
Remember me





What is already known:
Procedural sedation is a commonly used on adult patients in the emergency department. Although uncommon, adverse events during procedural sedation in the emergency department can occur. Adequate patient monitoring during procedural sedation reduces the likelihood of adverse events occurring.What this paper adds
Performing monthly procedural sedation chart audits can aid in identifying instances of non-compliance and ensure a focused approach to addressing areas of improvement during education sessions. The development and implementation of a patient monitoring tool for procedural sedation facilitated staff compliance with evidence-based practices. Recommendations based on lessons learned included exploring substitutes for end-title capnography monitoring and supplies to use in the event of a widespread supply chain disruption. INTRODUCTIONProcedural sedation (PS) is the safe administration of short-acting sedatives during a diagnostic or therapeutic procedure to reduce anxiety and pain during a non-invasive or minimally invasive procedure.1 PS is also known as conscious or moderate sedation. During PS, the patient maintains airway patency, protective airway reflexes, spontaneous respirations, and hemodynamic stability.2 This is in contrast to general anesthesia, where the goal is to render the patient completely unconsciousness and spontaneous ventilation is frequently inadequate.2 The use of PS outside the operating room has grown substantially for diagnostic and therapeutic procedures. The most common areas to use PS are the intensive care unit (ICU) and the emergency department (ED).3 Procedural sedation is a critical component of comprehensive care in the ED performed by emergency physicians and appropriately trained registered nurses.4 Standard nursing care during PS includes continuous monitoring of heart rate, oxygen saturation, electrocardiography, respiratory rate, and non-invasive blood pressure checks every 5 minutes. The American Society of Anesthesiology also recommends monitoring core body temperature and continuous capnography.3 However, in the context of the ED, the fast-paced environment may impede the use of evidence-based practices, particularly during PS procedures. As a result, providers and nurses may not consistently prioritize integrating evidence-based approaches into their decision-making.
Performing PS in the ED improves the quality and safety of patient care by decreasing the time necessary to perform a procedure and increasing the chances of success. Previously, due to the risks associated with adverse events, PS was only performed in the operating room.5 However, studies found that PS can be safely performed by trained ED physicians, resulting in a reduction of overall hospital costs and a decrease in the patient's length of stay.5 The use of PS, while deemed safe and effective with the implementation of proper safety protocols, still poses inherent risks for adverse events. Therefore, adhering to evidence-based guidelines when performing such sedation procedures is imperative. Possible adverse events include cardiac arrest, anoxic brain injury, apnea, hypoxia, laryngospasm, hypersalivation, hypotension, tachycardia, bradycardia, vomiting, aspiration, and prolonged sedation.6 The JBI Model of Evidence-Based Healthcare was used to determine best practices for PS in adults in the ED and served as a guideline throughout the project. An evidence summary of best practices was created by JBI for preventing adverse events when administering PS to adult patients in the ED. The best practices include the following:
Organizations should develop a multidisciplinary PS and analgesia guideline and/or policy. A pre-procedure assessment (including a comprehensive history and physical assessment) should be conducted. During PS and analgesia, continuous oxygen saturation monitoring is recommended alongside vital signs (including heart rate, blood pressure, respiratory rate, and oxygen saturation) and depth of sedation recorded at regular intervals and with audible alarms set appropriately on physiologic monitoring equipment. The rate and quality of ventilation should be monitored with waveform capnography in patients unable to provide a verbal response and where moderate to deep sedation is achieved. It may be useful as an adjunct measure to detect respiratory depression for minimal sedation. Supplemental oxygen is recommended throughout PS and analgesia to reduce the risk of hypoxia and cardiac arrhythmias. Airway and emergency resuscitation equipment should always be accessible, and health professionals caring for patients receiving PS should be trained in using the equipment and responding to emergencies. An appropriately trained and qualified staff member should be in constant attendance during PS and analgesia. An appropriately trained and qualified staff member should provide post-procedural care with the frequency and duration of monitoring determined by the length and complexity of the procedure, the patient's complexities, and the level of sedation provided.One systematic review identified that adverse events in adults undergoing PS in the ED are rare; however, they can occur. The most frequent events were hypoxia, vomiting, hypotension, and apnea. Hypoxia occurred at 40.2 per 1,000 sedations; vomiting at 16.4 per 1,000 sedations; hypotension at 15.2 per 1,000 sedations; and apnea at 12.4 per 1,000 sedations.7 Adverse events can be avoided when a trained physician and nurse remain in constant attendance. Evidence suggests supplemental oxygen therapy and continuous monitoring of the heart rate, respiratory rate, and oxygen saturation levels.7 Furthermore, it is advisable to ensure uninterrupted monitoring of end-tidal capnography during the procedure.1 Non-invasive blood pressure checks should be conducted every 5 minutes during the initial 15 minutes of the procedure and every 10 minutes after that until the patient meets discharge criteria. Discharge criteria includes the use of the Aldrete Discharge Readiness tool, which comprises 5 criteria. Each criterion is worth 2 points; a minimum score of 8 indicates readiness for discharge.8 Finally, immediate access to emergency airway and resuscitation equipment is essential.1
This project was implemented at a large non-metropolitan hospital in the southeastern United States. Designated as a Level II Trauma Center, the ED, which is in operation 24/7, provides trauma and high acuity care for approximately 897,722 individuals. Procedural sedation is performed on patients of all ages in the ED, with the ability to utilize the hospital's ICU in the event of an adverse outcome. Common medications used in the ED for PS include propofol, ketamine, and dexmedetomidate.3 An average of 24 PS of adult patients are performed per month at this facility. The health care workers directly involved in PS in the ED include 60 registered nurses and 16 physicians. An initial audit of 24 patient charts revealed that evidence-based practice guidelines were not being consistently followed for all sedation procedures.
The implementation site has a PS policy in place; however, the policy has not been updated since August 2021. The policy defines PS and provides pre-procedure, intra-procedure, and post-procedure monitoring guidelines. Although clear guidelines are available, the instructions provided for physicians and nurses are combined into a single document. Due to the lack of role separation in the guidelines, identifying the responsibilities of the registered nurse quickly and easily can be difficult. The project began with a clinical audit comparing current practices with best practices defined by the JBI Practical Application of Clinical Evidence System (PACES) audit and feedback tool.9 The audit criteria were defined by the Canadian Anesthesiologists’ Society, the European Society of Anaesthesiology, the European Board of Anaesthesiology, and the American Society of PeriAnesthesia Nurses.1 The audit results were reviewed collaboratively with the nursing leadership in the ED to identify opportunities for change and create systems and processes which align with best practices. To understand the registered nurse's role during PS, the project team was led by a registered nurse with designated registered nurses as team members. After 1 month, a follow-up audit was performed to assess the effectiveness of the implementation strategies and provide a platform for ongoing improvement.
OBJECTIVESThis project aimed to improve evidence-based practices during the PS of adult patients in the ED.
The specific objectives were to:
1. determine current compliance with evidence-based practices regarding PS of adult patients in the ED; 2. develop and implement strategies to address areas of non-compliance with evidence-based practices regarding the PS of adult patients in the ED; and 3. evaluate compliance with evidence-based practices regarding PS of adult patients in the ED after the implementation of improvement strategies. METHODSThis evidence implementation project used the JBI Model for Evidence-Based Healthcare.10 The JBI evidence implementation approach is grounded in the audit and feedback process, along with a structured approach to identifying and managing barriers to compliance with recommended practices. It consists of 7 phases: (1) identification of practice area for change, (2) engaging change agents, (3) assessment of context and readiness to change, (4) review of practice against evidence-based audit criteria, (5) implementation of changes to practice, (6) re-assessment of practice using a follow-up audit, and (7) consideration of the sustainability of practice changes.9
Implementation planningIn Phase 1, the project team identified PS in the ED as a high-risk procedure and the potential for non-compliance with best practices during these procedures. The project team included 1 director of nursing practice, 1 clinical coordinator of nursing practice, 2 nursing informatics analysts, and 1 bedside ED nurse. The director of nursing practice and clinical coordinator of nursing practice worked together as project sponsors. During Phase 2, stakeholder support was secured, including the interim ED manager and the ED nurse educator. The interim ED manager was responsible for operational and staff management. The nursing informatics analysts created a template within the electronic health record (EHR) to easily locate charts of patients who had received moderate sedation. The bedside ED nurse was responsible for data collection and staff education on best practices throughout the audits.
Baseline assessment and implementationDuring Phase 3, the project team conducted a context analysis at the project site to determine readiness for change and evidence implementation. Eight elements were considered when determining readiness for change: decision-making structure; workplace culture; communication; leadership; resource availability; staff knowledge, skills, attitudes; commitment to quality management; and interdisciplinary relationships.9 A meeting was held with the stakeholders where elements of readiness for change were discussed. The context analysis revealed strengths and weaknesses within the ED supporting readiness for change among staff and leadership.
Using a JBI evidence summary,1 eight audit criteria were developed based on best practice recommendations for PS and analgesia in adult patients, for use in Phase 4. The audit criteria were accessed from PACES. Table 1 shows the audit criteria (used for both the baseline and follow-up audits), together with a description of the sample and the approach for measuring best practices for each criterion. The project team determined a sample size of 24 patients based on the number of adult PS performed each month in the ED. The baseline audit was conducted using a random sample from July 27 to August 26, 2022, and entered into PACES.
Table 1 - Audit criteria, sample, method used to measure compliance, and audit guide Audit criteria Sample Method used to measure compliance with best practice Audit guide A procedural sedation and analgesia guideline and/or policy is in place. Policy review Nurses from the project team confirmed the guideline and/or policy is in place. “Yes” if there is a guideline and/or policy for procedural sedation and analgesia.After reviewing the baseline audit results, Phase 5 was conducted from August 1 to December 1, 2022. The team employed the GRiP tool to identify barriers hindering best practices. Using these insights, the team then developed strategies to improve compliance with best practices.
Impact evaluation and sustainabilityDuring Phase 6, a follow-up audit was conducted to determine any improvements in practice following implementation. The audit also aimed to identify opportunities to refine the PS processes and identify any variability in workflow or practice. There were no changes in the sample size of 24 patients. The follow-up audit took place from December 1 to 31, 2022, with the results entered into PACES.
During Phase 7, consideration was given to the sustainability of the practice changes. The project team agreed that monthly audits should be conducted to monitor progress and identify any other barriers. Monthly audits are now performed by nurse leaders within the department and reported to the department's Quality and Safety Committee for ongoing review and management.
ANALYSISThe results were measured using the descriptive statistics embedded in PACES in the form of percentage changes from baseline.
ETHICSInstitutional Review Board (IRB) approval was not required; however, quality improvement designation was approved for collection of patient data. Results were provided by the performance improvement department to the leadership team in the ED. Patient charts were reviewed using medical record numbers to protect patient privacy.
RESULTSIn Phase 1, the project team identified the potential non-compliance with best practices during PS in the ED. During Phase 2, stakeholder support was secured, which included the interim ED manager and the ED nurse educator. During a context analysis in Phase 3, the project team identified positive indicators of readiness for change in the workplace culture, leadership, and commitment to quality management as evidenced by the entire ED's eagerness to learn and willingness to explore process changes. Challenges were identified related to a lack of ED staff education surrounding EBP with procedural sedation.
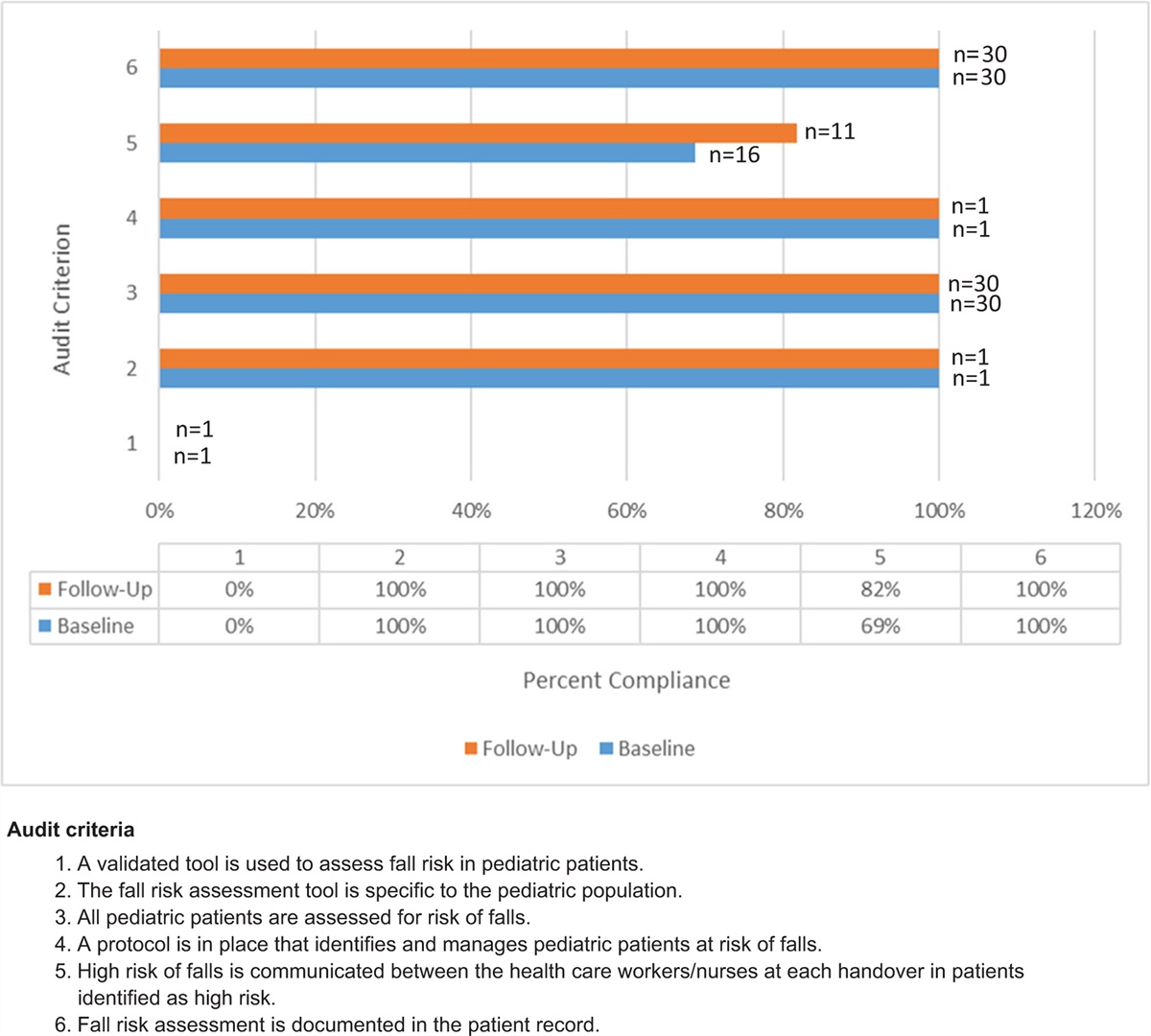
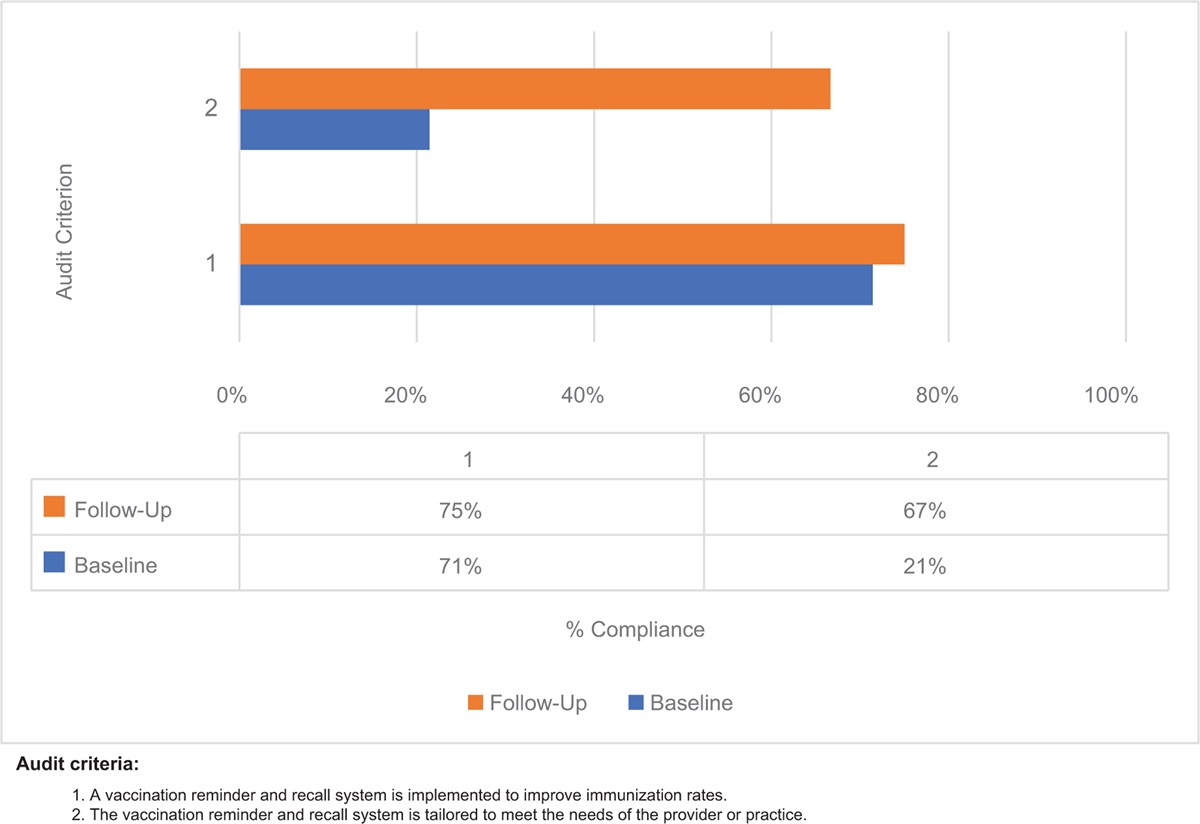
During Phase 4, 24 patients were randomly selected for the baseline audit. These patients were 18 years or older and had received PS in the ED during the mentioned timeframes. Figure 1 displays the results of the baseline audit. The criteria with the highest compliance (100%) were the organization having a current pre-procedural policy in place (Criterion 1, n = 24), completion of a pre-procedure assessment (Criterion 2, n = 24), accessible airway and emergency resuscitation equipment available (Criterion 6, n = 24), appropriately trained and qualified person in constant attendance (Criterion 7, n = 24), and appropriately trained and qualified person providing post-procedural care (Criterion 8, n = 24). The second highest percentage of compliance (at 83%) was using supplemental oxygen throughout the PS (Criterion 5, n = 20). The poorest performing measures included documentation indicating patients had received adequate monitoring of vital signs (Criterion 3, n = 9) and waveform capnography during PS (Criterion 4, n = 6). Vital signs were assessed at the correct frequency 38% of the time, and wave capnography was monitored continuously 25% of the time.
 Figure 1:
Figure 1: Compliance (%) with best practice for audit criteria at the baseline audit and follow-up audit.
During Phase 5, the GRiP matrix (Table 2) was used to identify barriers to implementation. Knowledge deficits regarding best practices were an anticipated barrier. The strategy to address this barrier was an educational PowerPoint presentation on best practices, followed by meetings with staff to review the presentation and disseminate the results of the baseline audit. Before the meeting, the JBI evidence summary, the PowerPoint presentation, and baseline audit findings were emailed to stakeholders. Upon reviewing the information, the stakeholders agreed with the plan to proceed with the project and demonstrated comprehension of the project's goals before scheduling the educational meeting with the ED team. During the educational meetings, the evidence summary and the audit criteria were shared with the entire ED care team, which included the registered nurses, paramedics, ED technicians, and board coordinators.
Table 2 - Getting Research into Practice (GRiP) analysis Barrier Strategy Resources Outcomes • Lack of staff education on evidence-based practice regarding the monitoring and assessment of adult patients during procedural sedation in the Emergency Department. • Create educational PowerPoint.The second barrier identified was twofold: increased nursing turnover rate and a limited number of experienced ED nurses to help execute PS. Like other health care areas, the project ED struggled with the nationwide nursing shortage crisis and high turnover rates and, therefore, the department had an unusual number of novice nurses.
For novice nurses, learning and retaining the required education in the early stages of their career can be difficult. To address the second barrier, a strategy was created that entailed the development and implementation of a patient monitoring tool (Appendix I, https://links.lww.com/IJEBH/A165). The tool was used to assist nursing staff in identifying and adopting best practices during all PS for adult and pediatric patients. The ED provided medical care to a diverse patient population of different age groups and medical conditions, necessitating extensive training for novice and experienced nurses to care for this patient cohort.
During Phase 6, 24 charts were audited after the two strategies had been implemented. Results of the audits are seen in Figure 1. The comparison between the baseline and follow-up audits showed an overall improvement in compliance with Criterion 3, rising from 38% to 96%; Criterion 4, rising from 25% to 79%; and Criterion 5, rising from 83% to 88%. No changes were noted for Criteria 1, 2, 6, 7, and 8, which were 100% at baseline.
In Phase 7, the project team identified the need for monthly audits to monitor progress with EBP compliance and to continue recognizing improvement opportunities. Monthly audits will be performed by the newly appointed Director of Emergency Services and reported to the department's Quality and Safety Committee for ongoing review and management. Oversight of the ongoing educational module will be maintained by the department's Nurse Educator and updated as new guidelines and EBPs become available. This work will continue past the project's end date as the implementation tool will continue to be available for nursing staff to support documentation and future compliance audits.
DISCUSSIONThis implementation project aimed to improve the hospital's compliance with best practices regarding the PS of adults. The project was conducted in the ED of a large Level 2 trauma center in the southeastern United States. Twenty-four PS charts were reviewed for the baseline audit. Information from the baseline audit enabled the team to identify barriers to compliance with best practices.
Additionally, a policy review was conducted, revealing the health care system's PS policy had not been revised since August 2021. The policy defined PS and outlined pre-procedure, intra-procedure, and post-procedure monitoring protocols. Although the policy included clear guidelines, the instructions for physicians and nurses were presented in a single document without clear role differentiation. Consequently, identifying the registered nurses’ responsibilities within the guidelines quickly and easily was challenging. The project team used the GRiP process to identify and apply strategies to these barriers. After project implementation, 24 additional charts were selected for the follow-up audit. Comparison between the two audit sets provided insights for further recommendations.
The follow-up audits showed improved compliance with Criteria 3 and 5. Criterion 3 evaluated the intervals at which vital signs were assessed during the PS. The compliance rate increased from 38% to 96%. Criterion 5, administering supplemental oxygen during PS, increased from 83% to 88%. These increases in compliance were likely due to the recent staff education and the use of the PS patient monitoring tool. Moving forward, routine staff education will be performed regarding PS. Monthly chart audits will also be performed to ensure sustainability and identify areas of non-compliance that will be addressed during educational sessions.
Compliance with Criterion 4, monitoring end-tidal capnography to assess patients’ ventilatory effectiveness, rose from 25% to 79%. Although the results were significant, the team believes there is still room to improve this criterion; however, sustainability may be difficult due to past issues with inadequate equipment. The project members were surprised to discover a baseline compliance rate of only 25% for this criterion. These findings highlight that the challenges of obtaining supplies post-COVID are still affecting supply chains. ED leaders will continue to look for the most cost-effective and readily available supplies to improve the availability of these supplies for monitoring end-tidal capnography.
The project team determined that the most critical strategy to maintain future compliance with Criteria 3 and 5 would be to consistently offer educational sessions on EBPs for PS. Additionally, conducting monthly PS chart audits will help identify areas of non-compliance and allow the educational sessions to specifically target areas of improvement. Due to the supply chain challenges resulting from the COVID-19 pandemic, end-tidal capnography supplies were difficult to obtain after they had been sourced and ordered, which decreased compliance with Criterion 4. Further recommendations are needed to identify alternative end-tidal capnography monitoring devices, equipment, and supplies in the event of a widespread supply chain-related event. No changes were noted for Criteria 1, 2, 6, 7, and 8, which were 100% at baseline.
CONCLUSIONSAppropriate patient monitoring is vital in promoting the best outcomes for patients receiving PS in the ED. The project goal was to determine current compliance with EBPs regarding PS for adult patients, and to design and implement strategies to address any areas of non-compliance. After implementation, the project aimed to assess compliance with best practices through a follow-up audit. An overall increase in compliance was observed after the implementation of EBPs for the PS of adult patients. To ensure sustainability, leaders in the ED continue to conduct monthly chart audits to ensure compliance, necessitating repeated education due to turnover and new nurse hires. Exploring modifications to the PS template in the EHR may be beneficial as such changes would create an electronic guide similar to the PS patient monitoring tool. The project team has also prioritized exploring the link between improved EBP compliance and adverse events during adult PS in the ED. No similar or relevant projects were found, and therefore, it was not possible to compare or evaluate the project results for similarities or differences to other areas.
ACKNOWLEDGMENTSThe authors would like to acknowledge Emily Edwards, RN, DNP, Director of Nursing Practice, and Chessie Womack, RN, DNP, Clinical Coordinator of Nursing Practice, for their partnership, assistance in workflow solutions, and tireless efforts to bring evidence-based care into practice.
Comments (0)