The survey used the Standardized methodology of the World Health Organization and International Health Action Organization (WHO/HAI) for a survey of prices, availability and affordability of medicines [10].
Study design
This study used a descriptive cross-sectional research design with a quantitative approach.
Areas surveyed
According to the standard survey method for drug accessibility research developed by the World Health Organization (WHO) and Health Action International (HAI), the scope of this survey must first be determined. This means that a survey can be conducted nationwide or regionally. For countries with vast areas of land or large populations, it is recommended that surveys can be based on regions. Considering the size and administrative divisions of Juba County, this survey selected five peripheral payams and one municipal Payam that hosts Juba City. This made up a total of six payams (administrative areas), namely: Kator payam, Rejaf payam, Juba payam, Munuki payam, Luri payam and Mangalla payam. A Payam is a second-lower administrative division in the South Sudan administrative categories below the county. All the selected six payams are reachable in a 1-day drive as per the recommendation from the WHO/HAI manual [10].
Juba County is located in Central Equatoria state and is the largest county among the 79 counties of South Sudan. The estimated population was 499, 538 by 2020. It hosts the capital city of South Sudan and has become a multi-ethnic centre. The county has 17 payams in which many health facilities are located.
Sectors and health facilities surveyed
Prices and availability of medicines were recorded from 55 health facilities comprising 15 Public health facilities, 18 private pharmacies, 18 private clinics and 4 faith-based health facilities across 6 Payams of Juba County. In addition, the central procurement data were obtained from HPF national office (grown agent) as it purchases medicines for the government of South Sudan. This collection of central procurement data is recommended by WHO/HAI methodology.
Initially, a sample size of 58 health facilities was drawn using the WHO/HAI sampling technique from the list of 365 active health facilities (from all four sectors) obtained from the county health department. From the selected 58 facilities, 3 public health facilities were excluded, because they did not stock the survey medicines as they were specialized centres for TB, HIV/AIDS and nutrition programs; therefore, data were collected from 55 health facilities only. The surveyed health facilities comprise 6 hospitals and 49 primary health care centres (PHCC) (Table 1).
Table 1 Distribution of the surveyed areas, health facilities and sectorsSample size
The sample size of this study was calculated using the WHO/HAI methodology which recommends that a main public medical outlet is purposefully chosen as the starting point and the rest of the medical outlets are selected based on their proximity to the main medical outlets. Using this WHO/HAI methodology for the selection of survey institutions, a total of fifty-eight (58) medical outlets (18 public outlets, 18 private pharmacies, 18 private clinics and 4 faith-based facilities) were selected for this study. All 58 medical institutions were selected in the areas within 3-h drive from the main health facility to comply with the recommendations of the methodology. This sample size was representative considering the fewer number of public medical facilities in Juba County. From the selected 58 facilities, 3 public health facilities were excluded, because they did not stock the survey medicines as they were specialized centres for TB, HIV/AIDS and nutrition programs; therefore, data were collected from 55 facilities only.
Sampling procedures
One major public facility was selected in each survey area and two other public medical institutions were randomly selected within a 3-h driving radius from the six public facilities that were initially selected in the first stage. Based on this criterion, a total number of 18 public medical facilities were selected in six payams. 18 retail pharmacies, 18 private clinics and 4 faith-based facilities were selected based on their proximity to the pre-selected public medical facilities. Therefore, this study intended to survey a total number of 58 different medical outlets sampled from four different sectors. The technique used here adapts the sampling procedures provided by the WHO/HAI methodology that involves many sequential steps. The first step of this sampling technique required that the main public medical outlet in each of the six study areas (designated Payams in this research) was chosen as a reference and then select the other 5 nearest public medical outs in each of the study areas. However, this procedure was not fully followed in this study, because there were fewer public medicine outlets in Juba County. Therefore, in this adapted Methodology, two public facilities nearest to the main medicine outlet were selected in addition to 1 main public facility to make three. This constitutes a total of eighteen selected public medical outlets in each of the six payams. Three private pharmacies and three private clinics were selected based on their proximity to the pre-selected main public health facility in all the six payams. If two or more private medical outlets had similar distances from the pre-selected main public medical outlet, then the survey outlets were selected using the simple random technique. Only four faith-based health facilities in Juba County were included in the sample for the survey.
Medicines selection criteria
Medicine selection was based on the updated WHO/HAI core List and the South Sudan tracer medicines list. Only 11 of the 14 medicines on the WHO/HAI core list and 15 tracer medicines were included in the study. Three medicines (simvastatin 20 mg, bisoprolol 5 mg and captopril 25 mg tab.) from the WHO/HAI core list were excluded, because they were not on the updated South Sudan Essential Medicines List (SSEML). They were replaced by three other therapeutically equivalent medicines (atorvastatin 40 mg, propranolol 40 mg and lisinopril 10 mg) on SSEML. All the medicines included in this study had international reference prices (IRPs) in the Medicines Price Indicator Guide provided by the Management Sciences for Health (MSH) version of 2015 and were authorized for sale in the Republic of South Sudan. The dosage forms, package size, and treatment regimens were confirmed in the South Sudan essential medicines list and standard treatment guidelines in collaboration with healthcare providers. Hence, this study collected data on 29 medicines drawn from the WHO/HAI core list and tracer medicines list of South Sudan (Table 2). These medicines were used at the hospital level (Level 3). However, 27 were used at the primary healthcare centre (Level 2), and 22 were used in the primary healthcare unit (Level 1).
Table 2 List of medicines that were surveyedData collection, entry and analysis
Data were collected using the data collection forms that were automatically generated from pre-programmed Excel workbooks obtained from the WHO/HAI website (https:/haiweb.org) after the entry and update of the core list of medicines provided by WHO and the local list of tracer medicines. Twelve data collectors were recruited and trained for 2 days. After the training was concluded, they were dispatched for data collection in six teams. Each team of two people was tasked to collect data in each payam. The data collection commenced on 10/03/2023 and was finished on 16/10/2023. The data collectors collected data in all four health sectors under the close supervision of the researcher. The sources of data were heads of departments in health facilities who consented to provide information about the availability of medicines and prices. Some of the challenges encountered during data collection include refusal to sign the consent form, absent of heads of departments, and difficulties in unit price calculation by data collectors, among others.
Data from the surveys were entered into the pre-programmed MS Excel Workbook provided as part of the WHO/HAI methodology. The Workbook's 'double entry' and 'data checker' functions were used to validate data entry. Errors and potential outliers were carefully verified and corrected.
Data analysis was carried out using the default settings of the automated Microsoft Excel worksheet created by WHO and HAI [10] which generated summary findings, such as percent availability, median price ratios, and cost for one treatment course. Further analysis was done to create graphs and pie charts using Microsoft Excel version 2010.
Measurement of availability of medicines
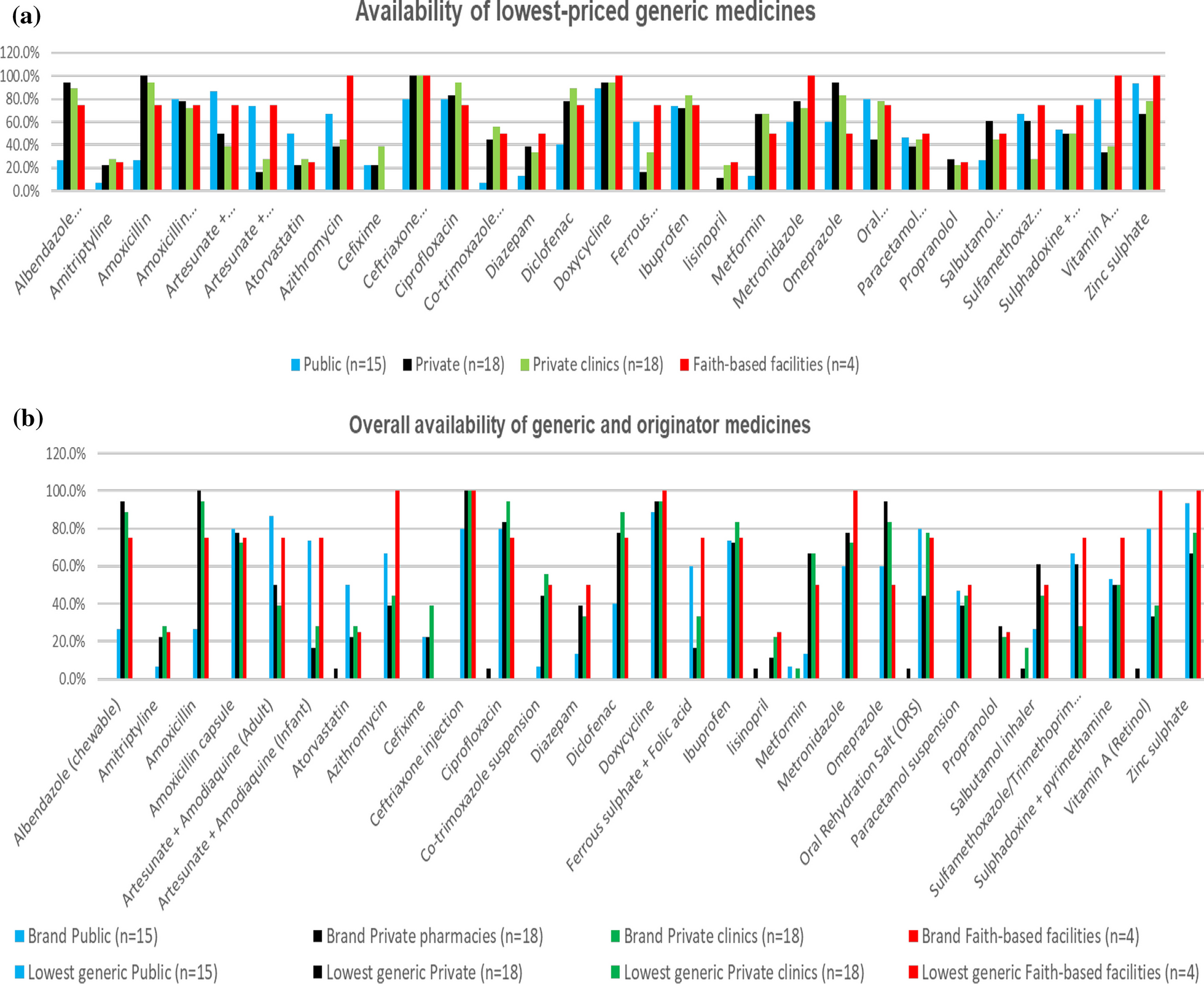
Based on the WHO/HAI methodology, individual medicine availability was determined by the physical presence of that medicine in medicine outlets at the time of data collection. As a result, availability was calculated and reported as a percentage (%) of sampled medicine outlets per sector, where the surveyed medications were found on the day of data collection [10].
Measurement of affordability of medicines
Medicine affordability was determined using the median patient prices of originator brands and the lowest priced generics of each medicine in local currency for a standard treatment regimen. As per the WHO and HAI methodology, affordability was expressed as the number of days' wages needed by the lowest paid unskilled government worker (LPGW) to purchase 30-day supply of the medicine to treat non-communicable diseases (NCDs) and 7-day supply of medicines to treat communicable diseases. If the cost of the full regimen does not exceed 1-day wage, then that medicine is considered affordable. The affordability was not assessed in health facilities, where medicines were not available and in public facilities, where medicines were provided free of charge. Any treatment course that requires more than 1-day wages is considered unaffordable by WHO and HAI. According to the information from the Ministry of Labor during the time of the survey, 1-day wage of the lowest paid unskilled government worker in South Sudan was 266.6667 SSP (equivalent to 0.3252 US$). The exchange rate in the Central Bank of South Sudan was 1 US $ = 820 SSP on April 2023. For medicines from the WHO and HAI global core list, the number of units for a course of treatment is defined in the WHO and HAI manual [10]. For the tracer medicines on the supplementary list, the South Sudan Standard Treatment Guideline was used to define each medicine's daily dose and treatment duration [11].
Prices assessment
The prices were evaluated using the international reference prices (IRPs) in the 2015 Management Sciences for Health (MSH) reference. IRPs are prices offered to international non-profit organizations for the purchase of generic medications. Medicine prices were recorded in local currency (South Sudanese pound, SSP) and they were automatically converted to US $ using the exchange rate from the Central Bank of South Sudan which was (1 US $ = 820 SSP), during the month of April 2023 in which the data were collected.
The following formula was used to express median local prices as ratios to international reference prices:
$$\mathrm\;\mathrm\;\mathrm\left(\mathrm\right)=\frac$$
MPR is an important indicator for assessing the availability of essential medicines, as well as the price level and international reference level of medicines in the survey area [12]. According to the WHO, an MPR of 2.5 is considered a high and excessive local price. This means that any MPR equal to or greater than 2.5 indicated that essential medicines were not affordable in Juba County.









Comments (0)