
Remember me

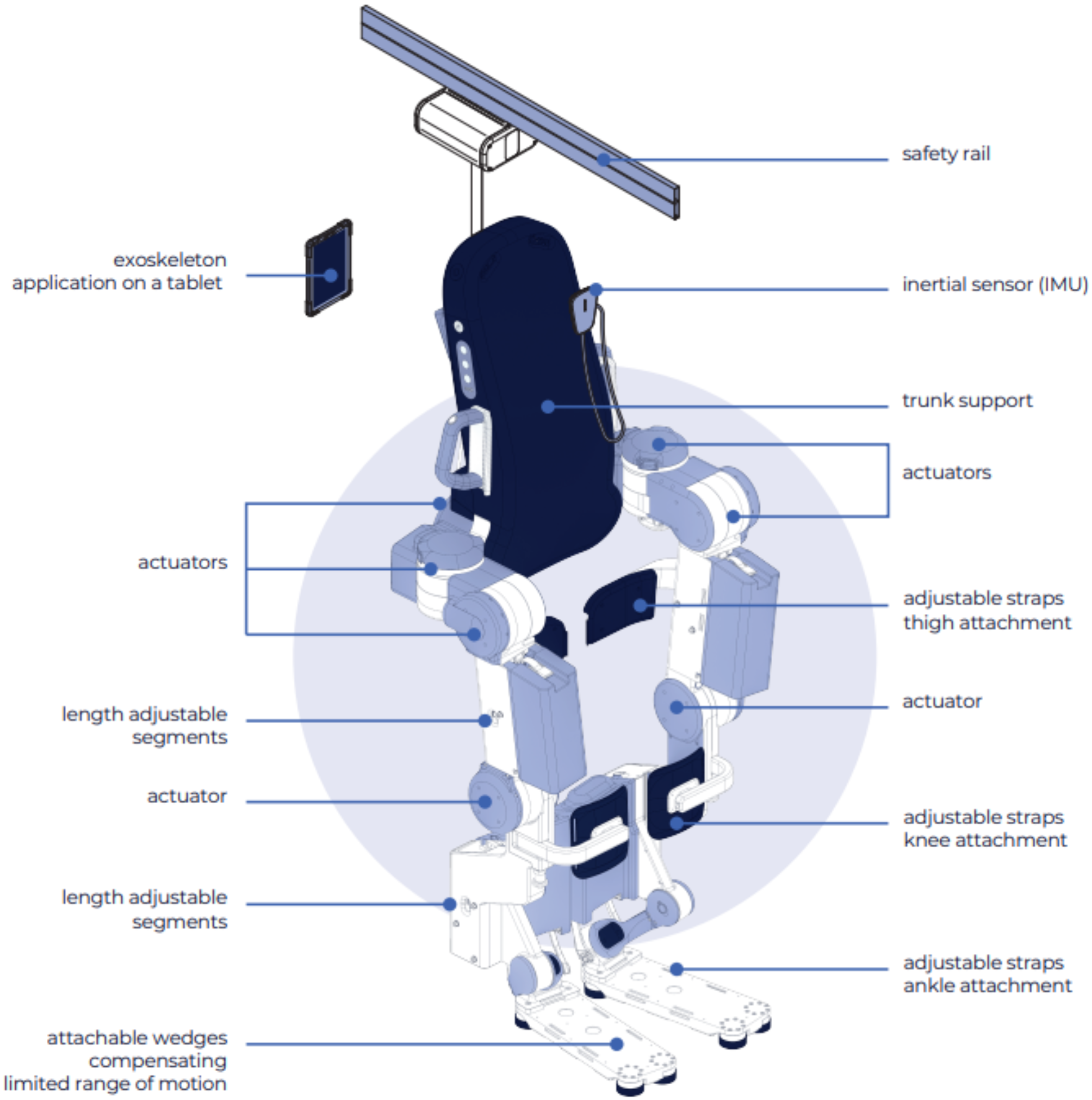




All subjects were alert throughout each experimental session even though they were not asked to engage in any task-dependent activation aside from relaxing. Robot-generated hand movements were always smooth, having unimodal, bell-shaped velocity profiles (Fig. 2A). Passive displacement of the hand modulated EMG activation in HS subjects (especially in stretched muscles) but rarely did so in NI control subjects. For example, stretching shoulder or elbow muscles in the hemiparetic arm caused EMG activation in some muscles to increase during movement (Fig. 2A, left), as might be expected due to spastic hypertonia (i.e. [41]. Interestingly, elevated muscle activation could remain active long after motion had ceased in some regions of the workspace, as might be expected due to a decrease in the stretch reflex threshold post-stroke [23], although other explanations are possible. In some muscles, tonic EMG activation after passive displacement of the hand appeared to depend on the final limb configuration (limb posture). Persistence of muscle activation was never observed in NI control subjects during or after passive movement (cf. Figure 2A, right).
Fig. 2
A Representative normalized movement kinematics (top) and normalized, rectified EMG signals (bottom) as a function of time for a single fast transition between targets C1 and B4 (grey) and a single moderate speed transition between targets C2 and B1 (red) in a representative HS subject (left). A single fast transition between targets C1 and B4 (grey) and a slow transition between targets C2 and B1 (red) in a representative NI control subject is shown on the right. Horizontal scale bar: 10 s. Vertical scale bar: EMG signal amplitude of 20% MVIC. Movement kinematics are displayed on an arbitrary scale to highlight general characteristics such as smoothness. The additional snippets of data to the right of each trace present data from the very end of the hold period (at least 25 s after the end of movement). Vertical dashed lines indicate the time of EOT + 2 s. B Spectrograms of BICS EMG signal power during MVIC trials (black) and quiet rest (blue) for the same subjects. Also shown for comparison for the HS subject (left) is the resting spectrogram multiplied by a factor of 5000 (purple)
Elevated EMG activations in HS subjects were not an artifact due to poor signal transduction or improper EMG normalization in these subjects. Because EMG normalization with respect to MVIC could overestimate voluntary muscular effort if the signals were corrupted by environmental noise, we visually verified that EMGs recorded from each muscle were of high quality by plotting the EMG signal power spectrograms from MVIC trials for each muscle and compared it to spectrograms obtained during quiet rest. In all cases, MVIC EMG signal power was distributed across the frequency range in a unimodal pattern characteristic of high-quality surface EMG recordings [35] (Fig. 2B, black). By contrast, EMG signal power was lower during rest in the center of the workspace (Fig. 2B, blue). MVIC EMG exceeded quiet resting signal power by a factor greater than 100 in all cases (≫ 20 dB signal to noise ratio). Thus, normalization with respect to MVIC yielded a high-quality assessment of relative voluntary effort. Note that while resting EMG power was uniformly negligible at all frequencies in NI subjects, it commonly displayed measurable, tonic activation post-stroke with a spectral signature of quality surface EMGs rather than broadband environmental noise (e.g. Figure 2B, left; purple).
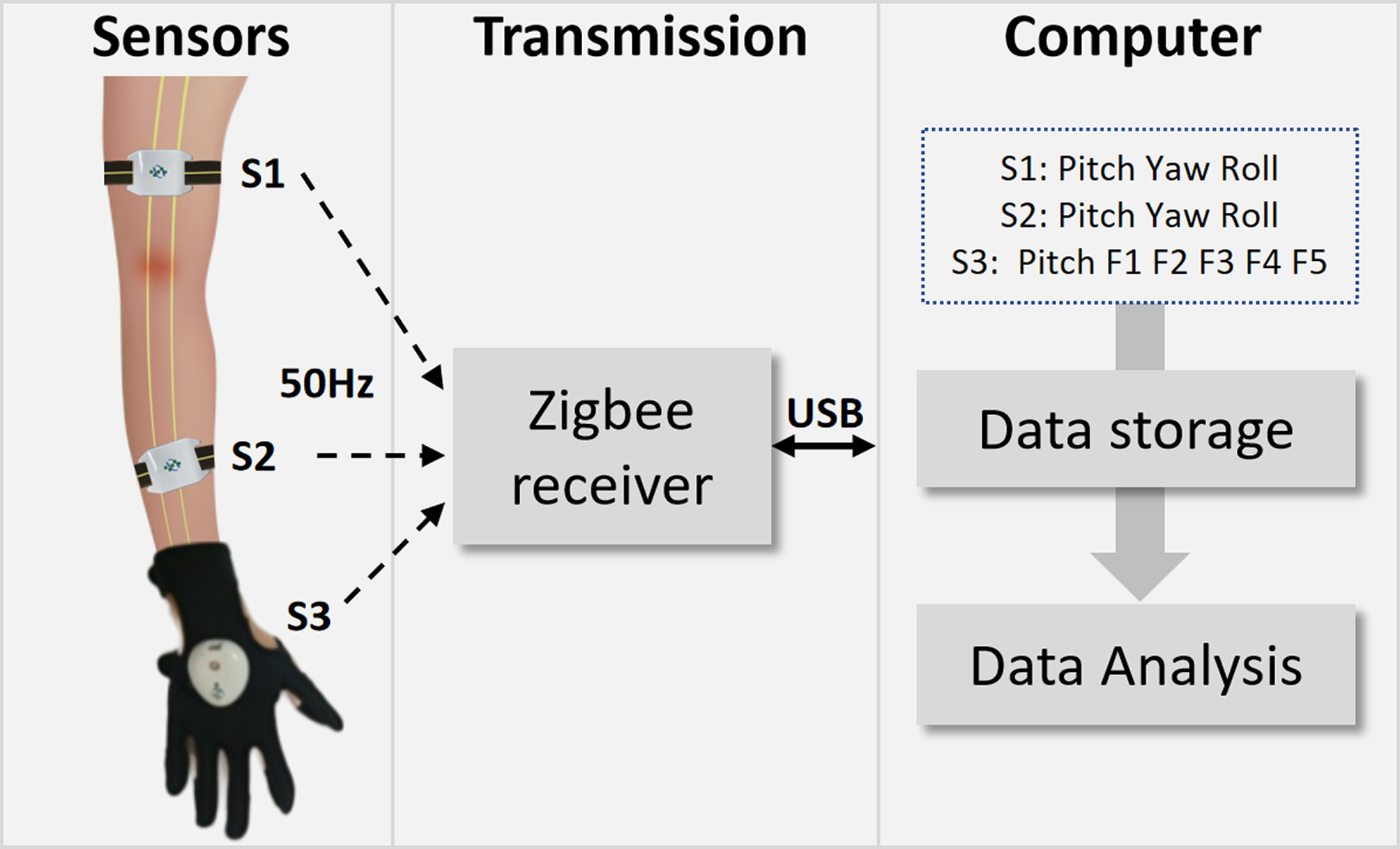
We sought to characterize how mechanical resistance to passive joint motion varied with movement velocity (i.e., spastic hypertonia; [21]. Visualization of raw hand forces from a selected HS subject (Fig. 3A) demonstrated that hand force magnitude could vary systematically by transport speed during movement, that variations in steady-state hand force were not systematic during the hold phase that followed, and that hand forces changed very little from EOT + 20 s onward. Despite efforts to minimize trunk motion, some trial-by-trial variability in hand force undoubtedly arose from subjects shifting in their seat during the ~ 1.5-h testing period. Because the effect of these infrequent postural shifts would be to alter the bias forces recorded at the handle throughout the trial, we reasoned that greater sensitivity in subsequent analyses of velocity-dependence would be achieved by removing the effects of postural shifts (i.e. by analyzing hand forces relative to their asymptotic values). Indeed, exploratory three-way repeated measures ANOVA found that hand force magnitude at EOT + 20 s post-stroke did not vary systematically with transport speed (F(3,207) = 1.40, p = 0.25). We therefore aligned the raw hand force profiles in time with respect to EOT and subtracted asymptotic values on a trial-by-trial basis (Fig. 3B) prior to evaluating how subject group, workspace location and other factors influence the transient effect of movement on reaction forces at the hand.
Fig. 3
A Hand force magnitudes as a function of time during transitions between targets as indicated by the red trajectory in Fig. 1 (panel B) for a representative HS subject (left) and NI control subject (right) at three transport speeds (90˚: thin trace; 30˚: medium-weight trace; 6˚: heavy trace). Markers (yellow +) indicate the time of End Of Transition (EOT). Markers (red hashes) indicate EOT + 20 s. Vertical scale bar corresponds to a measured hand force of 20N while the horizontal dashed line indicates 0 measured hand force. The horizontal scale corresponds to 10 s. B Force profiles plotted with respect to steady-state values (EOT + 20 s) and aligned in time with respect to EOT. Here, the vertical scale bar corresponds to a change in measured hand force of 20N relative to steady-state
Hand force measurements are repeatable across daysWe performed a six-way, mixed-model, general linear model, repeated measures ANOVA to quantify how changes in measured hand force magnitude (relative to EOT + 20 s) varied by subject group, movement speed, movement direction, workspace location (boundary vs center), temporal sampling instant and testing day in response to passive relocation of the subject’s hand from one workspace location to another. We found that testing day failed to demonstrate a significant main effect (F(2,4799) = 0.26, p = 0.769) and that this factor also had no interaction with any other factor (p > 0.21 in each case). Moreover, 78% of the Day 2 variations in hand force (across subjects, workspace location, speed, movement direction and sampling window) were predicted by measurements made on Day 1. From this we conclude that measurement of endpoint forces using our experimental approach was repeatable across days.
Effect of movement speed on measured hand forcesAlthough the ANOVA found no main effect of movement direction or workspace location on hand force (relative to steady-state) and no significant interaction between subject group and either of these factors, the analysis did find a significant three-way interaction between subject group, sampling instant and movement speed (F(14,4799) = 3.02; p < 0.0005). No other three-way or higher-order interactions achieved significance, indicating that the observed velocity-dependent effects did not vary systematically across the workspace after stroke. To test whether the observed three-way interaction could possibly have been due to alterations in the passive viscoelastic properties of tissues spanning the shoulder and elbow joints post-stroke, we repeated the ANOVA on the sampled hand force data from the 30°/s and 90°/s trials after subtracting values obtained during the 6°/s trials (i.e. trials wherein velocity-dependent stretch reflex activity—but not viscoelastic resistance—should have been minimal; [41, 44]. We obtained similar results and identical statistical conclusions from this supplemental analysis (results not shown). Thus, velocity-dependent responses measured during and shortly after movement were not solely due to passive tissue viscoelasticity but rather implicated the presence of abnormal stretch reflexes post-stroke.
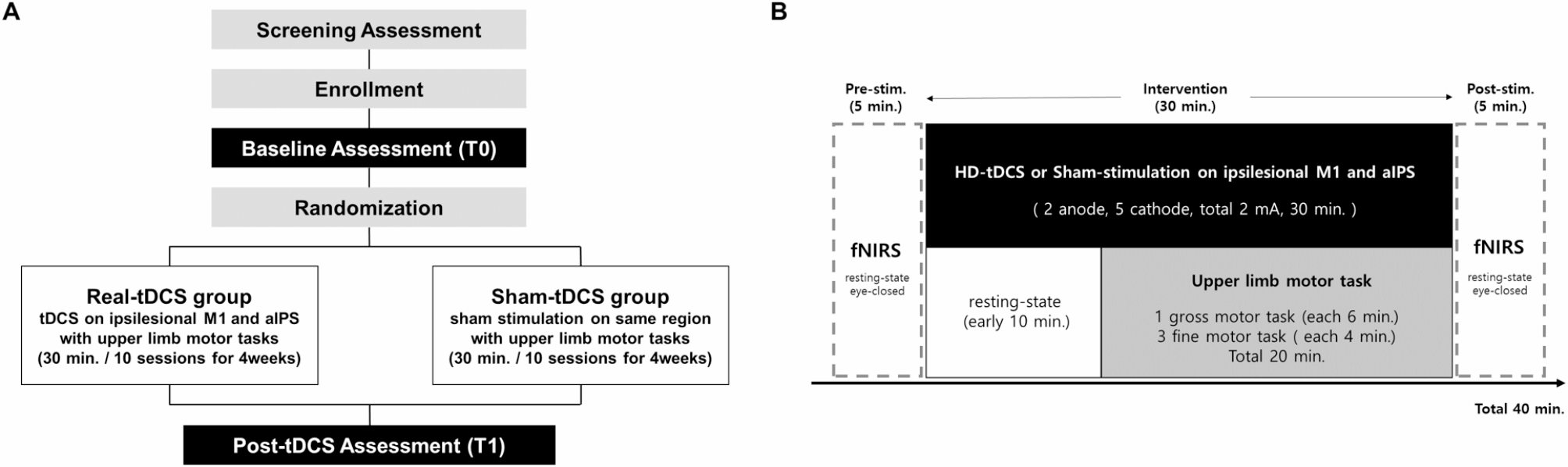
Figure 4 plots change in hand force magnitude relative to steady-state averaged across target locations, movement directions, and days. The three-way interaction between subject group, sampling window and movement speed can readily be seen in that hand forces differed across groups, transport speeds, and sampling times during and shortly after transport but not later in the holding period. To determine the earliest point in time beyond which hand force ceased to be movement velocity-dependent, we performed a post-hoc series of eight separate two-way, mixed-model, general linear model, repeated measures ANOVA to determine how changes in hand force magnitude varied by subject group and movement speed for each of the eight sampling times (PeakVel, EOT, and EOT plus 1, 2, 3, 5, 10 and 15 s). In contrast to the first three sampling times, wherein the main effect of movement speed was either significant (PeakVel: F(2,38) = 70.58, p < 0.0005; EOT: F(2,38) = 21.14, p < 0.0005) or marginally significant (EOT + 1 s: F(2,38) = 2.76, p = 0.085), the main effect of movement speed was absent at EOT + 2 s (F(2,38) = 0.91, p = 0.417) and at all subsequent time points. As shown by the vertical dashed lines in Fig. 2A, arm movement had completely ceased prior to EOT + 2 s (i.e. there was no acceleration or velocity component associated with EOT + 2 s for any movement speed). The interaction between movement speed and subject group was significant only during movement (PeakVel: F(2,38) = 8.44, p < 0.002); no interactions were found at later times. A set of one-sided t-tests revealed that hand force magnitude post-stroke did not differ from asymptotic values from EOT + 2 s onwards. Thus, spastic responses (i.e. velocity-dependent resistance to stretch) are most visible in the post-stroke hand in the fastest conditions of limb transport, but only during transport or for a short period thereafter (i.e. less than 2 s after movement ceases).
Fig. 4
Force magnitude as a function of speed, time and subject group (HS: Shaded bars; NI: open bars). Error bars represent ± 1 SEM. The shaded area from EOT + 2 s onwards indicates the sampling intervals in which ANOVA found no effect of movement speed on hand force magnitude. The dashed box identifies the point in time selected for subsequent detailed analysis of hand force and EMG data
Effect of hand position on postural bias forcesBecause hand forces reached velocity-independence and steady-state by EOT + 2 s, we next analyzed the raw hand forces—not relative to asymptote—measured at EOT + 2 s for each subject. Representative data are shown in Fig. 5A, where raw hand force magnitude was averaged across movement speeds and days. Compared to NI subjects who generated negligible tonic forces at the robot's handle throughout the workspace after movement had ceased, each HS subject displayed a unique field of hand forces that varied systematically across their arm’s reachable workspace. Steady-state, posture-dependent hand forces were typically higher at the workspace boundaries in HS subjects. These forces were stronger on one side of the reachable workspace and pointed towards an equilibrium point located in the approximate center of the workspace. These observations were supported by results of a mixed-model, repeated measures ANOVA that examined how hand force magnitude values measured at EOT + 2 s varied as a function of subject group (HS, NI), movement direction (EF, EE, SF, SE), and workspace location (boundary, center). Workspace location demonstrated a strong interaction with subject group (F(1,37) = 51.24, p < 0.0005): hand forces varied strongly depending on whether the location was at or near the boundary or center of the workspace for HS (Fig. 5B) but not for NI subjects. The ANOVA found no evidence supporting a main effect of movement direction or any interaction between this and the other factors (p > 0.301 in all cases). Thus, hand forces measured at EOT + 2 s post-stroke were predominantly position-dependent, having no systematic dependence on movement speed and/or direction.
Fig. 5
A Raw hand force vectors as a function of location throughout the workspace for a representative HS subject (left) and NI subject (right). B Population summary of hand force magnitude as a function of workspace location (boundary vs. center) for HS (grey bars) and NI subjects (open bars) at EOT + 2 s. Error bars represent ± 1 SEM
Elevated hand forces are accompanied by large EMG activations in some hemiparetic arm muscles post-strokeWe next sought to determine whether posture-dependent bias forces post-stroke were due primarily to passive properties of tissues spanning the hemiparetic joints or whether bias forces were at least partly neuromuscular in origin. Figure 6 plots spatial maps of selected EMG activations (normalized to MVIC) at EOT + 2 s for a representative subject from each group. For the selected HS subject, robotic translation of the hand led to elevated levels of EMG activations that were relatively large in some muscles with respect to signals recorded during maximal voluntary isometric contractions (e.g., TRILT, TRILG and BRD). In other muscles, the activations tended to exhibit posture-dependence such that activation was greater when the muscle was lengthened than when shortened (e.g., BICL, PECS). Yet other muscles exhibited negligible activations at EOT + 2 s regardless of limb posture (e.g., BICS, ADL, PDL). These results were characteristic of the study population in the sense that all stroke survivors exhibited high levels of muscle activation throughout the workspace only in some muscles (most notably TRI and PECS), a modest tendency to exhibit posture-dependent activation in a one or two muscles (which varied by individual), and no indication of abnormal “resting” activation in the remaining muscles. By contrast, activation was minimal in all muscles by EOT + 2 s throughout the workspace for all NI subjects (a selected individual's results are shown in Fig. 6B).
Fig. 6
A Contour plots of elbow and shoulder muscle activations (averaged across transition speeds) for a selected HS subject at 2 s after End of Transition. Muscle activation is presented as a function of hand position in the workspace on a scale ranging from 0 to 100% maximum isometric voluntary contraction (color bar on the right). B Contour plots of elbow and shoulder muscles for a selected NI subject at 2 s after End of Transition
These general observations were confirmed with a set of three-way, repeated measures, general linear model ANOVA that examined the extent to which the elbow and shoulder muscle activations varied by subject group and sample time across relevant workspace locations. Results from the elbow analyses (Fig. 7, top) were consistent with our hypothesis that interaction forces induced by passive translation of the hand are partly neuromuscular in origin in that we found a main effect of subject group for BRD (F(1,115) = 8.67; p = 0.010), TRILG (F(1,115) = 12.66; p = 0.003), and BICL (F(1,115) = 6.68; p = 0.020). In each case, the measured muscle activations were a larger percentage of their voluntary maximum capacity throughout the workspace for the HS group as compared to the NI control group. We did not observe a main effect of subject group for BICS or TRILT (F(1,115) < 0.71 and p > 0.411 in both cases). We did however observe an apparent interaction between subject group and target for BRD (F(3,115) = 3.86; p = 0.011) such that for the HS group only, BRD activation was systematically greater when the elbow was extended and that muscle was stretched, vs. when the elbow was flexed and the muscle was shortened. We observed no other two-way interactions for any of the recorded elbow muscles. We also found no main effect related to sample time (F(1,115) < 0.68; p > 0.412 in all cases), or any interaction between sample time and the other two fixed factors (F(1,115) < 0.93; p > 0.336 in all cases), reflecting the fact that the patterns of abnormal EMG seen at EOT + 2 s were also seen at EOT + 20 s.
Fig. 7
Cohort results: analyses of selected muscle activations (as a percentage of MVIC) at EOT + 2 s in the elbow contrast (top) and shoulder contrast (bottom), as described in the text. B1, B3, B4, and B6: selected workspace boundary positions; C2 and C3: selected central positions. Icons below the left panels depict limb configurations for the two boundary targets in each contrast. Grey bars: HS; Open bars: NI. Error bars represent ± 1 SEM
For the shoulder analyses (Fig. 7, bottom), we found no main effect of sample time (F(1,82) < 0.97; p > 0.328 in all cases), and no interaction between sample time and the other two fixed factors (F(1,82) < 0.93; p > 0.338 in all cases). We found a main effect of subject group for PECS (F(1,82) = 4.70; p = 0.046), TRILG (F(1,82) = 11.12; p = 0.004), and BICL (F(1,82) = 10.98; p = 0.004) in that measured muscle activations were a greater percentage of MVIC throughout the workspace for the HS group as compared to the NI control group. We did not observe a main effect of subject group for PDL or ADL (F(1,82) < 3.01 and p > 0.102 in both cases). We did however observe an interaction between subject group and target for BICL (F(2,82) = 24.24; p < 0.0005) such that for the HS group only, BICL activation was greater when the shoulder was extended and that muscle was stretched, vs. when the shoulder was flexed and the muscle was shortened. We observed no other two-way interactions for any of the recorded shoulder muscles.
We examined further the significant interaction effects by calculating for each subject an EMG modulation index as the difference between normalized EOT + 2 s EMG values measured at the target location where the muscles were most flexed vs. where the muscles were most extended (Fig. 8). For BRD (elbow contrast), this meant subtracting normalized EMG values measure at target B4 from those measured at B3. For the two-joint muscle BICL (shoulder contrast), this entailed subtracting values measure at target B6 from those measured at B1. EMG modulation index values were tightly packed around 0% MVIC in the NI control group. By contrast, index values were greater than zero in both the BRD and BICL muscles in the HS group. While a single HS appeared to be an outlier in both cases (BRD: HS09; BICL: HS02) (Fig. 8; open squares), removing these outliers and repeating the ANOVA described above did not impact the pattern of main and interaction effects reported. Thus, we obtained support for the idea that passively stretched muscles held in an elongated vs. shortened state elicit greater involuntary activations after stroke in a subset of tested muscles. Neither modulation index exhibited significant correlation with either FMUE or MAS scores.
Fig. 8
Cohort results: EMG Modulation Index [i.e., the change in normalized EMG values measured across the workspace for the elbow contrast (BRD) and the shoulder contrast (BICL) as described in the text]. Each dot represents the modulation index value obtained from a single subject in either the group of NI control subjects or the group of HS subjects
Comments (0)