
記住我






In the United States, non-Hispanic (NH) Black birthing people have an increased risk of adverse birthing outcomes known as severe maternal morbidity (SMM) (RR = 1.2–2.6).1–4 The excess SMM risk among NH Black birthing people compared with NH White is hypothesized to be almost, if not completely, preventable.5 Yet racial disparities in SMM risk have persisted over time and across places.6,7
Interventions targeting racial disparities in any maternal health outcome require attention to the hypothesized root causes of the disparity (e.g., racism and income inequality), their midstream manifestations (e.g., access to quality care and healthy food environments), and their potential downstream risk factors (e.g., individual-level comorbidities and younger maternal age).8,9 From an applied public health perspective, downstream risk factors may be perceived as a more immediate intervention opportunity, whereas continuing to identify opportunities to directly address midstream and upstream root causes of the disparity.
One such downstream risk factor is hypertensive disorders of pregnancy (HDP). HDP, which includes by definition gestational hypertension, mild and severe preeclampsia, eclampsia, hemolysis, elevated liver enzymes, low platelet count syndrome (HELLP), and chronic hypertension, are known contributors to SMM and maternal mortality.10–14 In studies of SMM, HDP usually encompasses preeclampsia, gestational hypertension, and chronic hypertension.15 Although eclampsia is an HDP, this diagnosis is excluded as a risk factor because it is one of the 21 SMM outcomes.16
HDP is estimated to occur in 6%–10% of US pregnancies.17–19 HDP rates are highest among NH Black birthing people compared with NH White birthing people, and birthing people living in the southern US, compared with birthing people living in other US regions.17–19 As such, HDP has been hypothesized to be an important driver of racial disparities in SMM.7,15 This has led to several proposed strategies to target HDP as a critical opportunity for reducing SMM disparities (e.g., enhanced models of prenatal care, patient safety bundles).7,15,20 However, to date, no studies have explicitly estimated the proportion of the Black–White racial disparity in SMM that operates through the pathway of HDP. Thus, it is unclear how effective targeting HDP (prevention and control) would be for reducing Black–White racial disparities in SMM. Equally important, we do not know how much of the disparity would remain even if HDP were eliminated, requiring alternative or additional strategies.
This conceptualization of HDP as a potential cause of increased SMM risk among NH Black birthing people is based on the assumptions that (1) the excess SMM risk among NH Black compared with NH White birthing people is preventable and (2) that the NH Black–White risk difference (RD) is driven by structural racism.
Individual-level race in SMM research is often used as a proxy for investigating how racism produces inequitable excess risk (i.e., preventable and therefore plausibly avoidable risk) among NH Black pregnancies compared with NH White.21 There is no evidence that racial differences in HDP are due to genetic causes.22 Rather, the incidence and management of HDP varies by racial group through differential access to health-related knowledge and resources by race (e.g., access to quality preconceptional primary care and healthy food options).8,21 The racial disparity in HDP is a socially structured phenomenon, influenced by both historical processes of racism and contemporary consequences and processes maintaining racial health inequities.22
Conceptualizing risk factors such as HDP as intermediates on the causal pathway from racism to SMM motivates the application of causal mediation analysis for decomposing disparities.23 One challenge of applying these methods in racial disparities research is the expectation of intervention on the mediator and the exposure, of which the latter cannot be readily modified (i.e., historical and contemporary racism). However, a counterfactual disparity measure framework adapts causal mediation methods to shift the focus to the mediator, in this case HDP, to estimate the residual magnitude of the disparity that does not operate through the evaluated mediator pathway.23 Application of a counterfactual disparity measure framework for investigating SMM racial disparities can inform the long-term intervention opportunities for the root and midstream manifestations of racism by estimating the remaining effect of racism on SMM, and more immediately for HDP by estimating the degree to which control of HDP would reduce the Black–White racial disparity.23 Despite its potential value for advancing birthing health equity, to our knowledge no studies have employed causal mediation methods to explicitly investigate the role of individual-level factors in mediating the SMM racial disparity. This study aims to estimate the proportion of the Black–White racial disparity in SMM risk explained through pathways including HDP using causal mediation models.
METHODS Study PopulationWe used Georgia hospital discharge and vital statistics records available to the Georgia Department of Public Health. Conceptualization of HDP on a pathway from structural risk factors to excess SMM risk motivates the use of Georgia population-based data given the prevalence of structural risk factors in the southern US. Contextually, Georgia has a long history of structural racism with substantial geographic and socioeconomic variation among NH Black birthing persons. Practically, Georgia population-based data provide adequate clinical and diagnostic detail to identify SMM and HDP and incorporate multilevel social determinants of health necessary to rigorously investigate the role of HDP in mediating the Black–White racial disparity in SMM risk.
We defined our study cohort as NH Black and NH White Georgia residents age 15–49 years who had any delivery hospitalization record in a Georgia hospital discharged between January 1, 2006 and December 31, 2019. We identified pregnancies using the US Centers for Disease Control and Prevention (CDC)/Alliance for Innovation in Maternal Health (AIM)-recommended ICD-9/10-CM hospital discharge birth denominator codes for the study of SMM (eAppendix 1; https://links.lww.com/EDE/C77).16 Pregnancies could have resulted in a live birth or stillbirth (fetal death ≥22 weeks gestation), but molar and ectopic pregnancies, spontaneous abortions (fetal death <22 weeks), and induced terminations were excluded.16 Pregnancies, not individuals, define our cohort. Thus, a single individual could have multiple SMM events over different pregnancies.
Identifying SMMWe identified SMM events using the CDC/AIM v6-27-2020 list of SMM-defining ICD-9/10-CM (eAppendix 2; https://links.lww.com/EDE/C77).24,25 Our SMM case definition excluded the blood transfusion indicator and included postpartum hospitalizations through 42 days postpartum. Blood transfusion was excluded given the low positive predictive value and variable sensitivity of this indicator for identifying SMM events in hospital discharge records.26–30
Decomposition Analysis Causal Effect Definition and AssumptionsOur goal was to estimate the proportion of the absolute NH Black–White racial disparity RD in SMM that does not operate through the evaluated mediator pathway (HDP), specifically, the counterfactual disparity measure.23 The RD was selected to measure the excess burden, which has advantages in applied epidemiology for interpretability and quantifying the potential public health impact.31 If validly estimated, the counterfactual disparity measure is interpretable as the excess risk of SMM among NH Black pregnancies per 10,000 delivery hospitalizations remaining if the mediator was set to the referent value (no HDP) (Equation 1)23,32:
CDM(HDP=No) =E[SMM(HDP=No) RACE=NH Black] −E[SMM(HDP=No)|RACE=NH White]
In our study, the operationalized exposure of race captures the consequences of structural racism and the lived experiences that differ by race. Note that the proxy of individual race is imperfect; we cannot disentangle the effects of structural racism from other lived experiences captured by race (e.g., individual-level experiences of racism).33
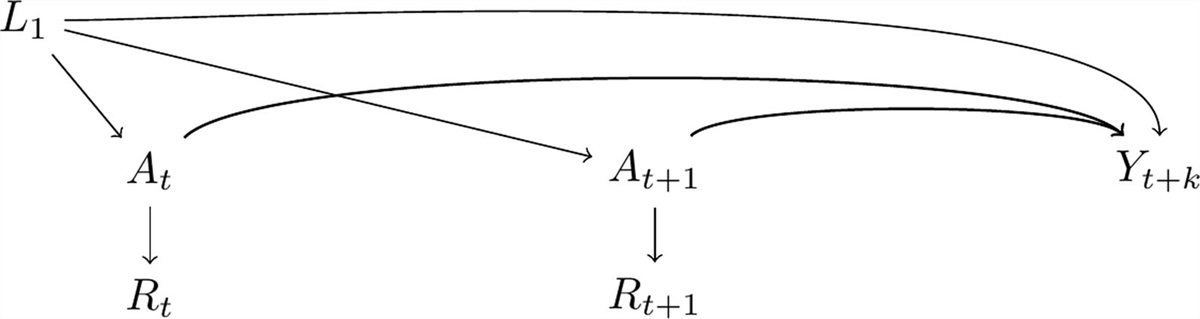
The counterfactual disparity measure can be estimated using causal decomposition analysis.32 We considered four assumptions specific to the decomposition methods used to estimate the measure: (1) No unmeasured exposure–outcome confounding, (2) No unmeasured mediator–outcome confounding, (3) No unmeasured exposure–mediator confounding, and (4) No mediator–outcome confounding affected by the exposure (eAppendix 3; https://links.lww.com/EDE/C77).34,35 Valid estimation of the counterfactual disparity measure only requires assumptions #1 and #2 to be met.32 However, whether assumption #4 is met or not guides the choice of decomposition methods. Adjustment for mediator–outcome confounding using standard regression methods blocks a nonmediated path if assumption #4 is violated. In our study, a path from racism to SMM that does not operate through HDP would be blocked (Figure and eAppendix 3; https://links.lww.com/EDE/C77).32 The mediation-specific assumptions are in addition to the standard assumptions needed for estimating a causal effect.32 These include the stable unit treatment value assumption, consistency (no variations in the potential outcome under the same treatment), positivity (nonzero probability of exposure and covariate for all outcome strata), no measurement error, and correctly specified models.32,36,37
 FIGURE.:
FIGURE.: Hypothesized relationship of race (proxy for racism, sociocultural factors), HDP, SMM, and HDP-SMM (mediator–outcome) confounders. HDP, hypertensive disorders of pregnancy; SMM, severe maternal morbidity.
Exposure and MediatorRace was coded as NH Black or NH White based on information from the hospital discharge record. If race was available and no ethnicity information was available, individuals were assumed to be NH (eAppendix 4; https://links.lww.com/EDE/C77). HDP (mediator) was identified in hospital discharge records based on ICD-9/10-CM codes for chronic hypertension, gestational hypertension, preeclampsia (mild, severe, and unspecified), and hemolysis, HELLP (eAppendix 5; https://links.lww.com/EDE/C77). We grouped chronic and gestational hypertensive codes in this analysis because of similar expected public health implications under the study objective: targeting social determinants of HDP and direct clinical intervention at pregnancy-related points of care. We evaluated a second scenario of the complete prevention of severe HDP defined as severe preeclampsia and HELLP, given a plausible clinical objective of prevention of the progression of chronic and milder forms of HDP to severe HDP.
CovariatesModels were adjusted for measured HDP-SMM (mediator–outcome) confounders based on our hypothesized directed acyclic graph (DAG) (Figure). Covariates included age, multiple gestations, diabetes, gestational diabetes, obesity, kidney disease, insurance payor, adequacy of prenatal care (Kotelchuck index), census tract proportion of the population living below the federal poverty line, and county-level urbanicity.19,38–40 We did not adjust for age given our conceptualization that some of the racialized differences in lived experience, such as age at delivery, are potential consequences of exposure to racism and may shape a birthing person’s SMM risk. When investigating the mediator severe HDP, we adjusted for the same covariates and nonsevere HDP outcomes as described by the DAG in eAppendix 4; https://links.lww.com/EDE/C77. The operationalization of these variables is also described in eAppendix 4; https://links.lww.com/EDE/C77.
We do not conceptualize assumption #1 as a threat to validity when the exposure is race (racism), given no covariate is hypothesized to cause race (Figure). We hypothesized that all measured mediator–outcome confounders were descendants of the exposure, violating assumption #4. We further hypothesized that there were mediator–outcome confounders that were unmeasured, unavailable, or poorly measured in our dataset (e.g., substance use, health behaviors, and other unknown factors).
We imputed covariates with missing values using additive regression, bootstrapping, and predictive mean matching, which assumes covariates are missing at random.41 These included imputation of multiple gestation (n = 127,808; 9%), insurance payor (n = 4,741; 0.3%), adequacy of prenatal care utilization (Kotelchuck index) (n = 384,661; 27%), and census tract poverty (n = 88; 0.001%). We described patterns of missingness by individual-level race and SMM status and compared the results using imputed data to complete case analyses in eAppendix 6; https://links.lww.com/EDE/C77.
G-Estimation of Structural Nested Mean ModelsG-estimation of a structural nested mean model was selected over other generalized methods (e.g., inverse probability-weighted marginal structural models and structural transformation) because the mediator–outcome model is doubly robust.23,34 We first estimated the magnitude of the total absolute Black–White disparity (i.e., the total effect of racism on SMM). G-estimation of a structural nested mean model to estimate the counterfactual disparity measure is a two-step process (eAppendix 3; https://links.lww.com/EDE/C77). In step one, we transformed the SMM outcome to remove the effect of HDP (setting HDP = No). In step two, we estimated the effect of race on the transformed SMM outcome (i.e., the effect of racism on SMM not through HDP). We used the standard error of the counterfactual disparity measure to calculate conservative 95% confidence intervals (CI). We calculated the proportion of the disparity eliminated by the complete prevention of HDP as the total effect minus the counterfactual disparity measure, divided by the total effect. Example R code is publicly available at: https://github.com/Katie-Labgold/Decomposing_SMM_Racial_Disparity. The Georgia Department of Health determined this activity to be consistent with public health practice, which does not require informed consent or IRB approval.
Hypothesizing About the Processes Producing Black–White Racial Disparities in SMM Risk Through HDPIf HDP is an important driver of the Black–White racial disparity, we are interested in hypothesizing about the processes producing this disparity. Two hypothesized scenarios are whether the race-specific differences in SMM risk are driven by differences in the prevalence of the mediator (e.g., a greater proportion of NH Black birthing people have uncontrolled HDP) or a difference in the strength of association of HDP and SMM for NH Black versus NH White birthing people (e.g., the interaction of individual-level race and the HDP). We compared the prevalence difference of HDP by individual-level race (i.e., the prevalence of HDP among NH Black minus the prevalence among NH White birthing people). Further, we compared whether the estimated effect of HDP on SMM risk differed by individual-level race and estimated the counterfactual disparity measure under the scenario of all individuals having HDP.
RESULTSBetween 2006 and 2019, there were 623,402 delivery hospitalizations among NH Black birthing people and 820,769 delivery hospitalizations among NH White birthing people in Georgia (Table 1). Compared with White birthing people, a greater proportion of Black birthing people were ages 24 or younger (42% vs. 30%), Medicaid insured (66% vs. 37%), received inadequate prenatal care (17% vs. 8%), and lived in an urban county (84% vs. 74%). The median proportion of individuals living below the federal poverty line was higher and more variable for NH Black birthing people’s residential census tracts (17%, interquartile range [IQR] = 10, 26) compared with NH White birthing people’s tracts (9%, IQR = 5, 16).
TABLE 1. - Sociodemographic and Clinical Characteristics of Birthing People Stratified by Individual-level Race and Ethnicity, Georgia, 2006–2019 NH Black NH White, N (%) N = 623,402 N = 820,769 HDP, N (%) Any HDP 77,515 (12%) 76,308 (9%) Chronic hypertension 28,782 (5%) 17,977 (2%) Gestational hypertension 20,501 (3%) 28,859 (4%) Preeclampsia (mild, severe, unspecified); HELLP 29,901 (5%) 30,984 (4%) No HDP 545,887 (88%) 744,461 (91%) Age, N (%) 15–19 years 73,429 (12%) 60,307 (7%) 20–24 years 188,175 (30%) 185,126 (23%) 25–29 years 167,665 (27%) 238,475 (29%) 30–34 years 117,695 (19%) 213,972 (26%) 35–39 years 60,898 (10%) 101,373 (12%) 40–44 years 14,623 (2%) 20,318 (2%) 45–49 years 917 (<1%) 1,198 (<1%) Insurance payor, N (%) Private 171,570 (28%) 451,977 (55%) Medicaid 410,748 (66%) 307,618 (37%) Self-pay 14,067 (2%) 11,462 (1%) Other 25,178 (4%) 46,810 (6%) Missing 1,839 (<1%) 2,902 (<1%) Multiple gestation, N (%) Single 553,916 (89%) 737,461 (90%) Multiple 11,465 (2%) 13,521 (2%) Missing 58,021 (9%) 69,787 (9%) Gestational diabetes, N (%) Yes 19,065 (3%) 28,725 (3%) No 604,337 (97%) 792,044 (97%) Preexisting diabetes, N (%) Yes 5,789 (1%) 5,496 (1%) No 617,613 (99%) 815,273 (99%) Renal disease, N (%) Yes 1,337 (<1%) 1,756 (<1%) No 622,065 (99%) 819,013 (99%) Obesity, N (%) Underweight/healthy 584,717 (94%) 789,230 (96%) Overweight/obesity 38,685 (6%) 31,539 (4%) Prenatal care (Kotelchuck index), N (%) Inadequate 107,118 (17%) 66,660 (8%) Intermediate 48,817 (8%) 62,345 (8%) Adequate 146,682 (24%) 247,505 (30%) Adequate plus 147,849 (24%) 232,534 (28%) Missing 172,936 (28%) 211,725 (26%) County urbanicity, N (%) Urban 520,701 (84%) 606,204 (74%) Rural 102,701 (16%) 214,565 (26%) Percentage of individuals living below the poverty line in residential census tract Median (IQR) 17% (10, 26) 9% (5, 16)HDP indicates hypertensive disorders of pregnancy; IQR, interquartile range; NH, non-Hispanic; SMM, severe maternal morbidity.
The SMM rate was 132.8 per 10,000 delivery hospitalizations among NH Black birthing people and 77.1 per 10,000 among NH White birthing people (Table 2). Overall, Black birthing people experienced an excess of 56 SMM events (95% CI = 52, 59) per 10,000 delivery hospitalizations compared with White birthing people (i.e., the total effect). Given our assumptions under the scenario of no HDP, the magnitude of the SMM rate for NH Black birthing people was reduced to 107, and for NH White was reduced to 66 per 10,000 delivery hospitalizations. Thus, the absolute disparity remaining after blocking the pathways through HDP was 41 SMM events per 10,000 delivery hospitalizations (95% CI = 38, 44). Comparing the total disparity and the estimated CDM suggests that if there are no causal pathways open through HDP, 26% (95% CI = 12, 40) of the absolute racial disparity would be eliminated. The magnitude of the estimated proportion eliminated was greater in the complete case analysis (37%) (eAppendix 6; https://links.lww.com/EDE/C77).
TABLE 2. - The Observed and Counterfactual Race-specific SMM Rates, the Total Disparity, Estimated CDM, and Proportion of the Disparity Eliminated for the Effect of Race and SMM Through the Mediator HDP NH Black SMM Ratea NH White SMM Ratea Black–White Rate Differencea (95% CI) Observed SMM 133 77 Total disparity 56 (52, 59) Counterfactual SMMb 107 66 CDM (HDP = No) 41 (38, 44) Percent decrease in race-specific rate 19% 14% Proportion of the disparity explained by HDP 26% (12, 40)aPer 10,000 delivery hospitalizations.
CI indicates confidence interval; HDP, hypertensive disorders of pregnancy; NH, non-Hispanic; SMM, severe maternal morbidity.
When focusing only on the prevention of progression to severe HDP, we estimated that the magnitude of the SMM rate for Black birthing people would be reduced to 124 and for White birthing people to 72 per 10,000 delivery hospitalizations (Table 3). Under the same assumptions, the remaining absolute disparity was estimated as 51 excess SMM events per 10,000 delivery hospitalizations (95% CI = 48, 54) among NH Black birthing people suggesting 8% (95% CI = 0, 19) of the total disparity would be eliminated if there were no open causal pathways through severe HDP.
TABLE 3. - The Observed and Counterfactual Race-specific SMM Rates, the Total Disparity, Estimated CDM, and Proportion of the Disparity Eliminated for the Effect of Race and SMM Through the Mediator Severe HDP NH Black SMM Ratea NH White SMM Ratea Black–White Rate Differencea (95% CI) Observed SMM, n 133 77 Total disparity 56 (52, 59) Counterfactual SMMb, n 124 72 CDM (severe HDP = No) 51 (48, 54) Percent decrease in race-specific rate 7% 6% Proportion of the disparity explained by severe HDP 8% (0, 19)aPer 10,000 delivery hospitalizations.
CI indicates confidence interval; HDP, hypertensive disorders of pregnancy; NH, non-Hispanic; SMM, severe maternal morbidity.
We estimated that the prevalence of HDP among NH Black birthing people (12%) was 3% higher than the prevalence of HDP among NH White birthing people (9%) (Table 4). Further, there was evidence of effect modification on the additive scale for the effect of HDP on SMM by individual-level race. Specifically, birthing people of NH Black race and ethnicity with HDP had 203 excess SMM events (95% CI = 191, 216) per 10,000 delivery hospitalizations compared with Black birthing people without HDP (Table 4). NH White birthing people with HDP had 112 excess SMM events (95% CI = 102, 121) per 10,000 delivery hospitalizations, compared with White birthing people without HDP.
TABLE 4. - Effect Modification Assessment of HDP Status on SMM Risk by Individual-level Race and Ethnicity, the Controlled Direct Effect (CDM) With and Without HDP, and Proportion of Race-specific Deliveries With HDP No HDP HDP RDa per 10,000 Deliveries for HDP in Strata of Individual-level Race/Ethnicity N (SMM/Deliveries) Proportion of Deliveries N (SMM/Deliveries) Proportion of Deliveries NH White 4,838/744,461 91% 1,490/76,308 9% 112 (102, 121) NH Black 5,681/545,887 88% 2,596/77,515 12% 203 (191, 216) CDM (HDP = 0)a 41 (38, 44) CDM (HDP = 1)a 129 (126, 132)aRD and CDM estimates adjusted for insurance payor, age, multiple gestation, preexisting diabetes, gestational diabetes, renal disease, obesity, prenatal care, and proportion of residential census tract living below the federal poverty line.
CDM indicates counterfactual disparity measure; CI, confidence interval; HDP, hypertensive disorders of pregnancy; NH, non-Hispanic; SMM, severe maternal morbidity.
Our primary interest was in estimating the counterfactual disparity measure for no HDP to inform our understanding of how much of the disparity in SMM would be reduced if the impact of HDP on SMM risk was eliminated, which yielded an estimated disparity of 41 SMM events (38, 43) per 10,000 delivery hospitalizations. The counterfactual disparity measure can also be estimated for the scenario in which all individuals had HDP to further elucidate how HDP may be contributing to the Black–White racial disparity in SMM risk. Under this scenario, we observed that the Black–White disparity would be 129 SMM events (126, 132) per 10,000 delivery hospitalizations (Table 4). An estimated Black–White SMM racial disparity under the scenarios in which everyone had HDP that is more than double the observed total disparity if no birthing people had HDP supports that the effect of HDP on SMM risk is stronger for NH Black compared with NH White birthing people.
DISCUSSIONHDP is a known cause of SMM and maternal mortality overall, with the greatest HDP prevalence in the southern US.10,12,17,20 In our study, decomposition of the absolute NH Black–White racial disparity in SMM using G-estimation of a structural nested mean model estimated that if HDP was no longer a pathway to SMM, the NH Black–White racial disparity in SMM would be reduced by 26% (Table 2). Yet if our assumptions hold, we estimated that a large magnitude of the Black–White racial disparity would remain under a scenario in which HDP was completely eliminated or controlled (74%).10,11
As noted previously, preventing progression to severe HDP is of potential clinical interest. Our results suggest that if we focus only on the complete elimination of severe HDP, the NH Black–White racial disparity in SMM would be reduced by 8%. This finding considered in the context of the differences in prevalence of specific HDP diagnoses by race (Table 1) and analysis of all HDP (Table 2) is consistent with the hypothesis that the largest drivers of the Black and White absolute disparity in SMM through HDP may be driven by chronic HDP, reemphasizing the call for investigating and targeting upstream causes of SMM risk.
Our results suggest that both differences in the prevalence of the mediator in each racial group and the interaction of race (racism) and HDP may be important mechanisms of the excess SMM risk among NH Black birthing people through HDP, given our assumptions (Table 4). These findings are consistent with the hypothesis that reducing the prevalence of HDP overall would reduce some of the Black–White racial disparity in SMM risk. However, a focus on reducing the prevalence of HDP through HDP prevention and treatment would likely be insufficient for remediating the racial disparity without further consideration of how differences in contextual- and individual-level experiences among Black birthing people produce elevated SMM risk through HDP compared with NH White birthing people.
The finding that the association of HDP on SMM risk was stronger for NH Black birthing people compared with NH White birthing people is consistent with our conceptualization that the inequitable excess risk among Black pregnancies operating through HDP may be driven by structural racism (Table 4).8,42 Structural racism produces differential access to healthcare systems such as quality primary care, prenatal care, and postpartum care, and neighborhood factors such as safety (influencing stress, allostatic load, and therefore increasing HDP risk), the availability of affordable healthy food options, green space, and educational opportunities.8,43,44 For example, among HDP indicators, the greatest Black–White prevalence difference was observed for chronic hypertension (Table 1). Results from mediation analyses and the effect modification assessment are consistent with a hypothesis that failed periconceptional and life course primary care, and differential access to healthy environments, are contributing to the excess risk among Black pregnancies.14 Findings are further consistent with a hypothesis that a greater proportion of NH Black birthing people entering into pregnancy with chronic cardiometabolic disease, putting them at an increased risk of SMM (Table 4). This is especially true if chronic hypertension is not recognized and properly managed because of structural constraints (e.g., insurance status before pregnancy, affordability of antihypertensive medication, inaccessibility to healthy food options, lack of green space or time for physical activity).14
Improving our understanding of the pathways of structural racism to SMM through HDP allows us to identify clinical and social determinants of health opportunities to reduce Black–White disparities in SMM risk. Although HDP is a meaningful opportunity for intervention, our results elucidate that focusing solely on HDP (under a scenario of the complete elimination of HDP) would still result in almost three-quarters of the Black–White disparity remaining (Table 2). Other pathways must be investigated and subsequently intervened upon to achieve health equity in birthing health ou
留言 (0)