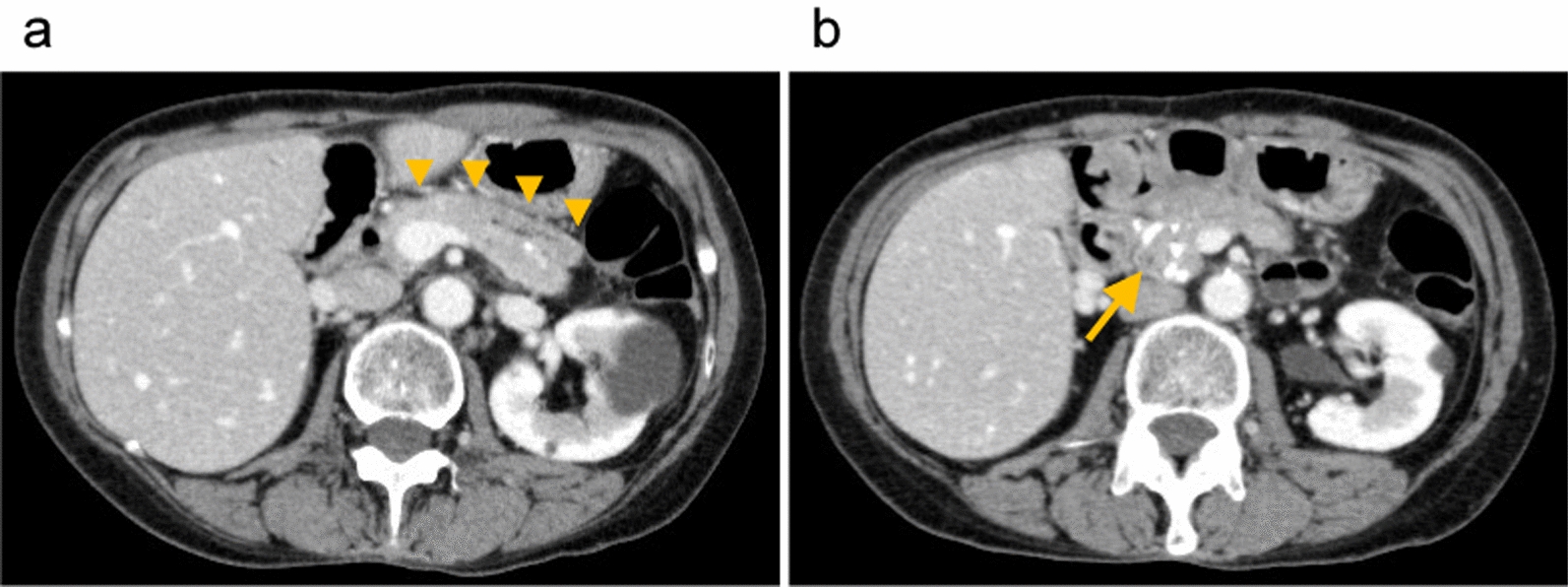
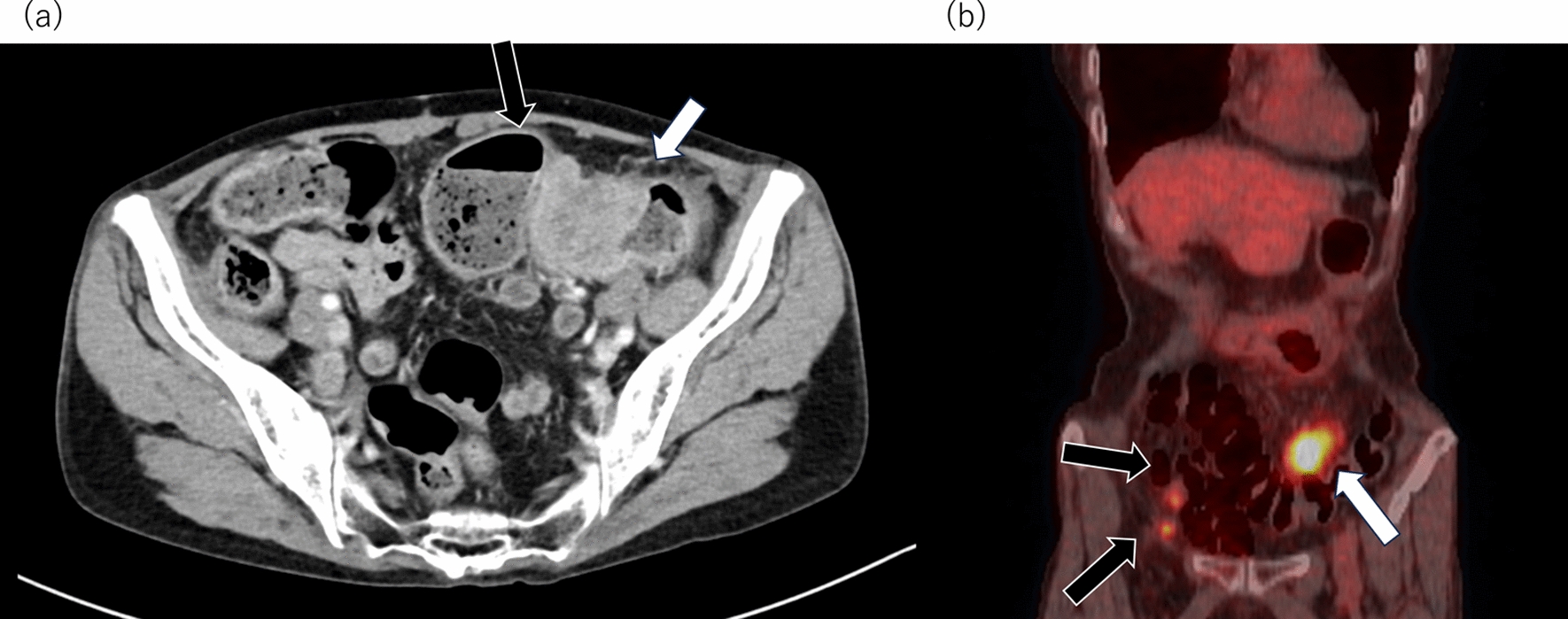
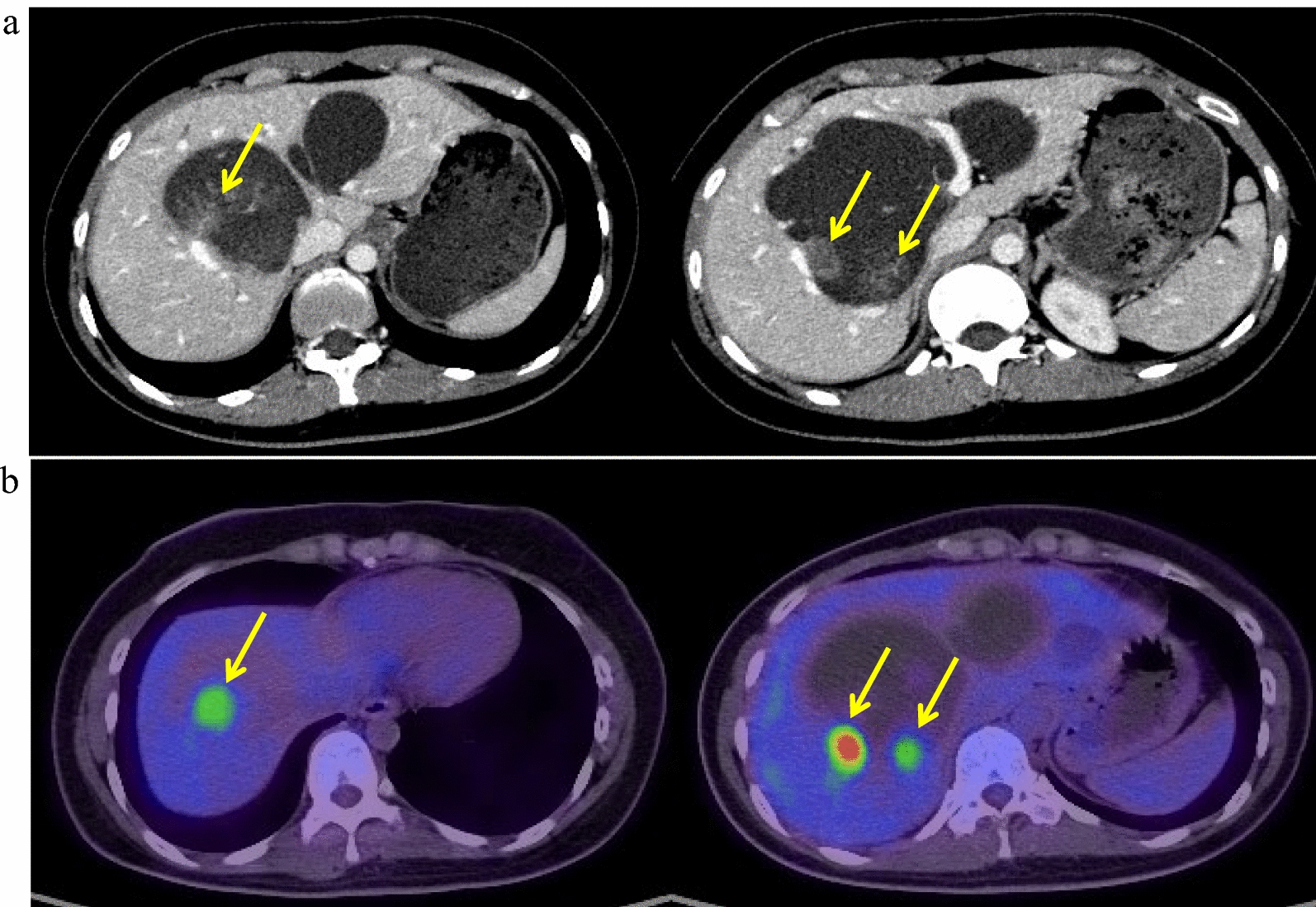
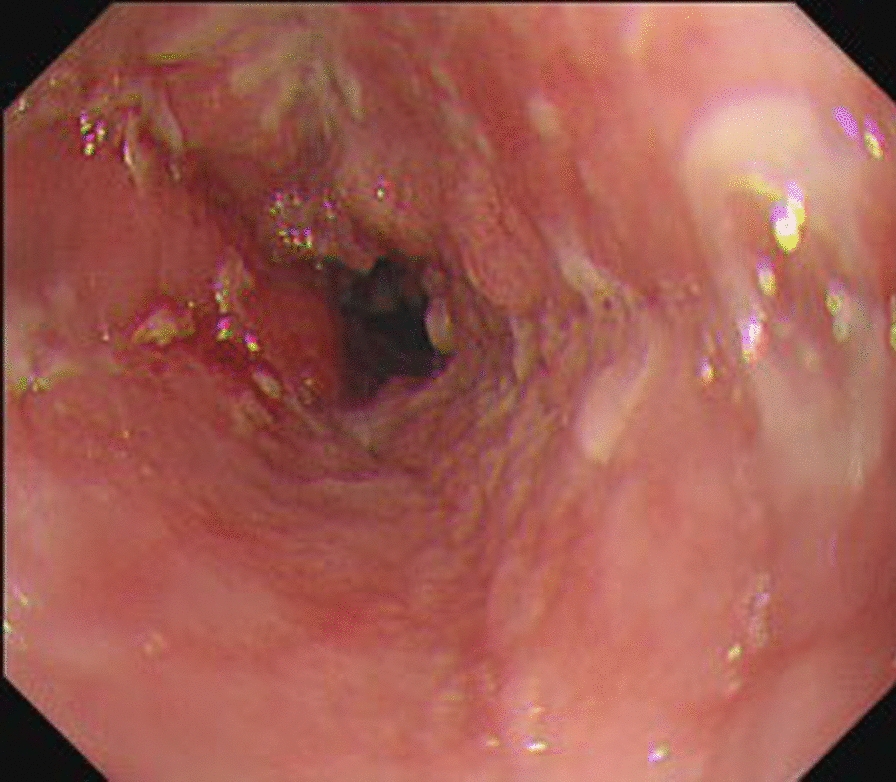
Herein, we report a case wherein multidisciplinary therapy was applied to successfully manage metastatic and locally recurrent SCCA. The treatment regimen included DCF chemotherapy for metastatic recurrence in the para-aortic lymph nodes following CRT, IMRT for metastatic re-recurrence in the same lymph nodes after DCF, and abdominoperineal resection for the local recurrence of the primary lesion. This comprehensive treatment approach led to complete remission and long-term overall survival (OS) and PFS.
Traditionally, the standard chemotherapy regimen for metastatic SCCA involves CDDP + 5-FU, based on a small retrospective trial [10], which shows a 66% response rate with only one patient achieving CR. However, the efficacy of the DCF regimen for unresectable, locally recurrent, or metastatic SCCA was demonstrated in the Epitopes-HPV02 study [11], where 66 patients were treated with standard or modified DCF regimens, resulting in an 89% response rate, with 30 patients achieving CR. Additionally, the InterAct study reported the effectiveness of carboplatin (CBDCA) and paclitaxel (PTX) regimens for inoperable locally recurrent or metastatic diseases [12]. Taxol anticancer agents have been used owing to their association with HPV and SCCA [13]. HPV types 16 and 18 encode the E6 oncoprotein, which degrades the tumor suppressor gene p53 [14]. p53-deficient cells are more sensitive to taxol antitumor agents owing to increased G2/M arrest and apoptosis. Therefore, the addition of docetaxel to the 5-FU and CDDP regimens has shown promise [15]. The 2023 National Comprehensive Cancer Network (NCCN) guidelines recommend these regimens and others for metastatic anal cancer [5], with recent retrospective studies favoring the DCF regimen over doublet regimens (FU + CDDP or CBDCA + PTX) in terms of OS and PFS [16].
In our case, DCF chemotherapy was administered for metastatic recurrence following CRT, and CR was achieved. Subsequently, the limited metastatic recurrence in the para-aortic lymph nodes was treatable using radiotherapy. DCF chemotherapy has demonstrated effectiveness in preventing metastatic recurrence of SCCA. Although HPV testing was not conducted in this case, considering the HPV status when selecting taxol as an antitumor agent is recommended.
The 2023 NCCN guideline recommends surgery for patients with locally recurrent disease and systemic chemotherapy for those with extrapelvic metastatic disease. However, there is no consensus on the optimal second-line treatment, and recommendations for local recurrence after metastatic recurrence, as in this case, are lacking. Analysis of secondary treatment in the Epitopes-HPV01 and Epitopes-HPV02 studies suggests that complementary treatments, such as surgery or radiotherapy, may lead to better prognosis [17]. Fourteen patients received complementary treatment, and their median OS and PFS were 48.3 months (NE-NE) and 31.3 months (23.2–NE), respectively. In contrast, 59 patients received systemic treatment, such as chemotherapy or immunotherapy, and their median OS and PFS were 11 months (8.4–15.4) and 4.9 months (3.3–7), respectively.
In our case, radiotherapy was administered for metastatic recurrence after DCF chemotherapy, and abdominoperineal resection was performed for local recurrence. This approach effectively suppressed long-term distant recurrence by treating para-aortic metastases with radiotherapy after suppressing micrometastases with DCF. Local recurrences of the primary tumor were completely resected without causing distant metastasis. This case highlights the effectiveness of complementary treatments, even for metachronous recurrence.




Comments (0)