
Remember me





What is known about the topic?
Post-operative pain in the ICU is multifactorial and has a high prevalence. Pain management should include the use of validated tools for multimodal assessment and analgesia. Nurses are the health care professionals who most frequently assess pain, as well as evaluating the patient's response to pain management treatment and monitoring for the occurrence of adverse events. Therefore, they must be up to date and trained on best practices in pain management.What does this paper add?
Despite advances in care, few studies have focused on management that incorporates best practices. The use of multimodal analgesia for pain management in ICU patients is challenging for the nursing team. Positive results were recorded with the use of educational strategies to raise awareness and change behavior of the nursing team regarding pain management. INTRODUCTIONThe International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated, or similar to that associated, with actual or potential tissue damage."1 Post-operative pain is the most prevalent type of acute pain. It is reported that 80% of surgical patients experience post-operative pain, and the frequency and intensity are greatest from the first to the fourth post-operative day. In this sense, post-operative pain management should be a priority in the care of these patients. When pain is not properly controlled, the patient becomes predisposed to chronic post-operative pain, which can have a significant impact on quality of life.2
About one-third of post-operative patients are admitted to surgical intensive care units after an elective or emergency surgical procedure. For many years, mortality or survival rates dominated outcome measures for critical care. Recently, with a shift in focus to patient-centered care, together with the use of international accreditation recommendations, measures such as pain assessment and pain management have become equally relevant.3,4 Furthermore, pain seriously affects a patient's quality of life and can interfere with the recovery of functional capacity.5
Unrelieved post-operative pain can reduce patient mobility, resulting in complications such as deep vein thrombosis, pulmonary embolism, or pneumonia. In addition, post-surgical complications related to inadequate pain management affect hospital performance due to long periods of hospitalization and readmissions, which increase the cost of treatment.6
Improving the quality of health care refers to obtaining better results through changes to practice, incorporating technical elements that can be standardized in each context. Therefore, pain quality indicators play an important role in assessing the structure, process, and results of care provided to patients in pain. Structure refers to the setting in which the care takes place and involves structural and organizational characteristics. Process represents what is actually done during the provision of this care, while the results refer to the effects of care in improving pain and optimizing practice.
Nurses are the health team professionals who evaluate pain most frequently, as well as assessing the therapeutic response to treatment and monitoring for the occurrence of adverse events. Among their various roles, they assist with determining the pain management treatment and propose non-pharmacological strategies. They prepare the patient for treatment, involving the caregivers as well, from the moment of admission to hospital discharge. From a managerial point of view, adequate pain management reflects the quality of care, and its monitoring is recommended by national and international accrediting institutions.
Despite advances in care, few studies have focused on management that considers the implementation of improvements.7,8 The best practice recommendations used in this project were based on a JBI evidence summary on post-operative pain management, as well as evidence from two systematic reviews with a meta-analysis, three clinical guidelines, and two expert opinion papers.9 These recommendations emphasize patient education; individual treatment goals and plans; patient assessment for comorbidities, history of chronic pain, substance abuse, and previous post-operative management regimen; use of a validated tool to assess pain; and use of multimodal analgesia for pain control. This should include the use of various analgesic medications combined with non-pharmacological interventions. Patients receiving systemic opioids should be monitored for sedation, and institutional policies and procedures should guide the management of pain after surgery.
The implementation project was undertaken at the ICU in a reference center in Brazil for medium- and high-complexity surgical treatment for orthopedic diseases, trauma, and the rehabilitation of associated musculoskeletal pathologies. Highly complex surgeries account for 40% of the total surgeries, and the post-operative period is performed in the ICU. The center has a total of 314 beds, with 16 ICU beds. The center also has an interdisciplinary team specializing in pain management, which assesses patients in different wards of the hospital. In cases of chronic pain, the hospital has a structured outpatient program for the management of these patients.10
Therefore, post-operative pain management was selected as the topic of this study, as pain control is always a challenge for the ICU nursing team, delaying hospital discharge, and leaving the patient more susceptible to risks and the occurrence of adverse events.
OBJECTIVESThe main objective was to improve post-operative pain management by nurses in an ICU. The specific objectives were to:
1. Conduct a baseline audit to determine compliance with best practice recommendations in post-operative pain management performed by nurses in an intensive care unit. 2. Identify barriers and enablers to improving compliance and develop strategies to address areas of non-compliance. 3. Conduct a follow-up audit to assess the extent of improved compliance with recommendations and identify strategies to sustain and further improve post-operative pain management outcomes. METHODSThe project is based on the JBI evidence implementation approach, which provided both a theoretical and a practical framework for the project.11 The JBI implementation approach is grounded in the audit and feedback process along with a structured approach to the identification and management of barriers and enablers to compliance with recommended clinical practices. The JBI approach occurs in seven stages: (1) identification of practice area for change, (2) engaging change agents, (3) assessment of context and readiness to change, (4) review of practice against evidence-based audit criteria, (5) implementation of changes to practice, (6) re-assessment of practice using a follow-up audit, and (7) consideration of the sustainability of practice changes. The seven stages occur within three phases: (1) planning, (2) baseline assessment and implementation, and (3) impact evaluation and sustainability.
For the selected topic, audit criteria were developed based on a JBI evidence summary.9 The audit criteria were accessed via PACES, based on the best scientific evidence available in the literature. Compliance with best practices by nurses in the ICU was assessed according to these criteria. The GRIP tool was used to document the barriers encountered and the strategies and resources needed to overcome them. The project was conducted over 8 months.
Phase 1: Implementation planning Stage 1: Identification of practice area for changeIn the first phase of the project, stakeholders were identified as well as relevant participants for the project team. At a technical visit, the project was presented to local leaders, comprising the ICU nursing coordination team and the pain clinic nursing coordination team. For the execution of the project, an improvement team was formed, composed of six people: a teaching nurse (project coordinator); a pain service coordinating nurse (team leader); three clinical nurses from the Pain Clinic (collection of data for baseline and follow-up audits); and a routine ICU nurse (collection of data for baseline and follow-up audits).
Stage 2: Engaging change agentsAt this stage of the project, the change agents were considered, which included the nursing team working in post-operative orthopedic care in the ICU in addition to the individuals mentioned above. In order to carry out safe and well-structured change that can be maintained in the organization, it is necessary to involve professionals who will motivate and lead the team. The ICU has a routine nurse, who was a reference for the ICU nursing team. This nurse was chosen to be the agent of change, together with the nurses at the Pain Clinic.
Stage 3: Assessment of context and readiness to changeA technical visit was carried out at the adult ICU for patients during the orthopedic post-operative period. The purpose of the visist was to meet the nursing team and its leaders, learn about routines and policies that guide pain management within the institution, and identify indicators for monitoring compliance in pain assessment. This allowed the team to become familar with the project setting, the existing processes, and the factors that could influence the proposed changes.
In the meeting with the team and its leaders, we conducted a situational diagnosis of how pain management was carried out, the strengths and weaknesses of the nursing team in this context, and opportunities for improvement. This provided detailed insights into the context in which the pain management process took place at the ICU.
Phase 2: Baseline assessment and implementation Stage 4: Review of practice against evidence-based criteria (baseline audit)The audit criteria selected for the project were extracted from the PACES program, based on the JBI evidence summary entitled “Post-surgery (adults) best practices: Acute pain management general principles (2020).”9Table 1 presents the audit criteria, sample, and measurement method. The team collected data for the baseline audit during April 2021. To gather data for Criteria 1 to 8, the team analyzed printed and electronic medical records. The service was in the process of transitioning to electronic medical records; therefore, it still used printed medical records as an inclusion criterion. To ensure that there would be pain records, it was determined that patients should be in ICU for at least 24 hours.
Table 1 - Audit criteria, sample, and measurement method Method used to measure compliance with best practice Audit criterion Sample Item of the medical record to be audited Response 1. Patients receive individually tailored pre-operative education about the management of post-operative pain. Baseline audit = 30 medical recordsThe results obtained in the baseline audit were discussed with the project improvement team. A brainstorming technique was used by listening to all opinions to discuss strategies to implement the best practices. The meetings took place through the Google Meeting platform and on-site. The GRiP matrix was used to identify barriers, define strategies and resources to address them, and evaluate the results obtained. The period from designing the matrix to implementing the strategies took place over 24 weeks, from May to October, 2021.
Phase 3: Impact evaluation and sustainability Stage 6: Follow-up audit of change strategiesThe follow-up audit used the same sample size, audit criteria, and data collection strategies as the baseline audit. The purpose of the follow-up audit was to assess the impact of the strategies on improving compliance. During this audit, which took place in December 2021, the team monitored staff adherence to recommended practices.
Stage 7: Considering sustainability of the projectSubsequent audits will be performed as recommended in the JBI Implementation Manual and plotted on a trend chart.
ETHICSThe project was approved by the Ethics and Research Committee of the National Institute of Orthopedics and Traumatology, CAAE number: 03179118.4.0000.5243. The standards for research involving human beings were followed, as established by Resolution 466/12 of the National Health Council of Brazil.
ANALYSISThe audits were carried out using an instrument developed in Google Forms, and the data were subsequently entered into an Excel spreadsheet. To assess changes in compliance, data were uploaded into the PACES software to derive descriptive statistics in the form of percentages.
RESULTS Baseline auditIn the baseline audit, we analyzed 30 medical records of ICU patients who were in the post-operative period (see Table 2). This process was used to measure compliance with Criteria 1 to 8. The sample had a median age of 65 years for both genders. Patients classified according to specialized care centers depending on the area being operated on. The most prevalent surgery was hip surgery (26.7%), spine surgery (23.3%), and trauma (23.3%). Most patients were in the post-operative period of hip arthroplasty (20%). The length of stay in the ICU had a median of 11.5 days.
Table 2 - Demographic profile of patients in the baseline audit and follow-up audit Baseline audit Follow-up audit Variable n (%) Variable n (%) Gender Gender Female 15 (50) Female 19 (63.3) Male 15 (50) Male 11 (36.7) NIOT Specialized Care Center NIOT Specialized Care Center Spine surgery 7 (23.3) Spine surgery 7 (23.4) Knee surgery 6 (20.0) Maxillofacial surgery 1 (3.3) Hip surgery 8 (26.7) Knee surgery 6 (20.0) Trauma 7 (23.3) Hip surgery 6 (20.0) Tumor 2 (6.7) Shoulder surgery 1 (3.3) Foot surgery 1 (3.3) Trauma 8 (26.7) Type of surgery performed Type of surgery performed Hip arthroplasty 6 (20.0) Amputation 1 (3.3) Femur fracture repair 2 (6.7) Knee arthroplasty 4 (13.4) Thoracic scapular disarticulation 1 (3.3) Hip arthroplasty 3 (10.0) Osteosynthesis 3 (10.0) Spine arthrodesis 6 (20.1) Tumor resection 1 (3.3) Rotator cuff repair 1 (3.3) Knee arthroplasty review 2 (6.7) Osteosynthesis 9 (30.0) Hip arthroplasty review 3 (10.0) Jaw reconstruction surgery 1 (3.3) Spine arthrodesis 3 (10.0) Arthrodesis review 1 (3.3) Knee arthroplasty 4 (13.4) Knee arthroplasty review 1 (3.3) Hip arthroplasty 6 (20.0) Hip arthroplasty review 3 (10.0) Median (dp) Median (dp) Days of stay in the ICU 11.5 (91.7) Days of stay in the ICU 10 (140.9) Age (years) 65 (17.52) Age (years) 70 (20.0)NIOT, National Institute of Orthopedics and Traumatology.
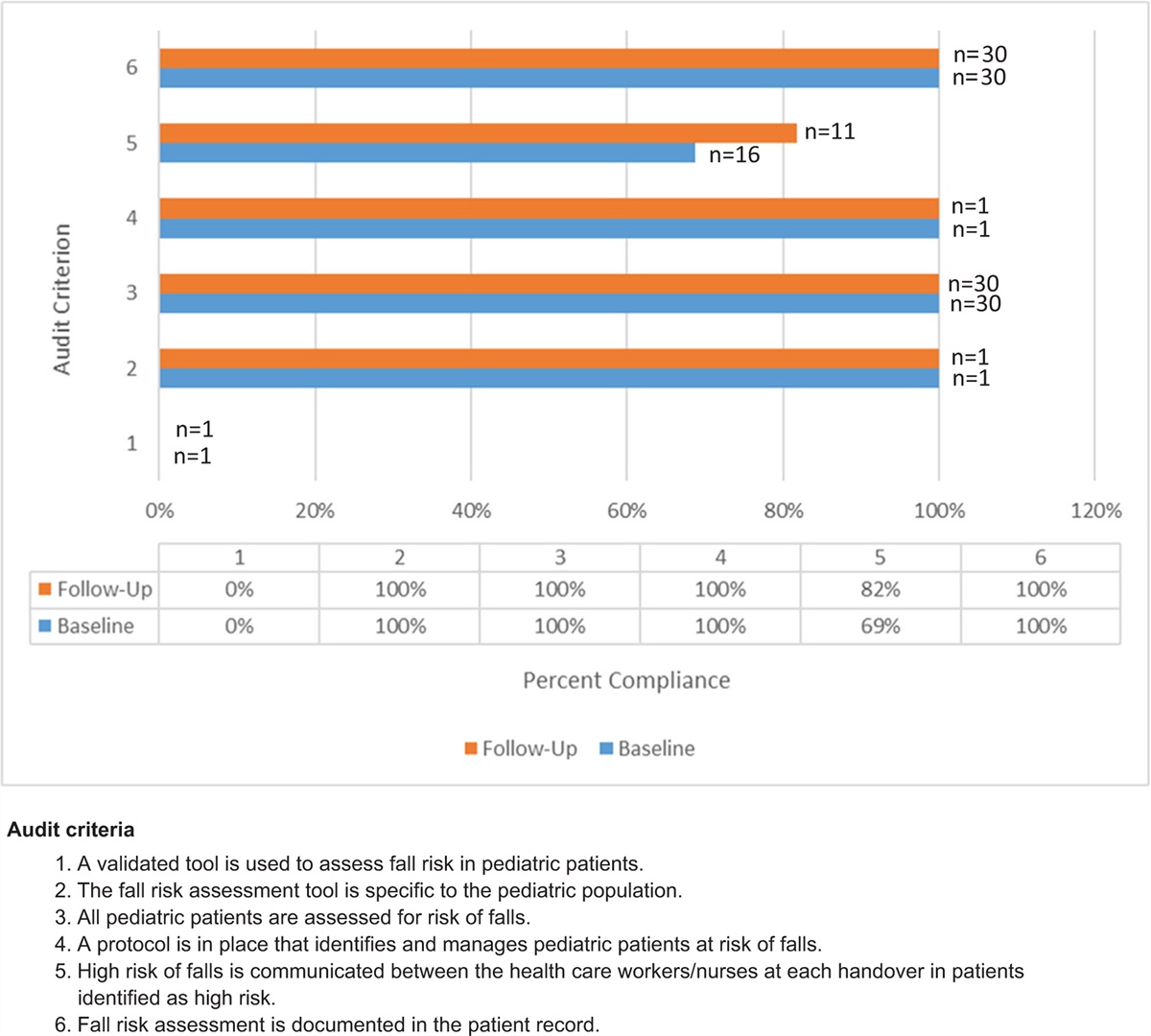
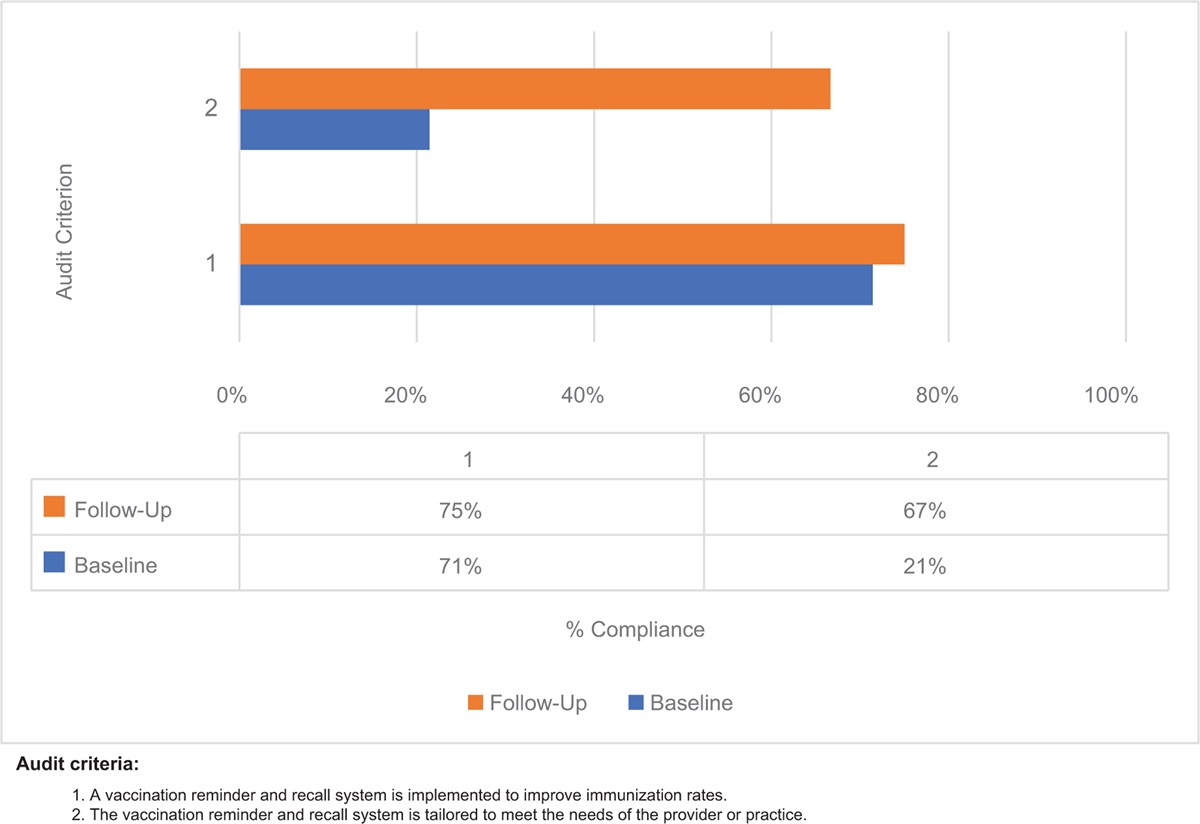
The percentage of compliance in the baseline audit is shown in Figure 1. Of the eight criteria, only Criteria 2, 4, and 5 showed 100% compliance, indicating that patients were evaluated pre-operatively to guide the management of post-operative pain (Criterion 2). The ICU already had a protocol for pain management (Criterion 4) and used a validated tool for pain assessment (Criterion 5). Criterion 1 showed good compliance (96.67%), indicating that only one patient did not receive pre-operative education. Criteria 3 (0%) and 6 (23.33%) showed low compliance, indicating that few patients had documented plans and goals, and had received multimodal analgesia in the ICU. Criteria 7 and 8 showed compliance of 60% and 50%, respectively.
 Figure 1:
Figure 1: Compliance (%) with best practice for post-operative pain management in the ICU at baseline audit compared with follow-up audit.
Implementation of strategies to improve practiceWhen analyzing the results of the baseline audit, the improvement team decided on actions that initially prioritized Criteria 3 to 8, as Criteria 1 and 2 would involve other areas of the hospital. The GRiP matrix was used to identify four barriers (Table 3).
Table 3 - Getting Research into Practice (GRiP) analysis Barrier Strategies Resources Outcomes 1. Lack of knowledge of nurses in the management of post-operative pain. Training workshop to enhance knowledge on pain management. Explanatory talk and case discussions. All nurses trained and proposal made of an improvement plan. Implementation of non-pharmacological interventions. 2. Insufficient record of pain in medical records. Standardize pain records and create a recording form. Meetings in the workplace and remotely. Specific form for recording pain in the ICU. 3. Absence of decision-making flowchart and specific actions for pain management in the ICU. Construct a flowchart according to severity and intensity of pain. Meetings in the workplace and remotely. Creation of a flowchart and definition of professional conduct. 4. Lack of awareness among professionals about the importance of pain management. Pain control awareness campaign called “NIOT without pain SEM DOR.” Informative pamphlet / computer screen saver / videos / conversation cycle. Professional awareness.NIOT, National Institute of Orthopedics and Traumatology.
Barrier 1. The first barrier related to ICU nurses’ knowledge of pain management. A workshop was conducted in a Google Classroom. The nurses registered through a link, and later received access to the classroom via e-mail. All 32 nurses took part in the training. The workshop addressed the following topics: best practices in post-operative pain in the ICU; nursing care in the IntegraDOR program; patient safety in pain management in the ICU; non-pharmacological therapies for patients in the post-operative period in the ICU; and integrative and complementary practices in health care. Each team member was responsible for a class, which was previously recorded for the nurses to watch in their free time. The ICU nursing coordination recorded a welcome video that was made available at the beginning of the workshop. In the end, an improvement plan was drawn up, which was built and placed in the 5W2H tool format, containing future actions to be developed.
Barrier 2. The second barrier was related to recording pain. The health care professionals only recorded pain intensity on the ICU fluid balance sheet. The need for a specific form for recording pain was identified. The project team created this form with additional space to specify the pain scale used, pain intensity, pain location, and pain characteristics, as well as the assessment of sedation and delirium in the ICU. This instrument is in the testing phase, awaiting approval by the team.
Barrier 3. Although the hospital had a protocol for pain management, there was a need for a specific flowchart to guide the decision-making of the health care professionals. The team developed a flowchart that started with assessing the level of consciousness of the patient admitted to ICU. Based on this assessment, the flowchart specified the use of the most appropriate pain assessment tool. The next steps were based on the results of the assessment scale.
Barrier 4. The health care professionals’ lack of awareness about the importance of pain management was the fourth barrier. The team launched a campaign, with the creation of educational pamphlets distributed in the unit, in addition to videos that were shown as screen savers on the ICU computers. An email was sent to the entire team and messages were disseminated via loudspeakers, directing the health care professionals’ attention to adequate pain management. On October 17, 2021, actions were intensified in acknowledgement of World Pain Day, a date created by the International Association for the Study of Pain, and supported by the World Health Organization.
Follow-up auditIn the follow-up audit, 30 patient records were analyzed. The sample was predominantly female (63.3%), with a median age of 70 years. Patients were monitored by a specialized care center for follow-up, with a higher prevalence of trauma (26.7%) and spinal (23.4%) surgeries. Most patients were undergoing post-operative osteosynthesis (30.0%) and spine arthrodesis (20.1%). The length of stay in the ICU had a median of 10 days (see Table 2).
Figure 1 presents the percentage of compliance in the baseline and follow-up audits. The follow-up audit sample showed that there was no improvement for Criteria 1 and 2. Because of the COVID-19 pandemic, it was not possible to intervene specifically in these criteria since it would affect other sectors of the hospital. Criterion 3 increased from 0% to 20%. Criteria 4 and 5 maintained 100% compliance. Criteria 6, 7, and 8 showed an increase in compliance of 30%, 22.8%, and 50%, respectively.
DISCUSSIONQuality improvement in pain management depends on the knowledge, experience, and training of ICU nurses.4,12 It is necessary to seek strategies to maximize patient comfort and optimize pain relief.13 In ICU, post-operative pain is common, with many underlying causes. Nurses are the health care professionals who attend to these patients at the bedside; therefore, the pain management performed by these professionals reflects the quality of care provided.7,14
This project successfully optimized pain management in the ICU. Education was used as the main strategy. A workshop on best practices in post-operative pain management was held for all ICU nurses. As a result, non-pharmacological interventions performed by nurses, a work flowchart, improved pain recording, monitoring of adverse events to opioids, and the referral of patients to the pain unit were implemented.
The follow-up audit showed improved compliance for four audited items and maintenance of 100% compliance for two items. Education as an intervention strategy to improve post-operative pain management was successfully reported in another improvement project, with the results showing a decreased percentage of patients with tolerance to opioids and reduced length of stay in hospital.15
Due to the COVID-19 pandemic, the workshop was held virtually, and at first, there were concerns about low participation. To counter this, we employed dissemination strategies through WhatsApp work groups, together with support from the ICU nursing coordinators and the pain management team, which ensured 100% participation by the nurses. The content of the classes was based on best practices but adapted to the local context. This engaged the nurses, who recognized the importance of implementing improvements in pain management. During the 2-week workshop, the nurses could interact with the team in the classroom chat, asking questions and making comments about the classes.
After the end of the workshop, the nurses answered a questionnaire on Google Forms, with suggestions for the improvement plan. Quality tools were incorporated into the improvement plan to optimize implementation.16 All actions were organized according to the 5W2H format (What? Why? Where? When? Who? How? How much?). To prioritize implementation, each action was evaluated using the GUT matrix (severity, urgency, and trend). This tool generates a score at the end to prioritize actions and help in decision-making.
The “NIOT (National Institute of Orthopedics and Traumatology) without pain” campaign created engagement in the unit and helped to raise awareness among nurses. Although the hospital had a pain management protocol, it was not specific to the ICU context. The team felt the need for something practical and visual to optimize nursing time. It was decided develop a decision-making flowchart, starting from the assessment of the patient's level of consciousness, and from there, to decide on the best pain scale to be used, containing guidelines for pain management. The flowchart was aligned with the hospital's pain management protocol and provided specific guidance for ICU patients.
Post-operative pain management is challenging and requires advanced assessment and management skills. In some cases, post-operative pain may be difficult to control, despite the use of multimodal interventions.17 For patients with inadequately controlled pain, the team decided that a request for evaluation and follow-up should be forwarded to the hospital's specialized pain management unit. The monitoring by the pain team was important in assisting the ICU team to manage the pain of these patients.
Pain in intensive care can be caused by factors such as ongoing discomfort related to ICU treatment, acute pain related to illness and surgery, intermittent pain during procedures, and pre-existing chronic pain present before ICU admission. Pain assessment in ICU patients remains a daily challenge for nurses, especially in sedated, intubated, and mechanically ventilated patients. It is known that regular pain assessment leads to better results and better quality of life for patients admitted to the ICU and after discharge from the ICU.18 The need to improve pain assessment in the ICU was perceived, as only pain intensity was recorded through standardized scales (i.e., the Visual Analogue Scale [VAS] and the Critical Care Pain Observation Tool [CPOT]). A new recording instrument was created after the workshop, and in addition to pain assessment using scales, included the recording of other relevant aspects, such as pain intensity, pain location, pain characteristics, and symptoms related to sedation and delirium.
CONCLUSIONThe use of the JBI Evidence Implementation Framework improved compliance with best practices in post-operative pain management, in addition to identifying new opportunities for the sustainability of best practices. Establishing a team and creating engagement in the change process was fundamental.19
The project team, together with the ongoing education team, are planning to strengthen the knowledge acquired in the workshop through the use of realistic simulation in the ICU to ensure the sustainability of the results achieved in the project. In line with the recommendations of the JBI Implementation Manual, subsequent audits will be carried out periodically and will be monitored on a trend chart.
ACKNOWLEDGMENTSThe authors wish to acknowledge the National Institute of Orthopedics and Traumatology, the ICU managers, all the nursing staff for their support and participation in this project, and the Brazilian Center for Evidence-Based Healthcare: A JBI Center of Excellence.
AVAILABILITY OF DATA AND MATERIALSThe authors confirm that the data supporting the findings of this study are available in the article and its supplementary materials.
AUTHOR CONTRIBUTIONSAll authors contributed equally to this paper.
REFERENCES 1. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain 2020; 161 (9):1976–1982. 2. Laufenberg-Feldmann R, Kappis B, Mauff S, Schmidtmann I, Ferner M. Prevalence of pain 6 months after surgery: a prospective observational study. BMC Anesthesiol 2016; 16 (1):91. 3. Baker DW. History of the Joint Commission's Pain Standards: lessons for today's prescription opioid epidemic. JAMA 2017; 317 (11):1117–1118. 4. Baker DW. Statement on pain management: understanding how Joint Commission Standards address pain. Jt Comm Perspect 2016; 36 (6):10–12. 5. Wunsch H, Gershengorn HB, Cooke CR, Guerra C, Angus DC, Rowe JW, et al. Use of intensive care services for Medicare beneficiaries undergoing major surgical procedures. Anesthesiol 2016; 124 (4):899–907. 6. Meissner W, Huygen F, Neugebauer EAM, Osterbrink J, Benhamou D, Betteridge N, et al. Management of acute pain in the post-operative setting: the importance of quality indicators. Curr Med Res Opin 2018; 34 (1):187–196. 7. D’Andrea MS, Fisichella PM. Improvement of post-operative pain control processes and outcomes in veterans of a surgical intensive care unit. World J Surg 2017; 41 (2):419–422. 8. Pasero C, Quinlan-Colwell A, Rae D, Broglio K, Drew D. American Society for Pain Management nursing position statement: prescribing and administering opioid doses based solely on pain intensity. Pain Manag Nurs 2016; 17 (3):170–180. 9. Porritt K, Overall B. Evidence summary. Post-surgery (adults): pain management. The JBI EBP Database. 2023; JBI-ES-360-3. 10. Antunes JdM, Daher DV, Moraes ÉBd, Ferrari MFM, Geraldo MdA. Programa Integrador e o cuidado de enfermagem frente a dor crônica: relato de experiência 2021; 11 (5): Epub 2021-03-23. Portuguese. 11. Porritt K, McArthur A, Lockwood C, Munn Z, editors. JBI Manual for Evidence Implementation [internet]. JBI; 2020. Available from: https://implementationmanual.jbi.global 12. Tagharrobi Z, Mohammad khan Kermanshahi S, Mohammadi I. Evaluation of perception of nurses toward the reasons for using complementary therapies in clinical their practice. Med Surg Nurs J 2017; 5 (1):e68040. 13. Khalil NS. Critical care nurses’ use of non-pharmacological pain management methods in Egypt. Appl Nurs Res 2018; 44:33–38. 14. Castillo RC, Raja SN, Frey KP, Vallier HA, Tornetta P 3rd, Jaeblon T, et al. Improving pain management and long-term outcomes following high-energy orthopaedic trauma (pain study). J Orthop Trauma 2017; 31: (Suppl 1): S71–S77. 15. Naqib D, Purvin M, Prasad R, Hanna IM, Dimitri S, Llufrio A, et al. Quality improvement initiative to improve post-operative pain with a clinical pathway and nursing education program. Pain Manag Nurs 2018; 19 (5):447–455. 16. Kammoun A, Hachicha W, Aljuaid AM. Integrating quality tools and methods to analyze and improve a hospital sterilization process. Healthc (Basel) 2021; 9 (5): 17. Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, et al. Management of post-operative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain 2016; 17 (2):131–157. 18. Kotfis K, Zegan-Barańska M, Szydłowski Ł, Żukowski M, Ely EW. Methods of pain assessment in adult intensive care unit patients: Polish version of the CPOT (Critical Care Pain Observation Tool) and BPS (Behavioral Pain Scale). Anaesthesiol Intensive Ther 2017; 49 (1):66–72. 19. Porritt K, McArthur A, Lockwood C, Munn Z. JBI's approach to evidence implementation: a 7-phase process model to support and guide getting evidence into practice. JBI Evid Implement 2023; 21 (1):3–13.
Comments (0)