Duodenal duplication cyst at the second part of the duodenum with congenital duodenal position anomaly completely resected by laparoscopic partial duodenectomy: a case report
The best treatment for DDC is complete resection to prevent future complications, including malignancy, because DDC may contain dysplasia mucosa or early malignant tissue. Three cases of malignancy arising from DDC were reported [6]. However, excision of the DDC, as much as possible, and mucosal stripping were selected when complete resection was hindered by the site and size of the DDC. Theoretically, pancreatoduodenectomy completely resects DDC wherever it is present but should remain the ultimate option [7] for long-term quality of life.
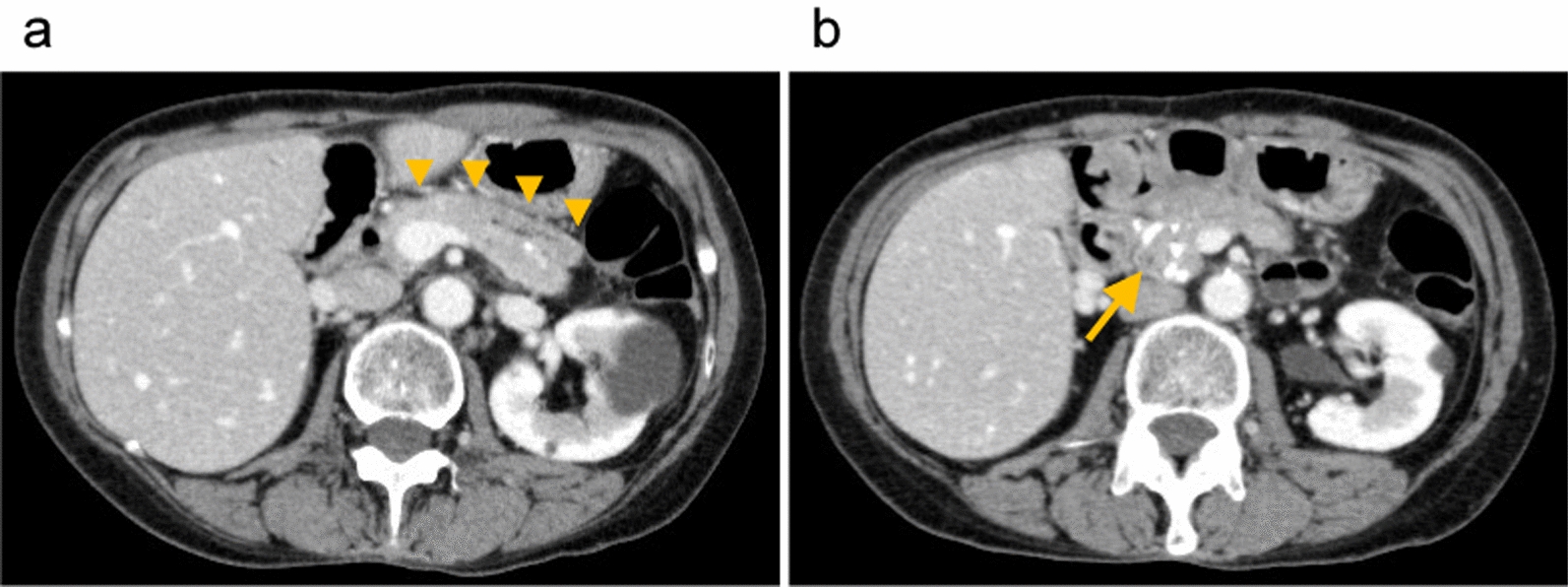
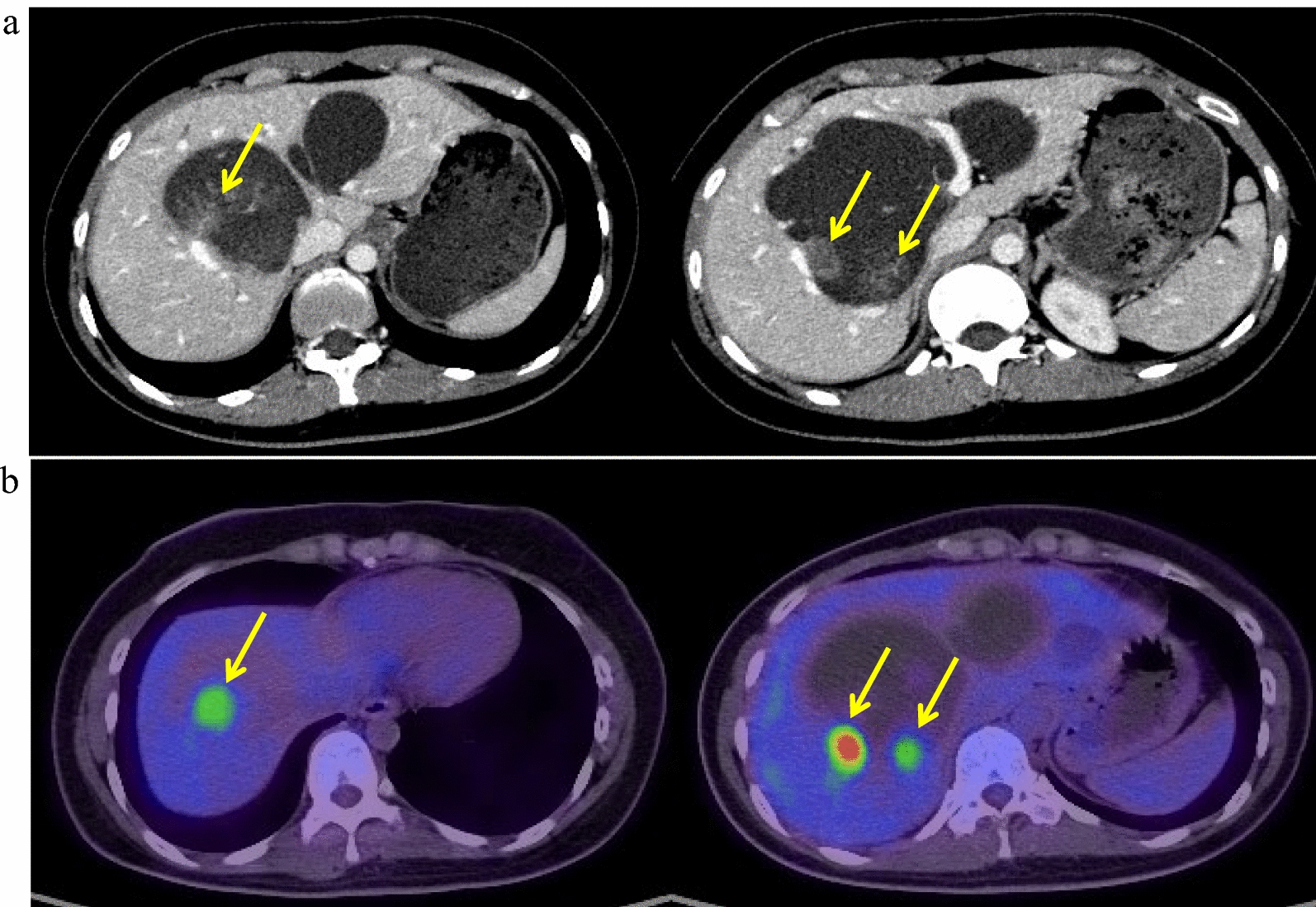
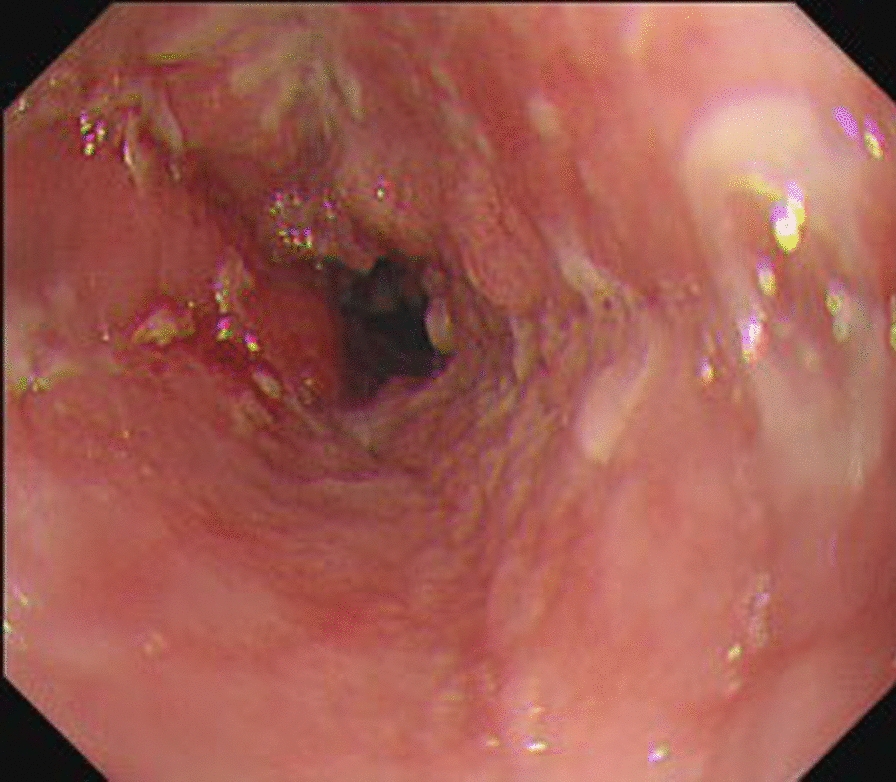
The preoperative examination revealed that the DDC was relatively large and intimately attached to the second part of the duodenum. As previously reported, subtotal resection of the DDC and mucosal stripping were considered to be a valid treatment option. Endoscopy-assisted windowing [8] is another option in unresectable cases, although maintaining the mucosal layer bears a slight risk of malignancies [6]. Mucosal stripping is safe and has few complications. However, postoperative stenosis or stricture could occur. Duodenal lesions > 30 mm carry a risk of postoperative complications following endoscopic mucosal resection; duodenal stricture occurred in 0.8% of cases [9]. Considering that our patient still has a long life and that there would have been the possibility of future complications such as stenosis, we considered that complete resection with reconstruction was the best method to treat the DDC ensuring no future complications. Endoscopy-assisted laparoscopic full-thickness resection could have been another option [10], if an endoscope could have been inserted.
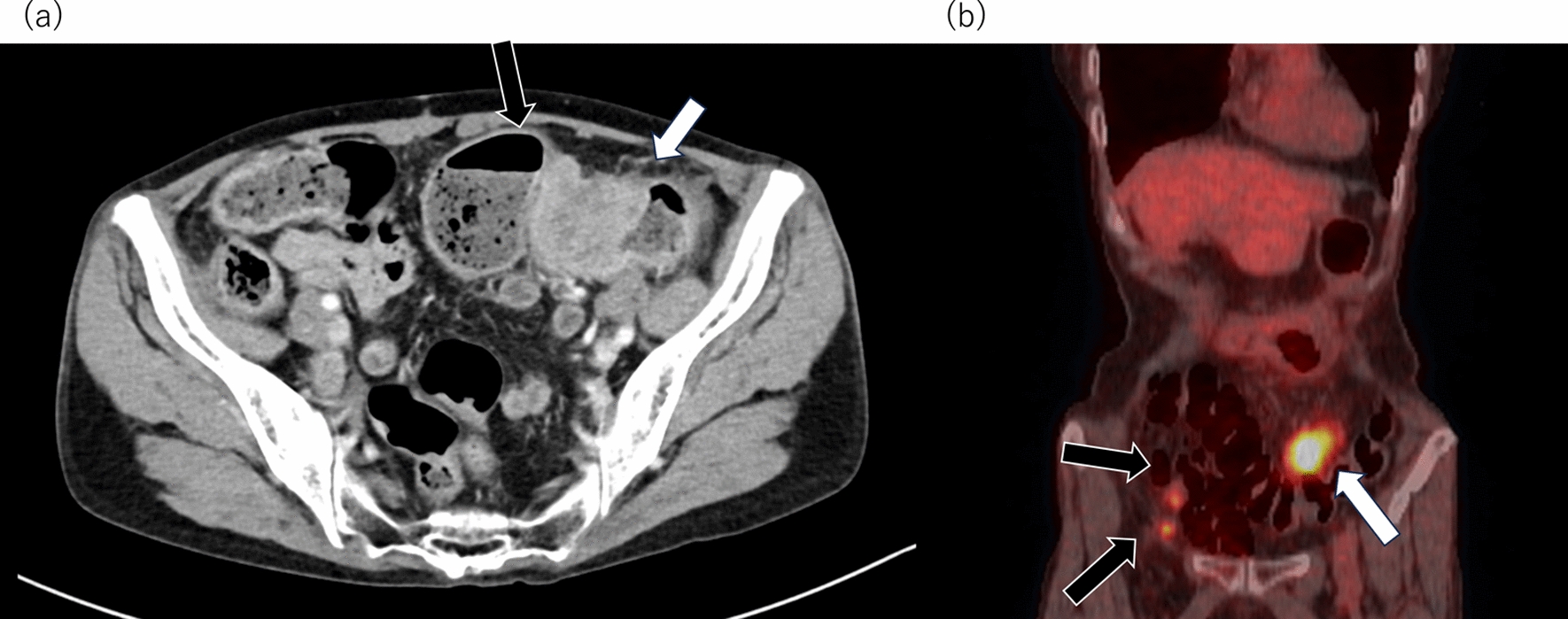
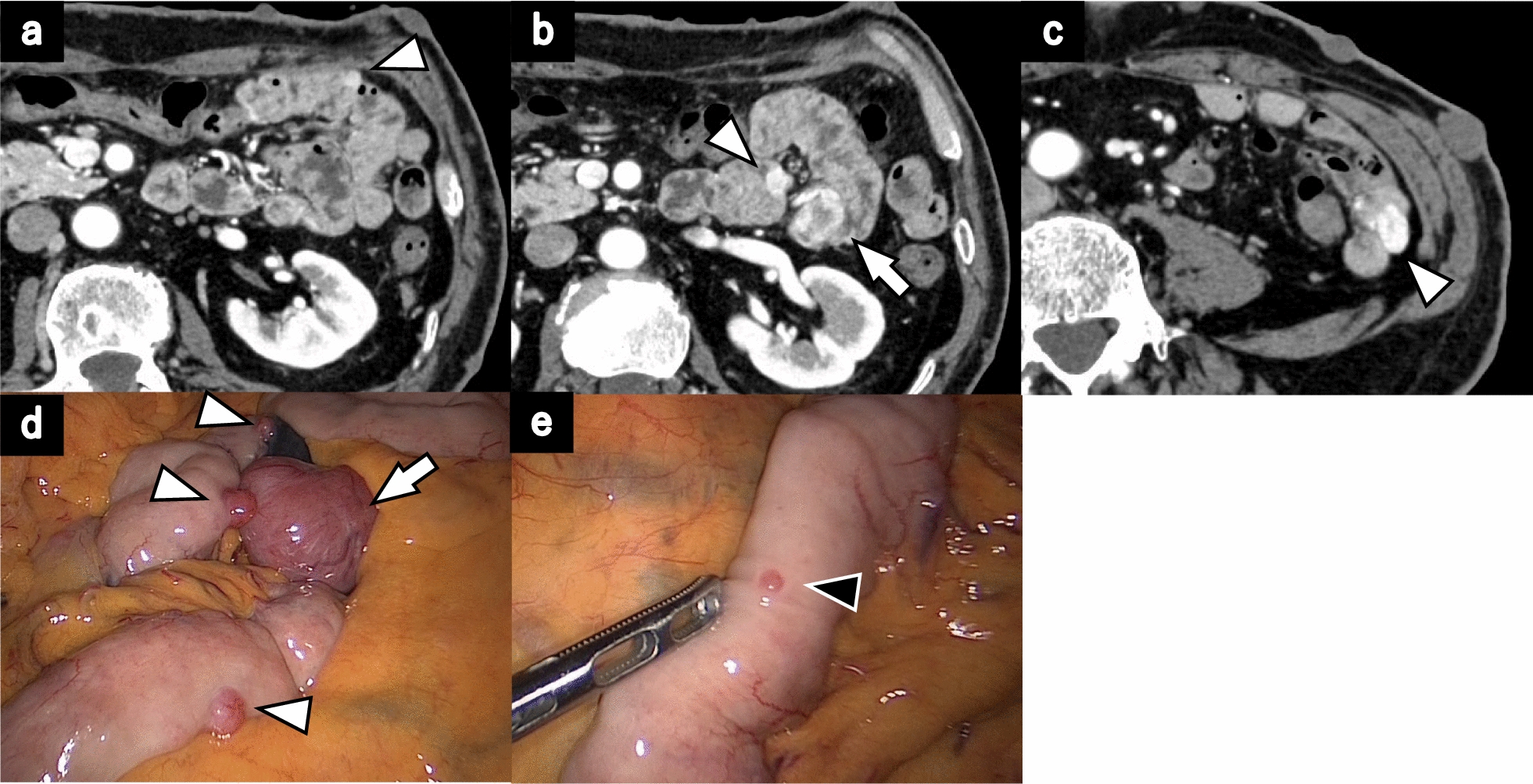
We preoperatively planned to perform total resection with a defect hole anastomosed to the jejunum with Roux-en-Y reconstruction rather than simple suture closure to prevent postoperative duodenal stricture. Intraoperative laparoscopic observation showed that the papilla of Vater was distant from the DDC. Furthermore, the duodenum was easily mobilized to the ligament of Treitz because of a congenital duodenal position anomaly. Hence, total resection of the DDC with the second to fourth parts of the duodenum via a retrocolic route duodenojejunostomy was performed. We selected this reconstruction approach because it guarantees a more physiologically normal food pathway, whereas a Roux-en-Y anastomosis could cause Roux stasis syndrome [11,12,13].
To our knowledge, the same duodenal position anomalies have been reported in three cases [14,15,16]. Pham et al. indicated that this anomaly was caused by folding of the second part of the duodenum at the junction of the foregut, midgut, or proximal midgut [15]. They also reported that the second and third parts of the duodenum did not adhere strongly to the adjacent organs. Hence, duodenal mobilization was not difficult [15]. In the present case, the mobilization of the duodenum was facilitated using laparoscopy. The procedure used in this case was not applied as easily in all previously reported cases by laparoscopy because in most cases the second to fourth parts of the duodenum were firmly fixed with the ligament of Treitz. Despite the relatively low occurrence rate, DDC is related to malignancies, and complete resection is an ideal treatment option when possible. The procedure reported herein may be a valid option for large DDCs distal to the Vater papilla, particularly in cases of a congenital duodenal position anomaly.




Comments (0)