
Remember me
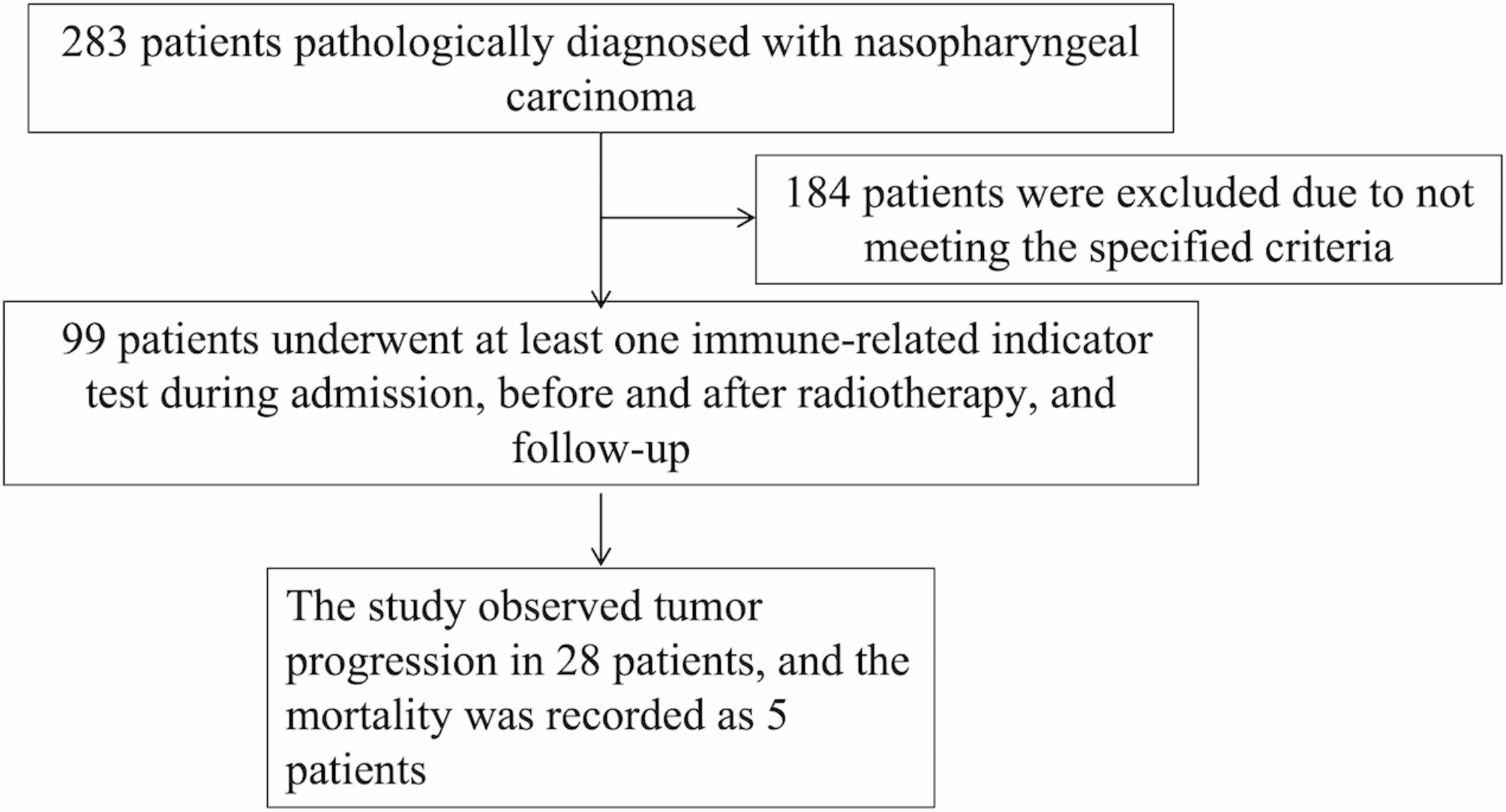
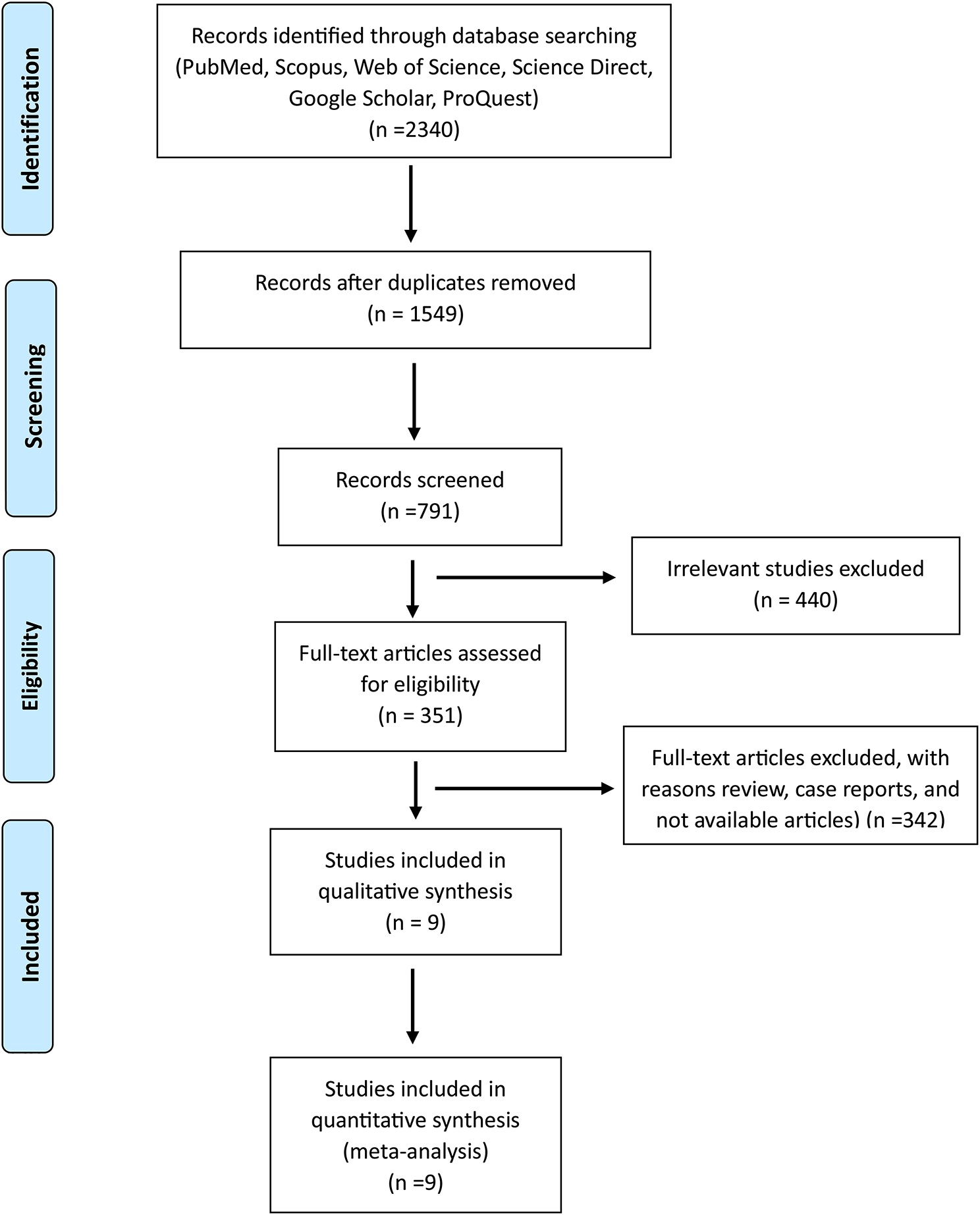





A flow scheme of the study is shown in Fig. 1. Pathology results for 82 samples were as follows: ≤ CIN1, n = 24 (29.3%); CIN2, n = 10 (12.2%); CIN3, n = 23 (28.0%); and CC, n = 25 (30.5%). DNA isolated from 82 cervical scrapes was bisulfite-treated and tested in MSP experiments for the 16 candidate DNA methylation markers GFRA1, MIR124-2, ASCL1, CCDC181, EPB41L3, JAM3, PAX1, SORCS1, PCDHA13, LOC100289333, BOLL, FAM19A4, MIR129-2, ZIC1, SOX1 and SST. There were 5 genes with AUCs greater than or equal to 0.8 (AUC ≥ 0.8) showing a distinction between CIN2- and CIN3+ in cervical scrapings (Fig. 2), which were validated next. The AUCs of MIR124-2, JAM3, LOC100289333, ZIC1, and SOX1 were 0.856 (95% CI 0.770–0.942), 0.800 (95% CI 0.701–0.898), 0.822 (95% CI 0.726–0.919), 0.839 (95% CI 0.751–0.928) and 0.814 (95% CI 0.720–0.909), respectively. The cutoff values corresponding to the above five genes were 9.89, 9.22, 6.2, 3.29 and 5.25, respectively (Additional file 1: Table S2). The positive rates of 16 candidate genes in the training set are shown in Additional file 1: Fig. S1. Eleven genes were excluded from further analysis.
Fig. 1
Flow scheme for the identification of the CIN3+ methylation marker. AUC, area under the curve; hrHPV, high-risk HPV
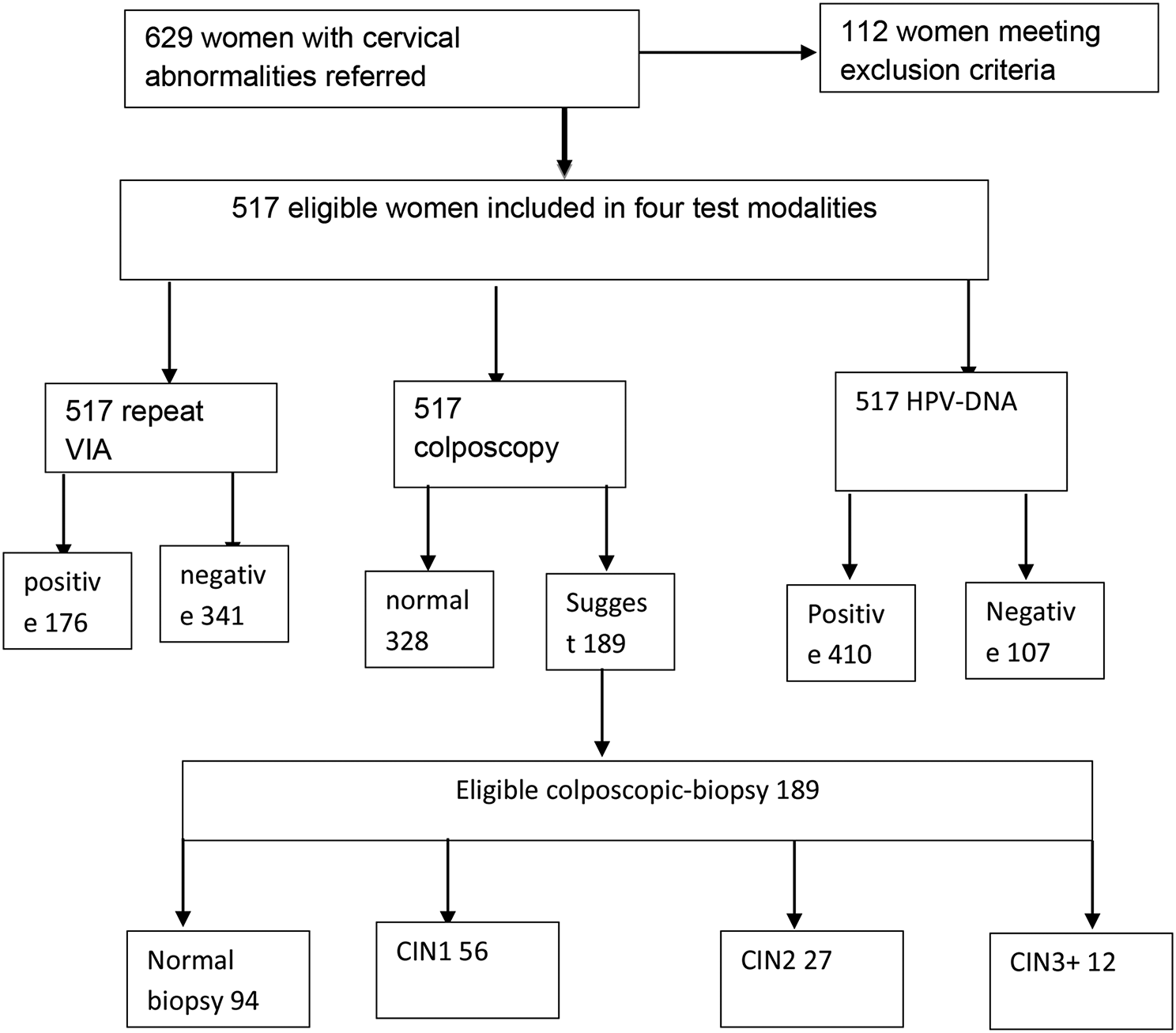
Fig. 2
ROC curves and corresponding AUCs of candidate gene DNA methylation markers differentiated between CIN2- and CIN3+ detection. Power the methylation of 16 candidate genes in differentiating CIN3+ from CIN2- subjects. AUC, area under the curve; CI, confidence interval
Patients and histological outcomesThe clinicopathological data and cytology results of the validation cervical scrapes are summarized in Table 1. Pathology results for 74 samples were as follows: ≤ CIN1, n = 47 (63.5%); CIN2, n = 13 (17.6%); CIN3, n = 6 (8.1%); and CC, n = 8 (10.8%). CIN3+ subjects (average age 54.3 years) were older than CIN2- subjects (average age 43.0 years) (p < 0.05). The cytology results included 51 (68.9%) cases of NILM, 8 (10.8%) cases of ASC-US, 1 (1.4%) case of LSIL, 3 (4.1%) cases of ASC-H, and 11 (14.9%) cases of HSIL. Cytological results showed that NILM constituted 86.3% of ≤ CIN1 and ASC-US constituted 62.5% of CIN2, while HISL constituted 45.4% of cancer.
Table 1 Clinicopathological data of validation samplesClinical performance of five DNA methylation markers in the validation setFive genes selected from the training set were validated with 74 cervical scrapings (Fig. 3). The positivity rate of HPV16/18 and methylation raised with increased pathological grade. Compared to the results of cytology (sensitivity: 71.4%, 95% CI 42.0–90.4%; specificity: 78.3%, 95% CI 65.4–87.5%), the sensitivity of hrHPV (92.9%, 95% CI 64.2–99.6%) was significantly higher with a slightly lower specificity (76.7%, 95% CI 63.7–86.2%), and the sensitivity of HPV16/18 genotyping (50.0%, 95% CI 24.0–76.0%) was lower with a higher specificity (95.0%, 95% CI 85.2–98.7%). Overall, methylation rates ranged from 16.7% to 66.7% for CIN3 and from 75.0% to 100.0% for cervical cancer. Single methylation of LOC100289333 (LOC100289333m), ZIC1 (ZIC1m) and SOX1 (SOX1m) tested positive in all cervical cancer scrapings. The new cutoff values in the validation set were recalculated from 156 subjects. The AUCs of LOC100289333m, ZIC1m, and SOX1m that distinguished CIN2- and CIN3+ in the validation set were still greater than 0.8, with 0.862 (95% CI 0.744–0.980), 0.835 (95% CI 0.700–0.969) and 0.879 (95% CI 0.763–0.994) by the new cutoff values of 6.27, 3.29 and 5.25, respectively. The AUCs of MIR124-2m and JAM3m were less than 0.8, with 0.763 (95% CI 0.605–0.922) and 0.750 (95% CI 0.576–0.924), respectively, resulting in exclusion from further analysis (Table 2). LOC100289333m and SOX1m, compared with ZIC1m (78.6%, 95% CI 48.8–94.3%), had better clinical performance, and which sensitivity was greater than 85% (85.7%, 95% CI 56.2–97.5%). However, SOX1m had higher specificity (90.0%, 95% CI 78.8–95.9%) than LOC100289333m (86.7%, 95% CI 74.9–93.7%).
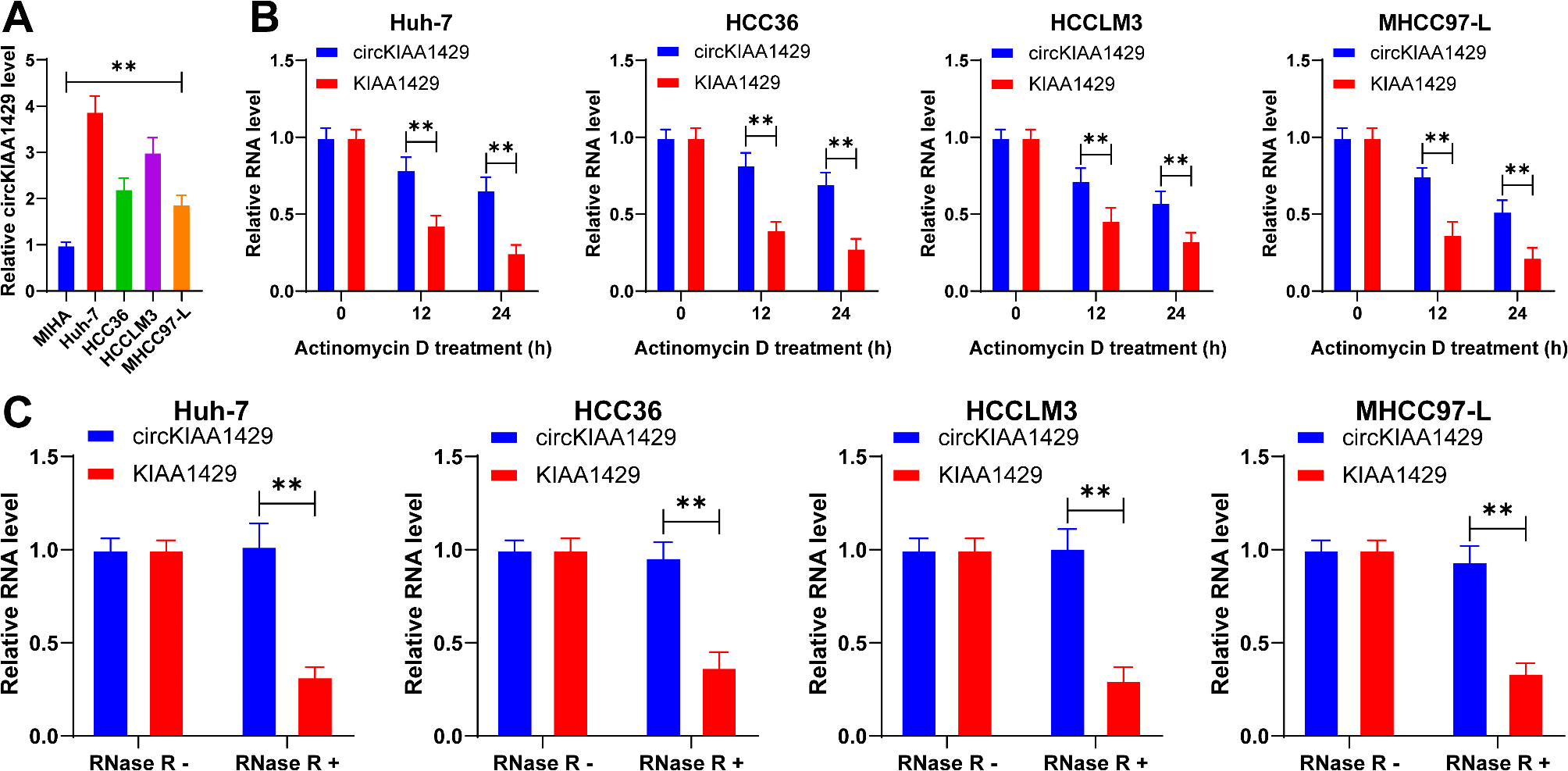
Fig. 3
hrHPV positivity and methylation positivity of five genes in cervical scrapings (n = 74). The distribution of the methylation positivity of the five selected markers in the ≤ CIN1, CIN2, CIN3, and CC groups
Table 2 Sensitivity and specificity of cytology, hrHPV, HPV16/18 genotyping and DNA methylation for detecting CIN3+ DNA methylation markers for the triage of hrHPV-positive womenForty-four of 74 (59.5%) subjects were hrHPV positive, with HPV16/18 positivity constituting 36.5% and non-16/18 hrHPV positivity constituting 23.0% of all subjects (Fig. 4). HPV16/18 genotyping was used to triage hrHPV-positive scrapings, and subjects with HPV16/18 positivity were referred directly to colposcopy. Among HPV16/18-positive women, 8 cases of CIN3+ (3 cases CIN3 and 5 cases CC) were detected, and 3 cases of CIN2- (1 case CIN1 and 2 cases CIN2) were overtreated. The rate of referral for colposcopy was 18.9% in non-16/18 hrHPV (+) plus cytology (≥ ASC-US) subjects. Thus, when cytology was applied as a screening strategy for hrHPV (+), the overall rate of referral for colposcopy was 31.4%, at which point the number of overtreatments was 13, and the number of missed diagnoses was 1 CIN3 and 1 CC (Fig. 4A). LOC100289333m, ZIC1m, or SOX1m in hrHPV-positive women was evaluated, with colposcopy referral rates of 20.3%, 20.3% or 23.0% and missed diagnoses in subjects with two, two or one CIN3 cases (Fig. 4B, D).
Fig. 4
Cytology and methylation tests for the triage and management of hrHPV-positive women in the Chinese cohort. Outcomes of the triage chart are shown for TCT (A), LOC100289333m (B), ZIC1m (C), and SOX1m (D). TCT, Thinprep liquid-based cytology test
Comments (0)