In our study, we demonstrated the feasibility of the use of overage of ICV ERT infusions for IVT ERT injections.
IVT ERT was a well-tolerated treatment for CLN2 related retinal dystrophy, which showed a statistically significant treatment effect even in patients approaching end stage CLN2 retinopathy.
Safety
During the study period, no serious ocular complications related to the treatment were detected. No previous literature describing IVT ERT in human patients exists, however in a previous study investigating the use of IVT ERT in dogs, severe anterior and intermediate uveitis developed. This raised a concern about possible pro-inflammatory properties of the drug. In our study, a careful slit lamp examination at each examination under anaesthesia did not detect any evidence of uveitis in human patients, suggesting that the inflammation seen in the canine model may be related to the use of xenogeneic (human) TPP-1 in the canine study.
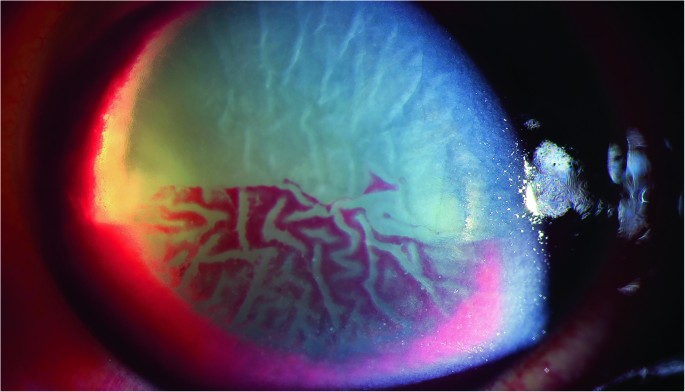
Two patients with the most severe vascular attenuation required the creation of an anterior chamber paracentesis following intravitreal injections in order to reduce the intraocular pressure since CRA occlusion was noted on indirect ophthalmoscopy immediately following intravitreal injections. Further work is required to understand whether immediate paracentesis is mandatory or not in such patients.
One systemic adverse event occurred in a patient who experienced laryngospasm following general anaesthesia. Anaesthetic complications highlight the importance of balancing any benefits of ocular treatment with IVT ERT against the risks of regular general anaesthesia. The possibility of performing intravitreal injections in this group of patients under sedation rather than general anaesthesia should also be considered in order to reduce anaesthetic risks.
Efficacy
This is the first study to report a statistically significant treatment effect of IVT ERT on the rate of macular volume loss in patients with CLN2 retinal dystrophy. Macular volume loss in CLN2 retinopathy is known to follow a reverse s-shaped curve, being stable in early life, followed by a rapid decrease between the ages of 4 and 7 and finally reaching a plateau once end stage disease is reached [7]. Since the study was designed to focus on safety, patients with very advanced CLN2 retinopathy were selected for treatment. Accordingly, 5 of 8 patients enroled had reached end stage degeneration prior to enrolment and serial OCT scans did not reveal any further volume change in either eye during the study period. 3 of 8 patients were in the actively degenerating phase of disease. IVT ERT was effective at reducing the rate of macular volume loss in all 3 patients who were in the progressive/actively degenerative phase of retinal thinning, although the treatment effect was modest. However, for patients in end stage disease, IVT ERT neither positively nor negatively influenced the macular volume.
Whilst the presence of a statistically significant treatment effect is encouraging, further work will be required to determine whether modification of the treatment protocol or the timing of intervention with respect to patients’ age can improve the efficacy.
Age at treatment initiation
The mechanism of action of TPP-1 is by restoring lysosomal protein catabolism in the neural cells of the retina, which in turn prevents cell death. It is, however, not a reparative treatment. Although three of eight children in our study had not yet reached end stage disease at enrolment, they did all have advanced disease. Previous work investigating the effects of ICV ERT on cerebral volume loss shows that rapid volume loss may persist for one year after initiation of treatment [2]. It is likely that treatment earlier in the course of disease will deliver higher efficacy. CLN2 is usually diagnosed before retinal degeneration begins and therefore there is a potential therapeutic window between diagnosis and the onset of retinal degeneration during which IVT ERT may prove more efficacious.
Dose and frequency
The dose of rhTPP-1 used in this study was chosen to replicate the dose that was found to be effective in the canine study. This was done by increasing the dose in proportion to the increased vitreous volume in humans as compared to dogs. However, the dogs were treated before the onset of degeneration and therefore the degree of lipofuscin deposition in the dog retinas as compared to our patients was likely to have been much lower. The retention of TPP-1 within neuronal lysosomes is related to the concentration of lipofuscin, therefore in patients with advanced disease, a loading dose at treatment initiation may be beneficial. Since no adverse effects of TPP-1 were found in this study, future study design should consider the use of a loading dose.
The frequency of IVT ERT was every two months in this study, compared to 6 weekly in the canine study. The frequency was reduced to 2 monthly in order to prioritise safety and the treatment burden of regular general anaesthesia however we did not increase the treatment dose to compensate for this. Since loss of rhTPP1 from lysosomes occurs at an approximately constant rate that is related to lipofuscin concentration and independent of rhTPP1 concentration [8] future studies could maintain an 8-weekly interval whilst ensuring the presence of a therapeutic concentration of TPP-1 by proportionately increasing the treatment dose per intravitreal injection.
Route of administration
Although intravitreal ERT was highly efficacious in the dog study, canine and human CLN2 retinopathy have very different phenotypes. In the canine model, inner retinal degeneration prevails, causing an electronegative ERG [5], whereas in humans outer retinal degeneration and a reduced ‘a’ wave are seen [4, 6]. Therefore, the intravitreal route may be less suited to human disease. Changing the route of administration to subretinal is not feasible as this approach would require repeated pars plana vitrectomy. It may however be possible to increase the concentration of TPP-1 in photoreceptors by administration of a higher dose intravitreally. It is unlikely that the inner retinal layers would act as an absolute barrier that would prevent TPP-1 from accessing the outer retina, since transport through the retinal layers is known to take place by mannose 6-phosphate dependent uptake and transcytosis [9].
Further work should also consider optimising the study design and addressing which outcome measures best reflect any potential benefit of treatment. Previous literature has suggested that CLN2 retinal dystrophy is a highly symmetrical condition [7]; our results confirm this. Therefore, a paired comparison between right (treated) and left (untreated) eyes should continue to be used in order to reduce the sample size required when investigating this rare disease. Our results show that paracentral macular volumes are robust and repeatable measurements, which are likely to be able to detect small differences between treated and untreated eyes. On the contrary, the use of optic nerve MRI did not detect any treatment effect in this group of patients with advanced disease but would be likely to be an important anatomical outcome if treating patients before the onset of retinopathy/optic neuropathy. In addition to anatomical outcomes, functional outcomes will also be required. In the present study, visual acuities are not reported because the patients’ neurological regression precluded them from engaging reliably in testing and because their retinal disease was very advanced at baseline. Similarly, patients’ ERG traces were already highly attenuated at baseline and therefore ERG evidence of a functional treatment effect was limited. In a future study investigating the effect of early treatment with IVT ERT in children who had been on ICV ERT since diagnosis, both visual acuity and ERG scores are likely to be important functional outcomes.
In conclusion, this study is the first to demonstrate the feasibility and safety of IVT ERT in human patients with CLN2 retinopathy and to demonstrate a treatment effect. The data gathered pave the way for a larger trial earlier in the course of disease, before the development of retinal thinning. Since IVT ERT is well tolerated, treatment could be commenced with a high loading dose to ensure a therapeutic drug concentration from the moment of initiation and continued with a maintenance dose higher than that used in the present study in order to ensure a therapeutic concentration is achieved in the outer retina. Initiating treatment in patients at an early stage of disease would allow the collection of high quality functional as well as anatomical data.
Supplemental material is available at Eye’s website

留言 (0)