The data used in this study are part of a larger register linkage which was designed to conduct matched case–control studies to examine risk factors and matched cohort studies to examine outcomes. This register linkage design is an efficient way to conduct multiple investigations of the causes and consequences of sarcoidosis using the same dataset. In this study, we used these data to conduct a case–control study nested within the Swedish population.
Sarcoidosis cases and general population controls
We identified women with at least two inpatient or outpatient International Classification of Diseases (ICD)-coded visits for sarcoidosis (ICD-8/9 135, ICD-10 D86) in the National Patient Register (NPR; inpatient hospitalizations nationwide since 1987 and visits to outpatient clinics since 2001). A validation study showed that two ICD-coded visits for sarcoidosis in the NPR has a high positive predictive value (0.94) [19]. Women were required to have their first ever visit occurring in 2007–2020, allowing for at least 1.5 years of prescription data before sarcoidosis diagnosis since the Prescribed Drug Register (PDR) became available in July 2005. The PDR captures all prescription dispensations in pharmacies across Sweden since July 2005 including the date and route of administration [20].
Women receiving treatment for sarcoidosis at the time of diagnosis were considered having a more severe sarcoidosis (e.g. debilitating symptoms or organ involvement in need of treatment) [1]. In Sweden, the mainstay of sarcoidosis treatment is systemic corticosteroids and second-line treatment is methotrexate or azathioprine [1]. We classified women as receiving treatment at diagnosis if they had ≥ 1 prescription of either systemic corticosteroids [Anatomic Therapeutic Chemical (ATC) classification codes: H02AB01/02/04/06/07], methotrexate (L01BA01/L04AX03) or azathioprine (L04AX01) in the PDR ± 3 months from their first visit in the NPR listing sarcoidosis. For a subset of cases (n = 108) who were registered in a clinical cohort at Karolinska University Hospital in Stockholm, we retrieved information on sarcoidosis phenotype, i.e. Löfgren or non-Löfgren syndrome.
Women from the general population without sarcoidosis served as controls. Up to 10 population controls without any sarcoidosis visits in the NPR were randomly sampled from the Total Population Register (TPR) and were matched to each unique woman with sarcoidosis on year of birth and residential location at time of sarcoidosis, and required to be living in Sweden at the time the matched case was first identified with sarcoidosis (matching date).
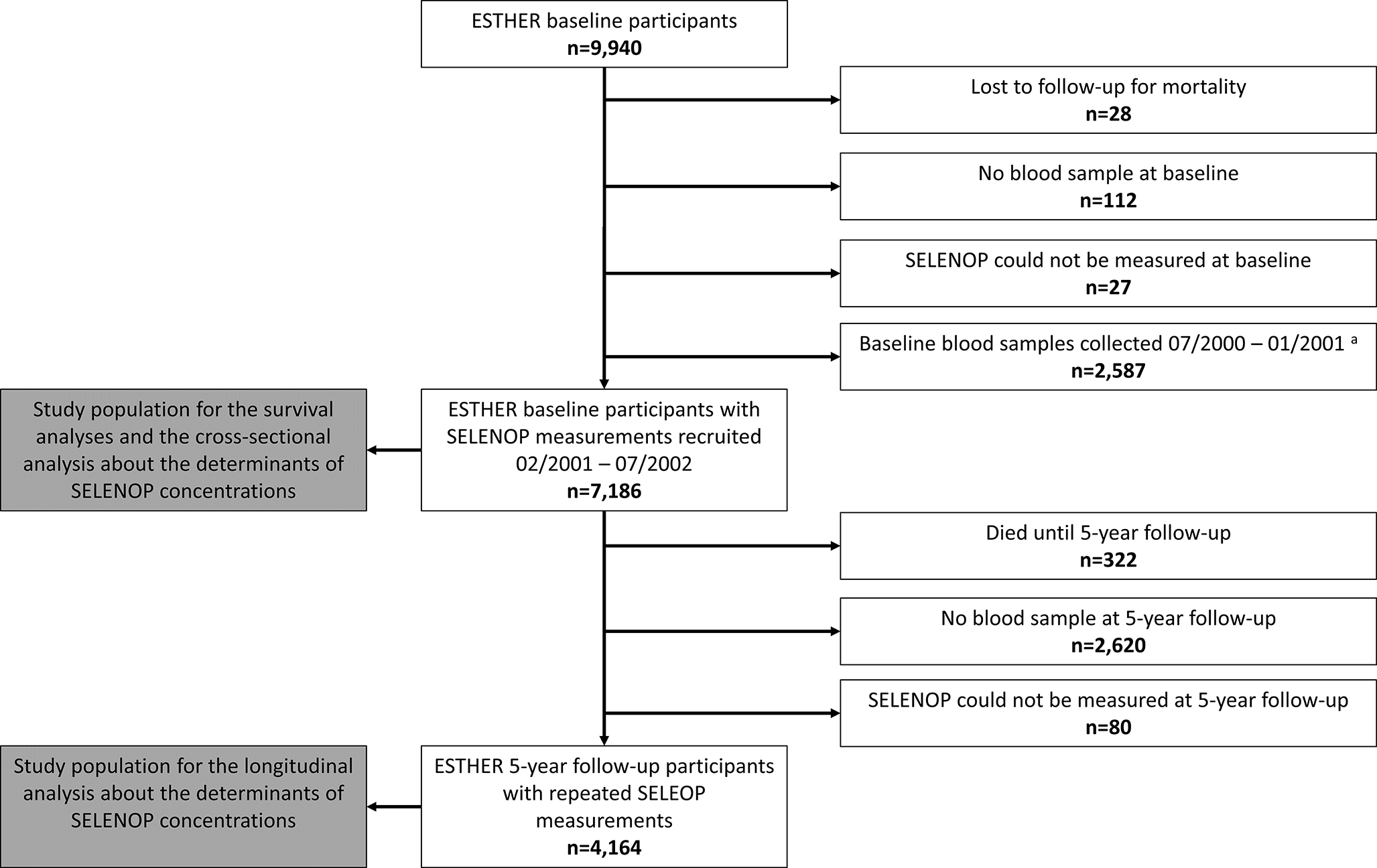
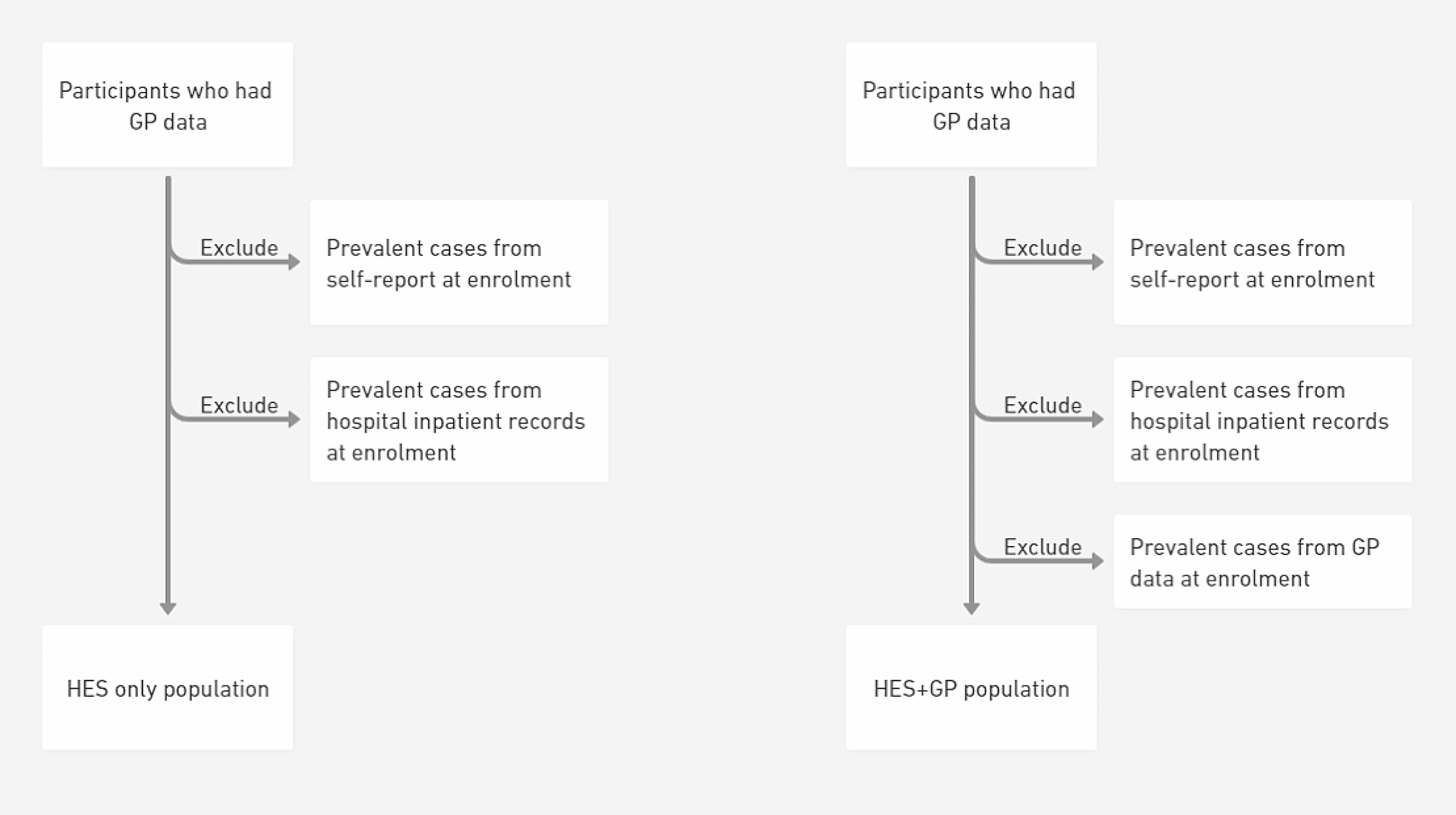
The study population was restricted to women 40 years or older to capture women of menopausal age. Women with a hematologic or lung malignancy diagnosis (ICD-7 162, 163, 200‒205) in the Swedish Cancer Register within 6 months before or after the first visit for sarcoidosis/matching were excluded to avoid including cases where cancer may have been misdiagnosed as sarcoidosis. Additionally, women with a diagnosis of breast cancer, endometrial cancer, cardiovascular disease (stroke, acute myocardial infarction, ischemic heart disease), venous thromboembolism or anticoagulant dispensation before the first visit for sarcoidosis/matching were excluded because they may have a contraindication for MHT use (see flow chart of study population in supplementary Fig. 1 and a list of ICD and ATC codes used for exclusions in supplementary Table 1).
Exposure: menopausal hormone therapy
To identify history of MHT use, cases and controls were linked to the PDR using each person’s unique identification number. Information on dispensations of MHT [ATC codes: G03C (estrogens), G03D (progestogen, if prescribed in combination with estrogens), G03F (estrogen combined progestogen), G03CX (tibolone; used as an alternative for continuous combined estrogen-progesterone hormone therapy which has androgenic properties); supplementary Table 2] was obtained from the PDR before sarcoidosis diagnosis/matching. Both systemic and local treatments were identified using the pharmaceutical form variable from PDR. Drugs for systemic MHT were defined as oral and transdermal products (i.e. oral tablets, dermal patches and dermal gel) and drugs for local MHT were defined as vaginal products (i.e. vaginal creams, rings and pessaries). A detailed description of the exposure variables is presented in Table1.
Table 1 Description of variables used to investigate menopausal hormone therapy (MHT) obtained from the Prescribed Drug RegisterPeople with undiagnosed/preclinical sarcoidosis might experience symptoms that mimic menopause, and receive MHT treatment for those symptoms. To mitigate this potential reverse causation, women whose first dispensation occurred within one year before the sarcoidosis diagnosis/matching were not considered exposed in main analyses.
Other variables
We retrieved demographic information from the TPR including the date of birth, country of birth (Nordic, non-Nordic, missing), and county of residence at diagnosis/matching (classified into healthcare regions: Stockholm, Uppsala-Örebro, West, South, Southeast, and North). From the Longitudinal Integration Database for Health Insurance and Labour Market Studies, we obtained data on education level at time of sarcoidosis diagnosis/matching (≤ 9, 10‒12, ≥ 13 years, missing), gross income in 2005 adjusted to 2019 inflation rate [21] (< 100, 100–< 300, ≥ 300 thousand Swedish krona, missing), and sick leave/disability pension during the year 2005 (0, 1‒49, 50‒199, 200‒364, ≥ 365 days, missing). Sick leave, disability and income were collected from 2005, to assure they were from before exposure and outcome, and not later in time when they could be mediators. When using data on sick leave, disability and income from the year before diagnosis, ORs were within ± 0.02 of the ORs using 2005 data. Women who use MHT may be systematically different in terms of socioeconomic and/or health status than women who do not use MHT. Therefore, we collected information on education and income as proxies for socioeconomic status, and number of days of sick leave/disability pension as a proxy for health status. From the Medical Birth Register, we retrieved data on number of births before sarcoidosis diagnosis/matching. It has been found that number of childbirths is associated with age at menopause [22] and to also be associated with sarcoidosis [11, 12]. A family history of sarcoidosis is the strongest risk factor for sarcoidosis, and is a proxy for genetic risk [23]. We therefore searched for biological first-degree relatives (parents, full siblings and offspring) of cases and controls in the Multi-Generation Register and identified those with at least two sarcoidosis diagnoses in the NPR (family history of sarcoidosis – yes; no) at any point in time.
Statistical analysis
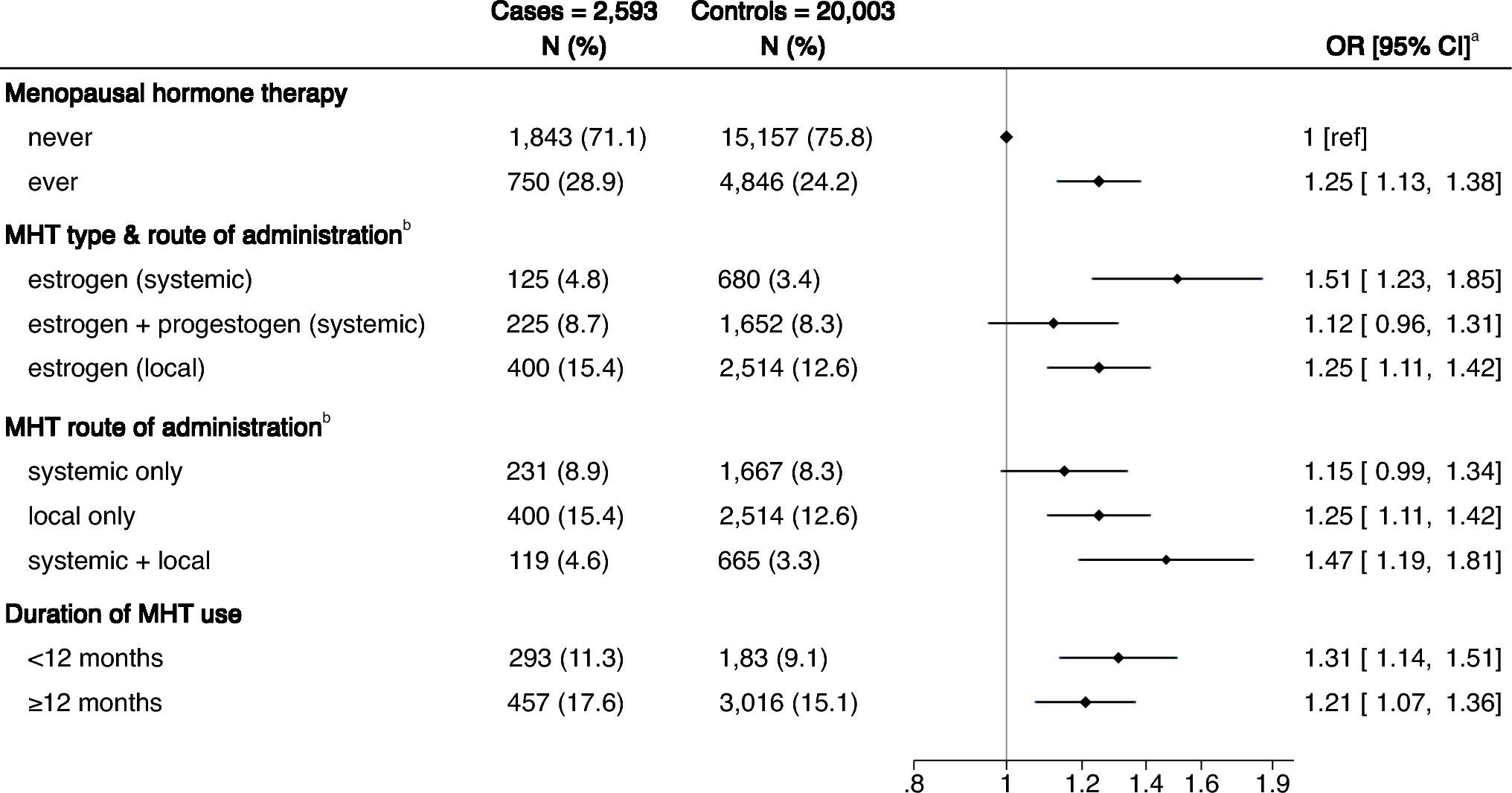
Characteristics of sarcoidosis cases and general population controls were reported as means with standard deviations, or as proportions. Conditional logistic regression models were used to estimate adjusted odds ratios with 95% confidence intervals (aOR; 95% CI) for the associations between MHT use, type of formulation, route of administration, and duration of use with incident sarcoidosis. MHT type and route of administration were considered together but since some women with systemic estrogen and with combined estrogen-progestogen had a history of local estrogen, we also considered the route of administration alone. We adjusted for age, education, income, sick leave/disability pension, number of births and family history of sarcoidosis.
A subgroup analysis by age at diagnosis/matching (< 60; 60–69; ≥70 years) was conducted to assess whether the association between MHT and sarcoidosis varies by age.
To address the heterogeneity of sarcoidosis, we investigated the association separately for treated and untreated sarcoidosis. Furthermore, to investigate whether misclassification of our register-based definition for sarcoidosis affected our results, we restricted to cases in the Karolinska clinical cohort who have medical record-confirmed diagnoses. Moreover, we examined Löfgren and non-Löfgren syndrome separately using data from the clinical cohort.
We stratified by time from first MHT dispensation to sarcoidosis diagnosis or matching (0 to 7 years) to investigate whether the OR varied by the time since MHT dispensation.
Three separate sensitivity analyses investigating potential misclassification of MHT were conducted. (1) Since the PDR was established in July 2005, we had incomplete information on the first dispensation date (left censoring) so to see if this affected results we included women who had their first ever visit occurring in 2010–2020, allowing for at least 4.5 years of PDR data, (2) we used a stricter definition for MHT, requiring at least two dispensations for MHT in the PDR, and (3) since tibolone has not only estrogenic and progestogenic properties, but also androgenic, we excluded women who received tibolone before sarcoidosis diagnosis/matching.
Since MHT is not used only for menopausal symptoms in a small group of women, we excluded non-menopause indications for MHT to test if those indications affected results (a list of ICD and ATC codes used for exclusions in supplementary Table 3).
We tested the robustness of the results against the potential unmeasured confounding of smoking and obesity using probabilistic bias analysis [24, 25]. Smoking and obesity have been found to be associated with both sarcoidosis [26,27,28,29] and women’s sex hormones [30, 31]. The assumptions for the analysis are described in the supplementary methods.
The relative risk (RR) can be computed from the OR as RR = (OR)/[(1 − P) + (P * OR)], where P is the prevalence in the unexposed [10]. With a sarcoidosis prevalence of 160/100,000, an OR of e.g. 1.25 corresponds to RR = 1.20, i.e. practically the same as the OR. We therefore refer to higher/increased odds as higher/increased risk.
Data management and statistical analyses were performed using SAS software (version 9.4; SAS institute Inc., Cary, NC, USA). Forest plots were performed using STATA software (version 16.1).

留言 (0)