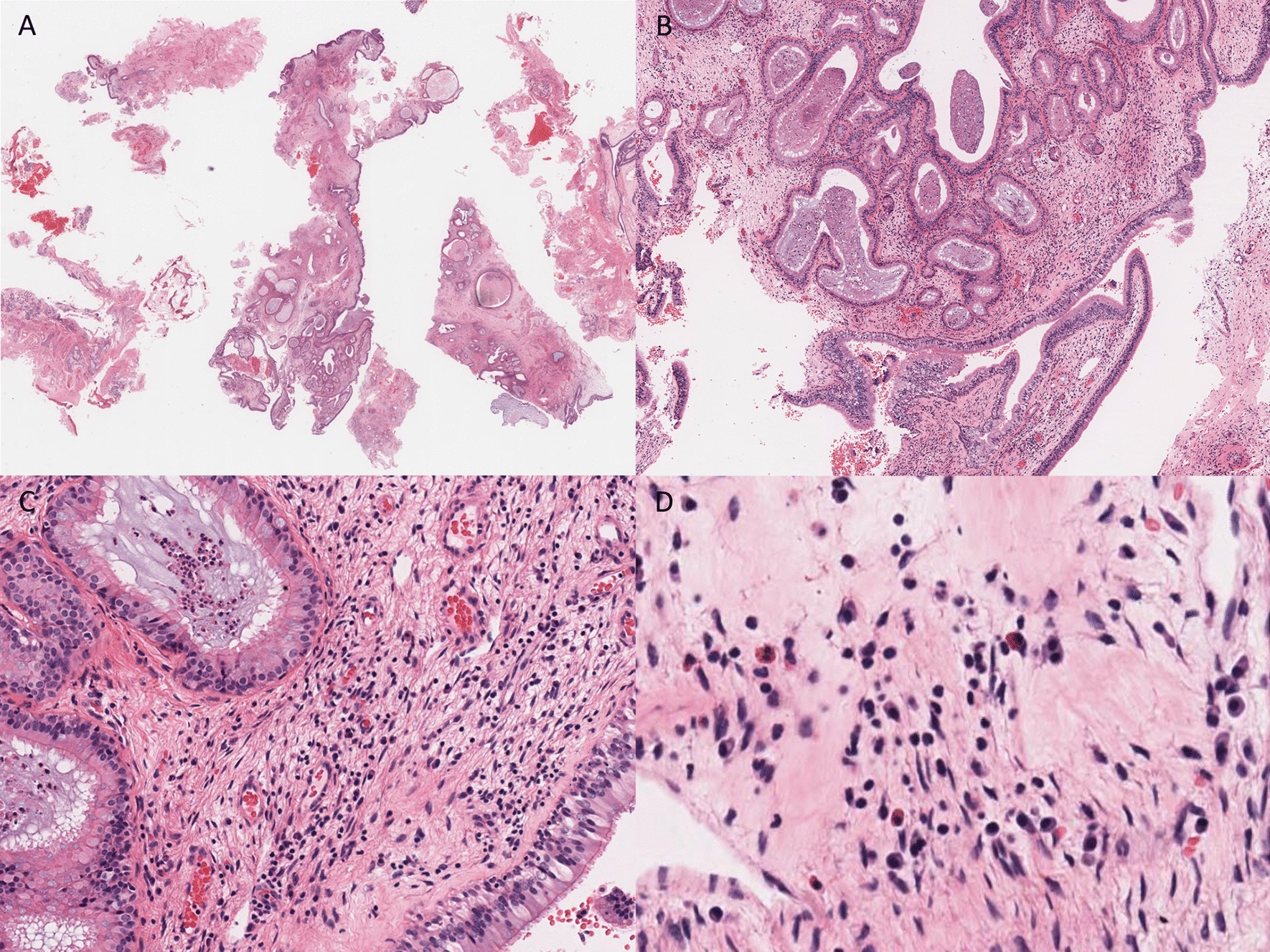
Salient morphological features of NUT carcinoma, with immunohistochemistry for NUT surrogate diagnosis, SOX2 and PRAME as promising anticancer targets, are illustrated in Fig. 1.
Fig. 1
NUT carcinoma. (A, B) Salient morphological features- monotonous proliferation of round small-to-medium-sized cells; abrupt keratinization and foci of squamous differentiation with larger cells with eosinophilic cytoplasm and pearl formation; (C, D) Immunoperoxidase staining with anti-SOX2 (C) and anti-PRAME (D), as promising anticancer targets
Sinonasal Lymphoepithelial Carcinoma (SLEC)Similar to other anatomical sites, sinonasal lymphoepithelial carcinoma (SLEC) is composed of sheets of undifferentiated malignant epithelial cells intimately intermingled with chronic inflammatory infiltrate. Malignant cells are often EBV positive [33], as shown by in situ hybridization for EBV-encoded RNA (EBER); serology for EBV-encoded RNA is also available.
The presence of lymphocytic infiltration, EBV expression, and the lack of neuroendocrine markers helps to differentiate SLEC mainly from SNUC and HGNEC.
High expression of somatostatin receptor 2 (SSTR2) has been documented in nasopharyngeal lymphoepithelial carcinoma, thymic LEC and salivary LEC 34,35,36,37,38]. SSTR2, a G-protein-coupled cell surface receptor, inhibits cell proliferation and is mainly expressed in neuroendocrine tumors. Lechner et al., in their large cohort of nasopharyngeal carcinomas, proposed a prognostic role for SSTR2 expression, with higher expression associated with increased survival rates [35]. High expression of SSTR2 is helpful as a diagnostic biomarker by imaging and an increased uptake of specific radiocontrast in EBV + NPC [39]. Targeted therapeutic strategies with SSTR2 agonists have also been studied with agonists prolonging progression-free survival in patients with metastatic enteropancreatic neuroendocrine tumors grade 1 or 2 (Ki67 < 10%) [40].
In view of SSTR2 diagnostic, imaging and therapeutic implications extrapolated from nasopharyngeal carcinoma studies, along with SSTR2 sensitivity and specificity for LEC, SSTR2 testing in SLECs is encouraged. Figure 2 depicts a nasal septum EBER-positive undifferentiated carcinoma, with strong expression of PRAME and SSTR2.
Fig. 2
Sinonasal lymphoepithelial carcinoma. (A) H&E- conventional morphology, with syncytial undifferentiated malignant cells set in a rich lymphoid background (Regaud pattern). (B) Presence of Epstein–Barr virus confirmed by EBER in situ hybridization. Immunostainings with (C) PRAME and (D) SSTR2
Sinonasal Undifferentiated Carcinoma (SNUC) and IDH2-Mutant Sinonasal CarcinomasThe WHO redefined SNUC as a highly aggressive and clinicopathologically distinct carcinoma of uncertain histogenesis that typically presents with great local aggressivity and tendency to metastasize [41]. SNUC is reputed to be refractory to even the most radical therapy and to carry a poor prognosis, particularly when the tumor transgresses the cranial base [42, 43].
In general, SNUC presents high chemosensitivity to cisplatin-based regimens, and a partial or complete response to induction chemotherapy is considered a favorable prognostic factor. Definitive chemoradiation is therefore usually recommended, while surgery is used as a salvage treatment in cases of persistence or recurrence [44].
SNUC arises from the sinonasal epithelium and therefore is of ectodermal derivation. In light of the overlapping clinical, anatomical, microscopic, and ultrastructural findings in olfactory neuroblastoma (ONB) and neuroendocrine carcinoma (NEC), their origins may share both cells of sinonasal respiratory mucosa and cells of olfactory neuroepithelium [45]. It has also been proposed that SNUC would be best categorized as a large-cell neuroendocrine carcinoma (reviewed in [46]).
SNUC is regarded as a diagnosis of exclusion. The immunohistochemical panel stains positively for epithelial markers (AE1/AE3, CK7, CAM5.2, EMA), p16, CD117, and focal p63 and negatively for CK5/6, p40, CEA, EBER, CD34, desmin, S100 protein, and calretinin. Neuroendocrine markers (synaptophysin, chromogranin, INSM, CD56) may be present.
An SNUC subtype with mutations in the Krebs cycle enzyme IDH2 is well characterized. IDH2 p.R172S is the most common mutation (55%); other mutations in the same codon (R172M, R172T, and R172G) have been described, and IDH1 mutations have rarely been reported [41, 47]. The spectrum is expanding, with IDH2 mutations documented in poorly differentiated high-grade carcinomas occurring in the sinonasal/paranasal anatomical boundaries as well as a handful of high-grade olfactory neuroblastomas [48]. As hypermethylation and upregulation of the repressive H3K27 epigenetic mark are hallmarks of IDH2-mutated carcinomas, DNA methylation-based classification is conceivable [48]. Given the therapeutic implications of IDH inhibitors, paralleling acute myeloid leukemia, some authors advocate for the classification of IDH2-mutated sinonasal tumors as a separate entity.
To date, no morphological or phenotypical differences between IDH-mutant and IDH-WT carcinomas have been recognized. Antibodies that recognize IDH1/2 (pR132/172) are a surrogate for diagnosis confirmation (granular cytoplasmic staining pattern); however, molecular testing validation is recommended. An example of a maxillary SNUC IDH2 mutation is shown in Fig. 3; the genomic event was confirmed by NGS studies.
Fig. 3
Sinonasal IDH2- mutated carcinoma. (A) H&E- Submucosal lobules of undifferentiated malignant cells, with large nuclei and prominent nucleoli (B) H&E. Diffuse immunoreactivity with anti-mutant IDH1/2 pR132/172, confirmed by molecular NGS
SWI/SNF Complex-Deficient Sinonasal CarcinomasSinonasal carcinomas characterized by rhabdoid/basaloid morphology and loss of expression of the SWI/SNF complex (SMARCB1, SMARCA4, SMARCA2), previously viewed as a subset of SNUCs, are recognized as a standalone entity in the 5th edition WHO Classification of Head and Neck Tumours [49]. Separation from the other types of sinonasal malignancies is justified, as the identification of SWI/SNF complex deficiency may provide a new target for novel treatment approaches and may ultimately lead to improved patient survival [50].
Available antibodies for SMARCB1/INI1 (BAF47) and SMARCA4 (BRG1) are routinely employed surrogates (FISH and NGS molecular studies offer verification of these genomic alterations). The tumor is positive for pancytokeratin and variably positive for CK5/6, p63/p40, and CK7; focal reactivity for synaptophysin and chromogranin is evident. P16 immunostaining is often positive but is not associated with the presence of HPV. HPV, EBV, and NUT are negative. Complete loss of SMARCB1 (INI1) is mandatory (SMARCA4 expression is retained); conversely, loss of SMARCA4 (with preservation of SMARCB-1/INI1) is diagnostic (Fig. 4a, b). Co-loss of SMARCA2 is occasionally observed [51].
Fig. 4
SNI/SWI complex-deficient sinonasal carcinoma. (a) SMARCB1/INI1-deficient sinonasal carcinoma. (A). H&E. Undifferentiated carcinoma (with large nuclei and prominent nucleoli) (B) Diffuse immunoreactivity with anti-p16. (C) Complete loss of expression of SMARCB1/INI1 (immunoperoxidase study with anti INI1/BAF47, with internal positive control/endothelial cells). (D) Patchy and weak expression of synaptophysin. E) Diffuse loss of expression of PTEN (correlated with NGS findings). (b) SMARCA4-deficient sinonasal carcinoma. (A, B) H&E- High-grade rhabdoid cells and rhabdoid appearance. Complete loss of expression of SMARCA4 visualized by immunostaining with anti-BRG1 (vascular internal control highlights nuclear signal and retention)
The spectrum of SWI/SNF-deficient sinonasal carcinomas currently includes the following: (1) SMARCB1-deficient sinonasal carcinoma, (2) SMARCB1-deficient sinonasal adenocarcinoma (with unequivocal glands or yolk–sac pattern), (3) SMARCA4 undifferentiated carcinoma, and (4) SMARCA4-deficient subset of teratocarcinosarcoma [51].
Sinonasal Nonkeratinizing Squamous Cell Carcinoma (SNKSCC) NOSA morphologically distinct sinonasal carcinoma (prior terminology as transitional, cylindrical cell, Schneiderian, and Ringertz carcinoma) is composed of cytologically atypical neoplastic cells arranged in ribbons that lack maturation and significant keratinization. Two subtypes have been added to the 5th edition WHO Classification of Head and Neck Tumours [52]: (i) HPV-associated – NKSCC defined by the presence of transcriptionally active HPV high risk and (ii) the emerging entity of DEK::AFF2 NKSCC characterized by recurrent DEK::AFF2 fusions 53,54,55]. Morphological differences between NKSCC-NOS and these subtypes of carcinomas are not appreciated.
SNKSCCs are diffusely positive for keratins CK5/6 and 34ß12 (CK903) and for p63 and p40; negative for synaptophysin, chromogranin, and INSM1, although occasional discrete or focal positivity for neuroendocrine markers is accepted; negative for NUT and EBV; and show retained SMARC expression. An example of NKSCC-NOS is shown in Fig. 5. Methodologies for DEK::AFF2 fusion confirmation include RNA sequencing, DEK FISH, or surrogate AFF2 antibody [56].
Fig. 5
Sinonasal nonkeratinizing SCC, NOS. (A, B). H&E Nonkeratinizing squamous cell carcinoma with ribboned arrangement (A) and discrete keratinization (B- 200 × magnification). (C) Diffuse positivity with anti-p40 antibody and (D) scattered anti-INSM1 reactivity. (E) PRAME is diffusely expressed within tumor cells. Viral studies (EBER, HPV-hr) are negative (not illustrated)
Sinonasal Teratocarcinosarcoma and Sinonasal High-Grade Poorly Differentiated Sinonasal Carcinomas NOSSinonasal Teratocarcinosarcoma (STCS)TCS is a rare skull base and sinonasal tract malignant tumor composed of carcinomatous, sarcomatous, and immature neural elements [57]. The most frequent sites are the ethmoid and maxillary sinuses and the nasal cavity in elderly male patients [58].
Morphologically, the tumor is characteristically composed of a high-grade carcinomatous component admixed with sarcomatous and immature neural elements. This tumor causes a diagnostic dilemma if only a dominant component is present on small biopsy samples. The TCS phenotype mirrors its constituent components: cytokeratin immunoreactivity within the epithelial component, CK5/6, p40, p63 for squamous elements, conventional neuroendocrine markers (chromogranin, synaptophysin, INSM1) highlighting the neuroepithelial component (and occasionally focally positive in epithelial), reactivity for myogenic markers (desmin, MyoD1, myogenin), SATB2, and SOX9 in sarcoma elements. Markers of germ cell derivation AFP, PLAP, and hCG are usually negative; however, positivity for SALL4 can be observed, and SALL4 immunohistochemistry appears to be relatively sensitive and specific for the diagnosis of TCS [59, 60]. Recurrent SMARCA4 alterations resulting in loss of SMARCA4 (BRG1) have been documented in up to 70% of studied TCS cases [61, 62]. Aberrant nuclear ß-catenin localization has been reported in a subset of TCS [61].
Despite major technological advances instrumental in refining the classification of sinonasal carcinomas, high-grade poorly differentiated sinonasal carcinoma NOS constitutes a temporary default diagnosis for a subset of cases. Figure 6 offers an illustrative example of a high-grade carcinoma arising from the middle turbinate in a middle-aged man (case from author files). The histological appearance is dominated by the presence of surface epithelial dysplastic transformation with endophytic epithelial growth of complex architectural patterns (ribboned, glandular, sieve-like spaces, ciliated neoplastic epithelium, and Schiller-Duval-like elements). No sarcoma elements are identified upon thorough sampling and examination of surgical specimens. The lack of all traditional neuroendocrine and conventional germ cells (AFP, PLAP, glypican, hCG) adds to the diagnostic challenges. SALL4 and PRAME expressions inform the pluripotential embryonic stem/germ cell origin. Comprehensive molecular NGS studies have not resulted in a more definitive diagnosis.
Fig. 6
High-grade sinonasal (“Schneiderian”) carcinoma NOS (arising from the middle turbinate). (A–D) H&Es. The histological appearance is dominated by the presence of surface epithelial dysplastic transformation with endophytic epithelial growth of complex architectural patterns (ribboned, glandular, sieve-like spaces, ciliated neoplastic epithelium, and Schiller-Duval-like elements (D) Diffuse immunoreactivity with anti-CK7 (E) and limited CK5/6 expression (F). No sarcoma elements are identified upon thorough sampling and examination of surgical specimens. The lack of all traditional neuroendocrine and conventional germ cells (AFP, PLAP, glypican, hCG) adds to the diagnostic challenges. SALL4 (G) and PRAME (H) expressions inform the pluripotential embryonic stem/germ cell origin. Comprehensive molecular NGS studies have not resulted in a more definitive diagnosis
Sinonasal Neuroendocrine Carcinoma (SNEC)Sinonasal neuroendocrine carcinomas (divided into small- and large-cell carcinomas) are almost always high-grade tumors with morphological and immunohistochemical evidence of neuroendocrine differentiation, characterized by a dismal prognosis and a high tendency to produce systemic metastasis. The most common location is the nasal cavity (40%), followed by the ethmoid sinus and maxillary sinuses (~ 20%), sphenoid sinus (13%), and frontal sinus (2%).
The 5th edition WHO Classification of Head and Neck Tumours relocates sinonasal small-cell neuroendocrine carcinomas [63] (SmCNECs) and large-cell neuroendocrine carcinomas [64] (LCNECs) into a dedicated neuroendocrine tumor section in an effort to unify neuroendocrine tumor terminology across organ systems. Regardless, their diagnostic criteria have not changed, with a minimum of 10 mitoses per 2 mm2 and Ki67 > 20% being mandatory.
The immunohistochemical profile includes positivity for cytokeratins AE1/AE3, Cam5.2, CK8/18 (frequently with a perinuclear dot distribution), and neuroendocrine markers (synaptophysin, chromogranin, INSM1- variable expression). The Ki67 mitotic index is more than 20%, usually ~ 70–80%). SNECs may benefit from induction chemotherapy followed by concurrent chemoradiation; surgery can be performed in nonresponsive cases or as a salvage treatment.
There is an ongoing effort to apply and validate novel lung small-cell (SCLC) molecular subtyping and biomarker-driven therapy for SNEC. According to RNA expression with validation at the protein levels of the transcription factors ASCL1, NEUROD1, POU2F3, and YAP1, four SCLC subtypes have emerged: SCLC-A (ASCL1-driven), SCLC-N (NEUROD1-driven), SCLC-P (ASCL1/NEUROD1-double negative with POU2F3 expression), and SCLC-Y (YAP1-related and NOS) and SCLC-I (inflamed gene signature), which share the last subtype 65,66,67,68,69]. SCLC-Is exhibit the greatest response to the addition of immunotherapy to chemotherapy, while the other subtypes each have distinct vulnerabilities, including to inhibitors of PARP, Aurora kinases, or BCL-2 [68].
Achaete-scute homolog 1 (ASCL1) is a powerful player in modulating neuroendocrine differentiation in tumor cells. ASH1 expression levels are inversely associated with the degree of tumor differentiation (high-grade tumors show increased expression of this protein), which correlates well with studies indicating that the expression of ASCL1 appears to be restricted to immature cells 70,71,72,
Comments (0)