
記住我
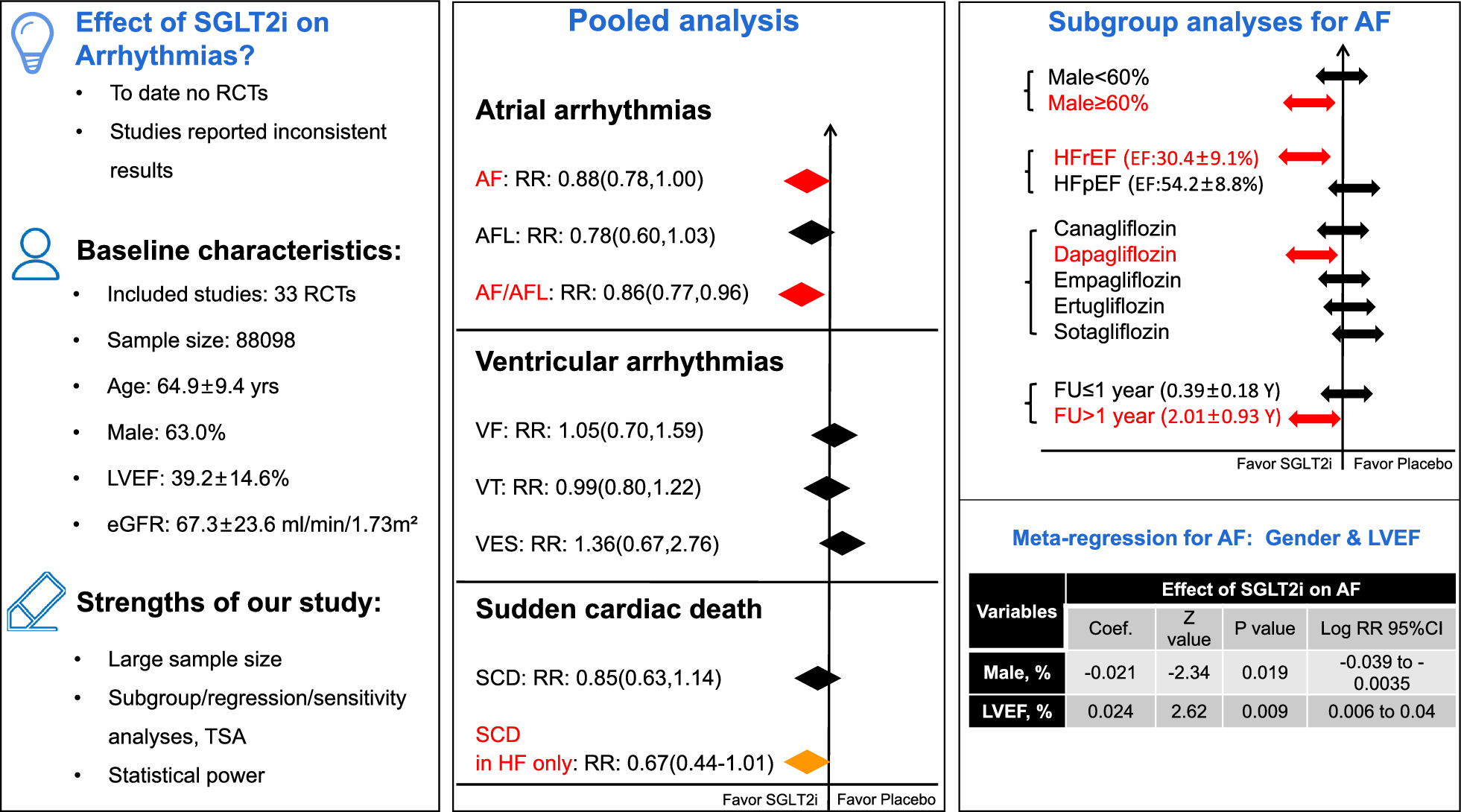
As illustrated in (Fig. 5), in this large meta-analysis including 33 placebo-controlled RCTs, we found that SGLT2i is associated with significantly lower risks of AF and composite AF/AFL, specifically, the this favorable effect of SGLT2i appeared to be substantially pronounced in patients with HFrEF, male gender, dapagliflozin, and longer follow-up (> 1 year). For SCD, only in heart failure patients, SGLT2i were found to be associated with a borderline lower risk of SCD. No significant effects of SGLT2i on other outcomes were found. To our knowledge, this is up to date the largest meta-analysis that investigated the association between SGLT2i and arrhythmic events.
Fig. 5
Central illustration—Insight from a large meta-analysis of randomized data focusing on effect of SGLT-2 inhibitors on arrhythmia events
The mechanisms for cardiovascular protective effects of SGLT2iSGLT2i has been shown to be cardioprotective by multiple mechanisms that may also contribute to decrease the risk of arrhythmias. Previous studies have shown that empagliflozin can ameliorate atrial structural and electrical remodeling as well as improve mitochondrial function and mitochondrial biogenesis in T2DM, and it may be potentially used in the prevention of T2DM-related AF [23,24,25]. Overexpression and Ca2+-dependent activation of Ca2+/calmodulin-dependent kinase II (CaMKII) has been recognized as a key mechanism of HF, leading to contractile dysfunction and arrhythmias [26]. Mustroph et al. found that SGLT2i can reduce CaMKII activity and CaMKII-dependent sarcoplasmic reticulum Ca2+ leak, which may contribute to the favorable effects of SGLT2i on improving cardiac function and preventing arrhythmias [27]. In addition, SGLT2i has been found to inhibit the sodium-hydrogen exchange in myocardial cells, suppress the sympathetic nervous system and reduce the accumulation and inflammation of perivisceral adipose tissue, leading to antiarrhythmic effect [28,29,30].
SGLT2i and atrial arrhythmiasWe found that compared with placebo, SGLT2i was related to a 12% lower risk of AF and a 14% lower risk of the composite events of AF/AFL. The effect of SGLT2i on atrial arrhythmias has been reported in a previous meta-analysis. Li et al. identified a 18% risk reduction in both AF and the composite events of AF/AFL with SGLT2i treatment [18]. However, in the present meta-analysis, substantially more patients (88,098 vs. 52,115) and larger number of RCTs (33 vs. 22) including recently published RCTs were enrolled, which allows for further subgroup analyses, regression analysis, and statistical power estimation. Thus the results found in our analysis appeared to be robust and relevant.
Further, our subgroup analysis found that SGLT2i significantly reduced the risk for AF and composite AF/AFL by 34% and 32% in patients with HFrEF, whereas there was no significant association between SGLT2i and risk of AF or composite AF/AFL in patients with HFpEF. It’s known that AF and HFrEF frequently coexist and significantly promote each other. The mechanism underlying the association between AF and HFrEF has be recognized as multifactorial, e.g. atrial pressure overload, altered myocardial conduction, structural and electrical remodeling, autonomic nervous disorder, and maladaptive gene expression etc. It has been reported that development of AF is linked with a significantly increased risk of HF re-hospitalization, all-cause mortality and stroke in patients with HFrEF [31]. Therefore, reducing the risk of AF represents an important target in patients with HF. As for HFpEF, our meta-analysis did not detect a significant association between SGLT2i therapy and lowed risk of atrial arrhythmias. One potential explanation may be that there were only two RCTs (EMPERIAL-Preserved trial and EMPEROR-Preserved trial) including patients with HFpEF. The DELIVER-HFpEF trial (NCT03619213) also explored the effects of SGLT2i in patients with HFpEF, but the arrhythmias-related results have not been published. Therefore further studies are needed before reaching definitive conclusion.
Interestingly, as shown in Fig. 4, we found that male gender was positively correlated with the favorable effect of SGLT2i on AF, suggesting that SGLT2i reduces the risk of AF more significant in men than it does in women. This result appears to be in line with the finding from a previous meta-analysis which showed that the reduction in MACE events with SGLT2i was significantly greater in men with diabetes than that in women [32]. It should be noted that in all the enrolled RCTs, male patients were mainly included, and 63% patients in this meta-analysis were male. This indicated the underrepresentation of female inclusion in SGLT2i trials, and further studies focusing on gender difference of SGLT2i in terms of different outcomes may be needed.
Moreover, different follow-up duration may impact the effect of SGLT2i. We found in the subgroup analyses that, pooled-results from RCTs with follow-up duration > 1 year yielded significant decreased risk of AF and composite AF/AFL (RR: 0.87, 95%CI 0.77–0.99 for AF; RR: 0.85, 95%CI 0.76–0.96 for the composite events of AF/AFL) in patients treated with SGLT2i, whereas there was no significant association found between SGLT2i and lowed risk of atrial arrhythmias in trials with < 1 year follow-up. This may suggest that, a shorter follow-up duration may be insufficient for SGLT2i to achieve significant effect on AF reduction.
In addition, our meta-analysis found that dapagliflozin was the only SGLT2i agent to substantially decrease the risk of AF or AF/AFL, while other SGLT2i agents showed only neutral effect on these endpoints. This raises the hypothesis that the antiarrhythmic properties of SGLT2i might be drug specific rather than class related, nonetheless, further researches remain warranted.
SGLT2i and ventricular arrhythmiasSGLT2i has shown to reduce all-cause and cardiovascular mortality in patients regardless of the presence of T2DM, HF, or CKD, however the association between SGLT2i and ventricular arrhythmias has been less well studied. In this meta-analysis we found that there were no significant differences in VT, VF, VES, and the composite events of VF/VT/SCD between the SGLT2i and placebo groups in overall comparisons or in subgroup analyses. However, we found that only in heart failure patients, SGLT2i were found to be associated with a borderline lower risk of SCD. Our finding seemed to be consistent with the results from an earlier meta-analysis [19]. In the DAPA-HF trial, SGLT2i resulted in lower incidents of ventricular arrhythmias (VT, VF, torsade de pointes), resuscitated cardiac arrest and SCD (5.9% vs 7.4%, HR: 0.79, P = 0.037) [33]. It should be noted that in the DAPA-HF trial, all patients had HF with reduced EF (31 ± 7%) and 55% of the patients had known ischemic cardiomyopathy.
What’s clinically relevant is that, our study found that SGLT2i lowered the risk of SCD only in heart failure patients instead of patients without HF, it’s therefore extrapolated that the effect of SGLT2i on reducing the SCD (or malignant ventricular arrhythmias) may be greater in those who had higher cardiovascular risk. On the other hand, our TSA and for sample size analysis suggested that the statistical power in terms of VF, VES and SCD was not adequate, thus further studies are needed to evaluate the association between SGLT2i and ventricular arrhythmias or SCD.
SGLT-2i: more HF treatment than the antiarrhythmic effect?As discussed, SGLT2i improves the prognosis of HF mainly by improving myocardial energy metabolism, suppressing inflammation, reducing oxidative stress, and preventing adverse cardiac remodeling, etc. These mechanisms can also be shared pathways in the prevention of cardiac arrhythmias. Currently, there is limited number of (preclinical or clinical) studies particularly focusing on the antiarrhythmic effect of the SGLTi. Based on the findings of our meta-analysis, the pronounced favorable effect of SGLT-2i in reducing the risk of arrhythmia was dominantly seen in patients with HFrEF rather than those without HF, it’s therefore likely that the reduced rate of arrhythmia from SGLTi seemed to be attributed to HF treatment instead of direct antiarrhythmic effect.
Strengths and limitationsDifferent from other studies, our study included the most recent RCTs, consisted of large sample size and wide spectrum of patient population, by which it increased the statistical power and enabled comprehensive, clinically-relevant subgroup analyses. We also looked into a broad spectrum of arrhythmias and events as our study outcomes, including AF, AFL, VF, VT, VES, SCD. All the included RCTs had high-quality in methodology, and no significant publication bias was observed. The robustness and stability of our primary results were further tested by sensitivity analysis, TSA and sample size estimation. Furthermore, meta-regression analyses and comprehensive subgroup analyses were performed based on gender percentage, diabetes status, HFrEF/HFpEF condition, eGFR classification, different SGLT2i agents and follow-up durations, from which new, clinically relevant results were found.
Several limitations should be acknowledged. First, the intrinsic heterogeneity in study design among different trials existed. Different trials were specifically designated for different patient group (e.g. T2DM, HF or CKD). Second, our meta-analyses were based on study-level data rather than patient-level data, and unknown baseline characteristics may potentially impact the study outcomes. Although the present analysis focused on new-onset arrhythmia events, patient-level data on pre-existing arrhythmia and the use of anti-arrhythmic medications were not available from all the included trials. Third, the arrhythmia events were mainly reported as SAEs rather than primary outcome in the individual trials, and these arrhythmia outcomes were identified during follow-up visiting. Although one may argue that all the patients were randomized so that the chance of bias (if there was) should be the same in the SGLT2i and in the control group, however without continuous heart rhythm monitoring, the incidence of those arrhythmia events could have been underestimated and biased.
留言 (0)