
記住我


A 61-year-old man was admitted to a local hospital for abdominal pain and subsequently diagnosed with a perforated gastric ulcer and conservatively treated. However, owing to the subsequent worsening of his condition, an emergency surgery was performed. Omental filling of the perforated part of the gastric antrum and gastrostomy for gastric decompression were performed. Post-operative leakage subsequently occurred, and a gastrocutaneous fistula formed at the wound. He was transferred to our hospital for the treatment of gastrocutaneous fistula.
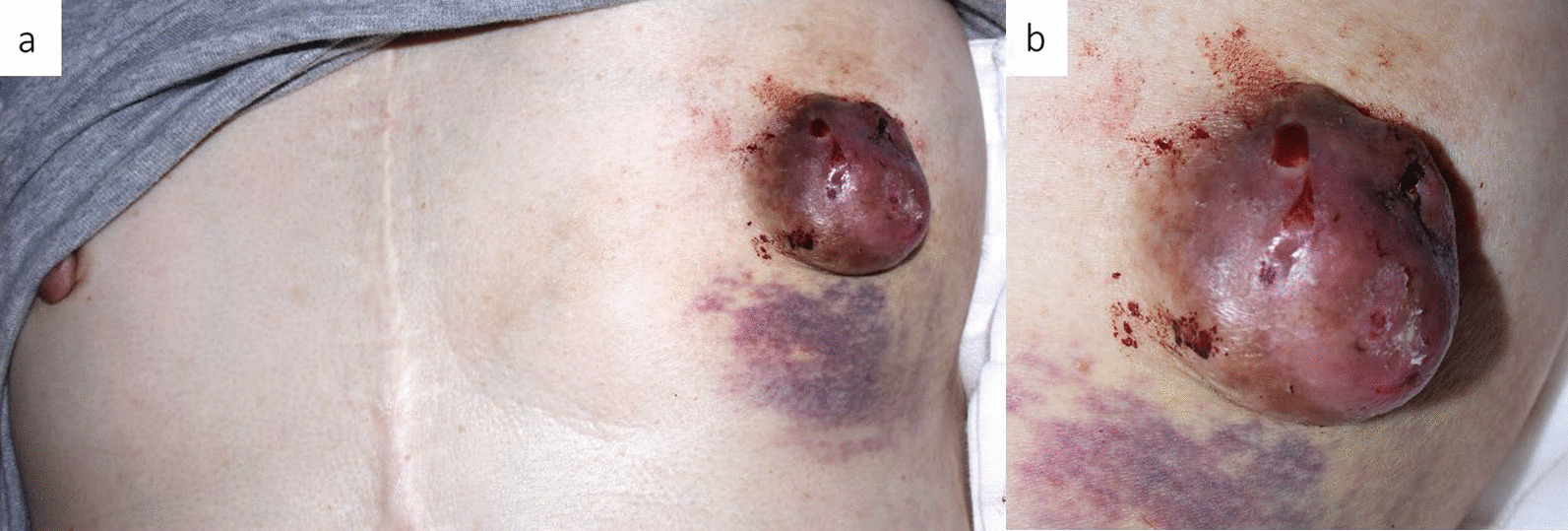
The gastrocutaneous fistula on his epigastric region was 10 cm in size. A gastrostomy was noted on his left hypochondrium (Fig. 1a). He had erythema with scales that was scattered throughout the body due to psoriasis. The huge gastrocutaneous fistula resulted in discharges of more than 1000 mL of gastric juice daily, indicating a high-output gastrocutaneous fistula. It subsequently caused dehydration, electrolyte abnormalities, metabolic acidosis, and acute kidney injury. Laboratory examination showed the following findings: hemoglobin, 10.4 g/dL; albumin, 2.7 g/dL; and creatinine, 1.37 mg/dL owing to the loss of gastric secretion. The test for Helicobacter pylori antibody was positive.
Fig. 1
Surgical findings. A gastrocutaneous fistula (yellow arrow) (a) was observed in the epigastric region. A gastrostomy was noted on the left hypochondrium (yellow arrowhead) (a). Laparotomy with a midline abdomen was performed to avoid a gastrocutaneous fistula (yellow arrow). Severe intra-abdominal adhesions were observed (b). Resection of the stomach on the anal (c, yellow arrow; gastrocutaneous fistula) and oral sides (d) was performed. Roux-en-Y anastomosis was performed (e). Open abdomen management was performed with ABThera™ (f). A fistula was found on the anterior side of the antrum of the stomach (g)
We attempted to improve the nutritional status of the patient by providing enteral nutrition for the fistula and central venous nutrition for the surgery. Enteral nutrition was performed by placing a feeding tube through the gastrocutaneous fistula into the jejunum using fluoroscopy.
The patient also had a skin disease and inflammatory induration around the fistula, which could have complicated abdominal closure. Therefore, the surgery was performed with preparation for open abdomen management.
Surgical findings revealed severe intra-abdominal adhesions. Further, distal gastrectomy reconstruction with Roux-en-Y anastomosis and jejunostomy were performed (Fig. 1b–e). As the preoperative condition of the patient was poor and extended adhesion peeling was performed, open abdomen management was performed to detect anastomotic leakage and unpredictable damage of adhesion peeling. Moreover, open abdomen management was performed using ABThera™ (Fig. 1f). A fistula in the pylorus was found in the resected specimen. The fistula had no malignancy findings on pathology (Fig. 1g). The ABThera™ device was replaced every 2 days for observation of gastrointestinal injury and anastomotic leakage (Fig. 2). Abdominal closure was performed 9 days after gastrectomy (Fig. 3).
Fig. 2
Open abdominal management. Replacement of the ABThera™ to observe abdominal secondary injury
Fig. 3
Secondary surgery. Abdominal organs were capsulized after open abdomen management (a). A fascia was expanded by undermine method and separated to abdominal closure (b, c). Abdominal closure by the secondary surgery (d)
The postoperative course was uneventful, and oral nutrition was resumed on postoperative day 7. He was discharged from the hospital without complications on postoperative day 80. Hospital stay was 128 days. At the time of discharge, his nutritional status improved, with albumin and creatinine levels of 3.5 g/dL and 1.79 mg/dL, respectively.
留言 (0)