
記住我
What is known about the topic?
Dysfunction related to pelvic floor muscles is common among pregnant and postpartum women and can cause symptoms such as urinary incontinence and pelvic organ prolapse, which can severely decrease the well-being of women. The practices for guiding pregnant and postpartum women to physical activity and exercise vary in Finland, and national clinical guidelines on this topic are lacking. Recommendations are also lacking for health care professionals on when to refer pregnant and postpartum women to more individualized pelvic floor muscle assessment and guidance.What does this article add?
This article bridges evidence synthesis and evidence transfer through an umbrella review. It provides recommendations for health care professionals on guiding pregnant and postpartum women. Based on the synthesized evidence, women who already have pelvic floor dysfunction during pregnancy or postpartum should be guided to a physical therapist or other health care professional who specializes in the pelvic floor. This article provides a possibility for international audiences to understand and replicate the process by which Finnish national evidence-based clinical guidelines for nursing are developed. IntroductionPregnancy and childbirth change the bodies of women, and some of the most notable anatomical changes occur in the pelvic area. The progressive increase in volume of the uterus causes a major overload in perineal structures, commonly resulting in muscle trauma, nerve injuries, and connective tissue damage.1,2 Pelvic floor muscles (PFM) support the bladder, vagina, rectum, and lower back.3 Reduced strength and functionality of PFM can cause dysfunction of the PFM, resulting in different common and bothersome symptoms2,4 such as urinary incontinence5 or pelvic organ prolapse (POP).6
Urinary incontinence refers to the unintentional passing of urine,7 with prevalence varying from 30% to 70%.1,5,8,9 Typically, urinary incontinence increases during pregnancy and gradually decreases during the first postpartum year, with prevalence varying from 30% to 58%.9,10 POP refers to the bulging of the uterus, bladder, and/or bowel as a result of impairment of the supporting tissues surrounding the vagina.11 The prevalence of POP in women varies from 3% to 50%,12,13 and it is known that pregnancy and childbirth are risk factors for developing POP.14 The symptoms of POP can severely decrease the quality of life of women,15 and health care professionals working with pregnant and postpartum women need evidence-based knowledge to guide and support women to prevent and care for the symptoms of urinary incontinence and POP.
It is common that the amount of exercise decreases as the pregnancy progresses and only a few pregnant women move as much as recommended.16,17 Physical factors related to pregnancy, such as pain, swelling, or nausea may be the causes of reduced exercise, as well as concerns about pregnancy complications. Moreover, lack of motivation, knowledge, and guidance may be the causes of reduced exercise.18 It is also common that after birth, the amount of exercise may not reach the desired level or return to pre-pregnancy levels.19
In Finland, all pregnant women are entitled to free maternity and child health services during pregnancy and after birth. During pregnancy, there are usually 11–15 visits, mainly not only with public health nurses but also with doctors. The purpose of the visits is to follow up on the growth and development of the fetus and the health of the woman during pregnancy and after birth.20 Public health nurses should provide guidance for pregnant and postpartum women, for example, regarding exercise.
This review was conducted as part of the development of the Finnish national clinical practice guidelines, “Pregnant and postpartum women in health care: justification and guidance for physical activity and exercise,” coordinated by the Nursing Research Foundation (NRF).21 The guidelines coordinated and published by the NRF are evidence-based recommendations mainly for nursing professionals. The process of developing guidelines includes 11 phases. Development of the guidelines starts with receiving and accepting the suggested topic and preparing the work plan (phases 1–3). The next phases are systematic literature search; methodological quality assessment of the included studies; rating the level of evidence based on the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach; formulating the recommendations; and external expert review (phases 4–8). The last phases are publication and dissemination of the guidelines; implementation; and updating the guidelines (phases 9–11).22
The guideline “Pregnant and postpartum women in health care: justification and guidance for physical activity and exercise” includes seven sections. This umbrella review forms the basis of one section of the guideline: “Exercise, guided pelvic floor muscle training and function of the pelvic floor” (see Figure 1).
 Figure 1:
Figure 1: Nursing Research Foundation guideline, “Pregnant and postpartum women in health care: justification and guidance for physical activity and exercise”.
The aim of this umbrella review was to summarize the existing evidence about the effectiveness of exercise interventions on urinary incontinence and POP in pregnant and postpartum women. The aim of the guidelines is to unify the exercise guidance given to pregnant and postpartum women in maternity and child health services in Finland, and to reduce any unwarranted variations in guidance.
Review questions (1) What is the effectiveness of exercise interventions on urinary incontinence in pregnant and postpartum women? (2) What is the effectiveness of exercise interventions on POP in pregnant and postpartum women? MethodsWe conducted an umbrella review to form an overall understanding on the topic of interest and to identify areas for future research.23 We followed the JBI Manual for Evidence Synthesis23 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.24 The protocol produced a priori was registered in PROSPERO (CRD42020191591). After rating the level of evidence, recommendations were formulated by a clinical guideline working group based on the guideline handbook of the NRF.22
Inclusion criteriaReviews were included if they met the following criteria: (i) types of study: systematic review and/or meta-analysis of effectiveness; (ii) population: pregnant and/or postpartum women up to 24 months from birth. According to Romano et al.,25 the postpartum period lasts until 6 months after birth, but in this review, the time frame was set at 24 months so that the long-term effectiveness of the interventions could be identified; (iii) interventions: any type of physical activity (e.g. exercise, physiotherapy) or guidance to address the symptoms of UI and/or POP, delivered individually, in a group, face-to-face, or online; (iv) comparison: usual care, no exercise, or being on a waiting list; (v) outcomes: symptoms of urinary incontinence and/or POP; and (vi) language: English or Finnish, as there was no funding for translations.
Search strategy and data sourcesSearches were conducted in MEDLINE (PubMed), CINAHL (EBSCOhost), PsycINFO (EBSCOhost), Web of Science, Medic, Cochrane Library, ERIC (EBSCOhost), Embase, and Academic Search Premier (EBSCOhost) on 3 January 2022. A search update was conducted on 11 January 2023. The search strategy followed the PICO model.26 Detailed search strategies are available in Appendix I, https://links.lww.com/IJEBH/A138. The search was conducted with the assistance of an information specialist.
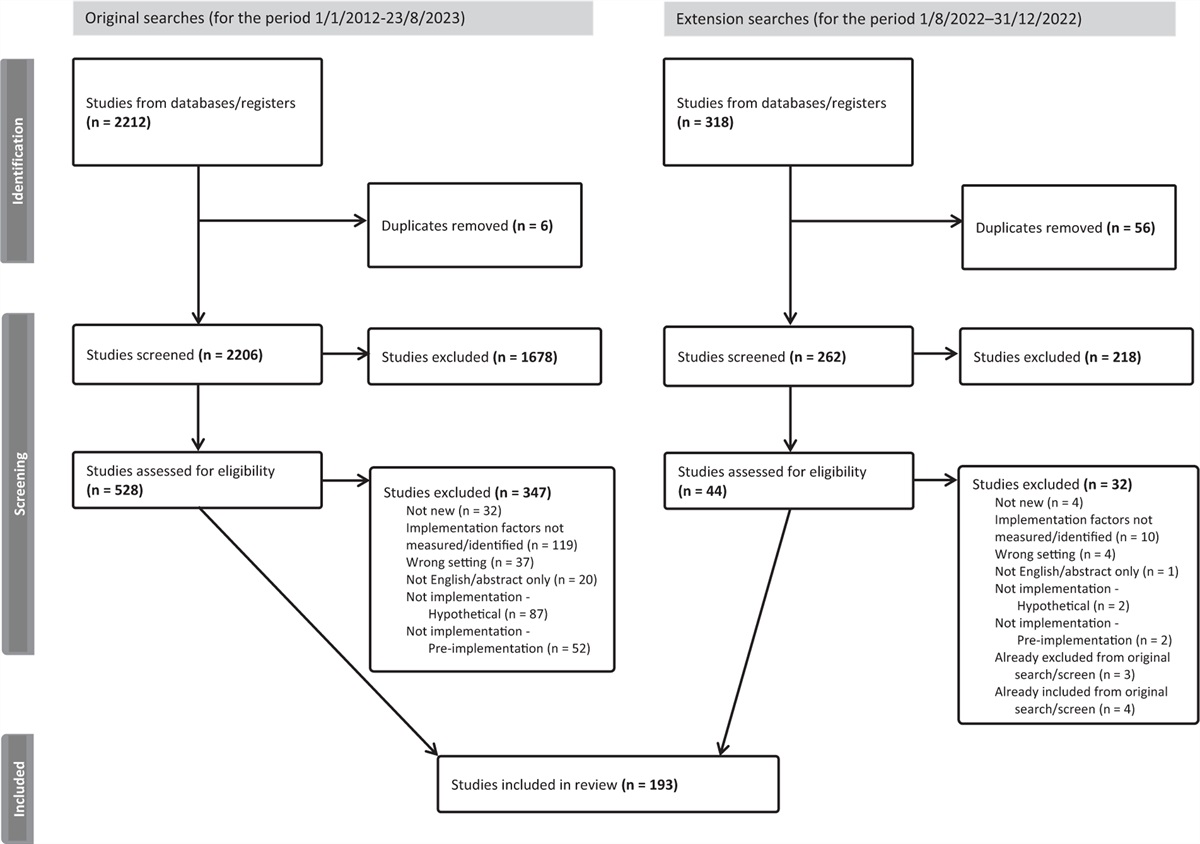
Screening and selectionFirst, two authors (IR, LH) independently screened the titles and abstracts by applying the established eligibility criteria, and after that, any conflicts were discussed to reach consensus. The full texts were screened similarly. The decisions in all phases were recorded using Covidence software (Veritas Health Innovation, Melbourne, Australia). The study selection process is described in a PRISMA flowchart (see Figure 2).
 Figure 2:
Figure 2: PRISMA flow chart of screening process.
Critical appraisalTwo authors (IR, LH) independently performed the methodological quality assessment of the reviews using the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses.27 If the information was not available or was unclearly stated, authors contacted the corresponding authors of these articles. Disagreements over assessments were resolved through discussion. The checklist consists of 11 items (see Table 1) with 4 possible responses: Yes (the criterion is clearly identifiable and assigned 1 point), No (the criterion failed to be applied appropriately), Unclear (the criterion is not clearly identified in the report), and Not applicable. It was determined a priori that the overall scores of a review needed to be at least 6/11 to be included in this umbrella review. Moreover, Item 5: Critical appraisal of studies, needed to have a Yes answer. This was done to ensure the quality of the included reviews.22
Data extraction and analysisTwo authors (IR, LH) independently carried out the data extraction according to JBI's instructions,23 using Covidence. The data extraction table was tested before its actual use. The analysis of the included reviews was done narratively. The summaries of findings from the included reviews were presented in a table.
Grading the level of evidence and forming the recommendationsIf the GRADE assessments were already done by the authors of the included reviews, the same gradings were used. If the GRADE ratings varied for different reviews, the methodological quality ratings of the reviews, publication year, and clinical relevance of the results were considered (emphasis was placed on the most recent, highest quality systematic reviews and clinical relevance). Regarding the level of evidence and the wording of the recommendations, the NRF guideline handbook was followed. The level of evidence is interpreted as follows: A = high, B = moderate, C = low, and D = very low.22
Results Study inclusionAfter duplicates (n = 342) were removed, 391 titles and abstracts were screened. After excluding irrelevant records (n = 359), 32 full-text articles were assessed for eligibility, following which a further 19 articles were excluded. Consequently, 13 articles were included for the methodological quality assessment; however, 4 were excluded because of poor quality. As a result, 9 articles were included in the umbrella review, forming the basis of the recommendations (see Figure 2). The list of excluded studies is available from the authors upon request.
Methodological qualityThe methodological quality of the reviews was assessed using JBI's Critical Appraisal Checklist for Systematic Reviews and Research Syntheses.27 Four studies scored the maximum 11/11 points7,28–30 (see Table 1).
Table 1 - Methodological quality of included reviews Itemsa Review (n = 9) 1 2 3 4 5 6 7 8 9 10 11 Points von Aarburg et al., 202131 Yes No Yes Yes Yes Yes Yes Yes No Yes Yes 9/11 Davenport et al., 201828 Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes 11/11 Harvey, 200332 No No No Yes Yes No Yes Yes No Yes Yes 6/11 Lemos et al., 200833 Yes Yes Yes Yes Yes Yes No Yes No Yes Yes 9/11 Mørkved and Bø, 201434 Yes Yes Yes Yes Yes Yes No Yes No Yes Yes 9/11 Wagg and Bunn, 200735 No No No Yes Yes Yes Yes Yes No Yes Yes 7/11 Woodley et al., 20207 Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes 11/11 Wu et al., 201829 Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes 11/11 Yang et al., 202230 Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes 11/11 aItems from the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses27:1. Is the review question clearly and explicitly stated?2. Were the inclusion criteria appropriate for the review question?3. Was the search strategy appropriate?4. Were the sources and resources used to search for studies adequate?5. Were the criteria for appraising studies appropriate?6. Was critical appraisal conducted by 2 or more reviewers independently?7. Were there methods to minimize errors in data extraction?8. Were the methods used to combine studies appropriate?9. Was the likelihood of publication bias assessed?10. Were recommendations for policy and/or practice supported by the reported data?11. Were the specific directives for new research appropriate?The 9 included reviews, consisting of 89 original studies, were published between 2003 and 2022 (see Appendix II, https://links.lww.com/IJEBH/A139 for a list of original studies). All were systematic reviews, of which 4 were meta-analyses, 2 were narrative analyses, and 3 were both meta-analyses and narrative analyses. The main purpose of the reviews was to assess the effectiveness of exercise interventions in pregnant (n = 2), postpartum (n = 2), or both pregnant and postpartum women (n = 5). Primary outcomes assessed were urinary incontinence (n = 8) and POP (n = 1) (see Table 2).
Table 2 - Characteristics of included reviews (n = 9) and interventions Primary outcome UI (n = 8) Review, year (country) Primary outcome Interventions used Total number/sample size, participants Number of original studies in review Methodological quality, appraisal tool Method of analysis von Aarburg et al., 202131 (Switzerland) Incidence of UI F: not reportedF, frequency; FI, fecal incontinence; GW, gestational week; I, intensity; PFMT, pelvic floor muscle training; POP, pelvic organ prolapse; QoL, quality of life; RCT, randomized controlled trial; S, setting; T, time; Ty, type; UI, urinary incontinence.
The interventions and the degree of description of the interventions in the reviews were heterogeneous. The exercise protocols varied from solely pelvic floor muscle training (PFMT)29,30,33–35 to combinations of aerobic exercise and PFMT.28,32 In 2 reviews, the exercise interventions included various sports, for example, strength training, stretching, or aerobic exercise.7,31 The exercise interventions were initiated independently and/or in groups; and/or under supervision of a physiotherapist, midwife, nurse, or other qualified person; in hospitals, exercise classes, or at home. The frequency of exercise varied from several times a day to once a week and the duration of the intervention was from 4 weeks to 17 months. The interventions began between gestational week 9 and 12 months postpartum. The interventions were described according to FITT principles (frequency, intensity, time, type).36 In addition, the setting of the intervention was added (see Table 2).
Summary of findings Exercise and pelvic floor muscle training during pregnancy and urinary incontinence risk and symptoms during pregnancyA meta-analysis including 15 randomized controlled trials (RCTs) (n = 2764 women) found a 50% reduction in the odds of developing urinary incontinence during pregnancy between the women in the exercise intervention group and women in the control group [odds ratio (OR) 0.50, 95% confidence interval (CI) 0.37–0.68, I2 = 60%].28 Another meta-analysis of 11 RCTs (n = 3307 women) found that exercise and PFMT for mixed prevention and treatment of urinary incontinence during pregnancy decreases urinary incontinence risk in late pregnancy compared with women in the control group [risk ratio (RR) 0.78, 95% CI 0.64–0.94, I2 = 79%).7 In contrast, a meta-analysis of 3 observational studies (n = 960 women) found no statistically significant association between physical activity and urinary incontinence during pregnancy (OR 0.90, 95% CI 0.69–1.18, p = 0.45, I2 = 0%).31
Exercise during pregnancy and severity of urinary incontinence symptoms during pregnancyA meta-analysis including 5 RCTs (n = 465 women) showed a moderate reduction in the severity of the symptoms of urinary incontinence during pregnancy between the exercise intervention group and control group (SMD −0.54, 95% CI −0.88 to −0.20, I2 = 64%).28
Exercise and pelvic floor muscle training during pregnancy and the risk and reduction of postpartum urinary incontinence symptomsTwo meta-analyses found that exercise during pregnancy decreased the risk of developing postpartum urinary incontinence (OR 0.63, 95% CI 0.51–0.79, I2 = 0%)28 (OR 0.45, 95% CI 0.31–0.66, p < 0,0001, I2 = 7%).33 Women performing PFMT during pregnancy for prevention (RR 0.38, 95% CI 0.17–0.83, I2 = 74%)7 and for mixed prevention and treatment (RR 0.83, 95% CI 0.71–0.99, I2 = 0%)7 of postpartum urinary incontinence were less likely to report symptoms of urinary incontinence in early postpartum (6 weeks to 3 months postpartum). In addition, PFMT during pregnancy may reduce the risk of urinary incontinence in mid-postpartum (>3 to 6 months postpartum) (RR 0.71, 95% CI 0.54–0.95, I2 = 0%)7 (RR 0.75, 95% CI 0.56–1.02, p = 0.028)32 (RR 0.73, 95% CI 0.55–0.97, I2 = 65%).7 In contrast, in late postpartum (>6 to 12 months postpartum) (RR 0.85, 95% CI 0.63–1.14, I2 = 0%),7 12 months postpartum (RR 1.20, 95% CI 0.65–2.21),7 and in the long-term (>5 years) (RR 1.07, 95% CI 0.77–1.48, I2 = 25%)7, there was no evidence of a difference between women in the intervention group and the control group in terms of risk in the prevalence of urinary incontinence. A narrative analysis systematic review of 22 studies (n = 3731 women) found that exercise interventions during pregnancy showed a significant reduction in symptoms, episodes of urinary incontinence, or a lower percentage of women with urinary incontinence in late pregnancy or during the first 3 months after birth.34
Exercise during pregnancy and severity of postpartum urinary incontinence symptomsA meta-analysis including 3 RCTs (n = 284 women) found that exercise and PFMT during pregnancy played a moderate role in reducing the severity of postpartum urinary incontinence symptoms (SMD −0.54, 95% CI −0.87 to −0.22, I2 = 24%).28
Pelvic floor muscle training during pregnancy and prevention of symptoms of urinary incontinence during pregnancyContinent women performing PFMT during pregnancy had a lower risk of reporting urinary incontinence in late pregnancy (62% less, RR 0.38, 95% CI 0.20–0.72, I2 = 78%).7
Group pelvic floor muscle training during pregnancy and prevalence of urinary incontinence during pregnancy or postpartumGroup PFMT during pregnancy significantly reduced the prevalence of urinary incontinence during pregnancy (RR 0.67, 95% CI 0.57–0.80, p < 0.00001, I2 = 0%)30 and postpartum urinary incontinence (RR 0.66, 95% CI 0.52–0.84, p = 0.0008, I2 = 0%).30
Pelvic floor muscle training during pregnancy and treatment and risk of urinary incontinence during late pregnancy and postpartumPFMT for the treatment of urinary incontinence during pregnancy was not effective and there was no evidence of any difference in the risk of urinary incontinence in late pregnancy (RR 0.70, 95% CI 0.44–1.13, I2 = 71%),7 in early postpartum (RR 0.75, 95% CI 0.37–1.53, I2 = 65%),7 in mid-postpartum (RR 0.94, 95% CI 0.70–1.24, I2 = 65%),7 or in late postpartum (RR 0.50, 95% CI 0.13–1.93, I2 = 94%).7
Exercise and pelvic floor muscle training postpartum and risk and symptoms of postpartum urinary incontinenceA meta-analysis including 2 observational studies (n = 742 women) found that there was no statistically significant association between postpartum physical activity and postpartum urinary incontinence (OR 1.31, 95% CI 0.74–2.34, p = 0.35, I2 = 42%).31 A meta-analysis including 2 RCTs (n = 321 women) found that women performing PFMT were 46% less likely to report urinary incontinence in early postpartum (RR 0.54, 95% CI 0.44–0.66, I2 = 0%),7 but no evidence of a difference in the risk of urinary incontinence in women randomized to PFMT or control group in mid-postpartum (RR 0.95, 95% CI 0.75–1.19, I2 = 65%),7 in late postpartum (RR 0.88, 95% CI 0.71–1.09, I2 = 50%),7 6 years postpartum (RR 0.96, 95% CI 0.88–1.05),7 or 12 years postpartum were found (RR 1.03, 95% CI 0.94–1.12).7 However, 1 meta-analysis including 7 RCTs (n = 2692 women) found that women performing PFMT showed a significant reduction in urinary incontinence still 12 months postpartum (RR, 0.44, 95% CI 0.25–0.75, I2 = 91%).29
Pelvic floor muscle training postpartum and treatment of symptoms of POP postpartumA meta-analysis including 3 RCTs (n = 609 women) found that structured PFMT compared with watchful waiting showed a reduction in vaginal bulging in late postpartum (RR, 0.48, 95% CI 0.30 to 0.76, I2 = 47%).29 A meta-analysis including 6 RCTs (n = 1275 women) showed there may be a reduction of stage II or greater POP within 12 months postpartum (RR 0.74, 95% CI 0.45 to 1.24, I2 = 47%).29
Recommendations for clinical practiceBased on the summary of findings of this review, the recommendations were formulated by a clinical guideline working group (see Table 3). The NRF guideline handbook was followed in terms of the level of evidence and the wording of the recommendations.22
 Table 3:
Table 3: Recommendations for clinical practice and summary of findings

留言 (0)