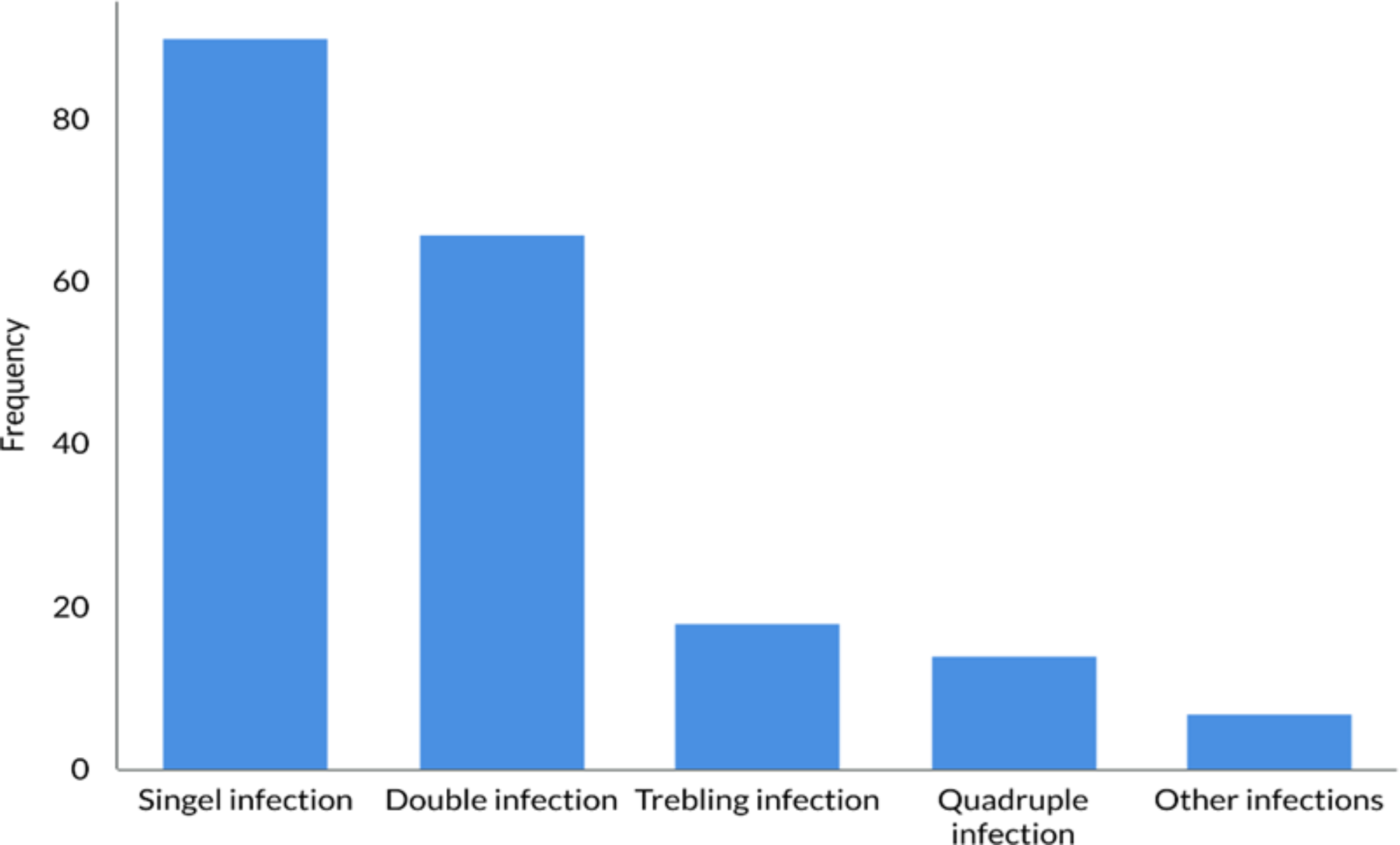
This study offers an up-to-date analysis of HPV genotype distribution among men and women in Urmia. Between 2022 and 2023, a total of 447 individuals, comprising 431 females and 16 males, were referred to the laboratory. Among them, 195 were diagnosed with HPV, indicating an overall infection rate of 43.6% (42.5% in females and 75.0% in males). The highest rate of positive cases occurred in individuals under 30 (47.5%) and those aged 31–40 (42.7%). As well, the cases were categorized into two groups: individuals who underwent a Pap smear and those who did not. As shown in our results, the prevalence of HPV had no statistically significant difference between two each group. Additionally, a notable percentage of HPV-positive individuals had infections with multiple genotypes. Of the total positive cases, 90 (46.2%) had a single HPV genotype, while 105 (53.8%) were infected with two or more genotypes. The most common types identified were LR-HPV6, HR-HPV16, HR-HPV56, and HR-HPV90.
A systematic review and meta-analysis that evaluated 26 eligible studies with a total sample size of 5,560 women revealed an overall HPV prevalence of 23% among Iranian women. The highest prevalence was observed in Tehran, while the lowest prevalence was found in Isfahan [22]. In alignment with our results, a study conducted in Tehran on 219 HPV-positive cases (160 females and 59 males) found that HPV-16 (17.4%) was the most prevalent HR type, and HPV-6 was the most common LR type [23]. However, contrary to our findings, this study indicated that the prevalence of HR-HPV was greater than that of LR-HPV in their population [23]. Another study conducted in Tehran aimed at analyzing the molecular characteristics of HPV genotypes among 5,176 male and female patients revealed that 2,727 (53%) tested positive for HPV [24]. Of these, 2,372 (87%) were women, and 355 (13%) were men. In line with our findings, the survey recognized HPV-6 as the most predominant LR type (32% in females and 31% in males) and HPV-16 as the most common HR type (12% in females and 11% in males). The highest frequency of HPV was observed in the 31–40 and 21–30 age groups. Additionally, a significant proportion of the study population, 1,306 patients (52%), were found to have infections with multiple genotypes, similar to what we observed in this research [24]. In the largest survey conducted in Iran, which analyzed 10,266 samples from 31 provinces, Mobini Kesheh et al. reported that 49.5% (n = 5085) tested positive for HPV DNA [13]. Similar to our findings, the most frequent LR-HPV type identified was HPV-6 (77.7% in males and 43.3% in females), while the most common HR type was HPV-16 (5.5% in males and 16.6% in females). Additionally, they observed mixed HPV infections in 14.0% of HPV-positive males (n = 174) and 42.2% of HPV-positive females (n = 1620). In line with our findings, HPV-6 was the most frequently detected genotype in mixed infections across both genders. However, unlike our results where HPV-16 was the second most common genotype, their analysis found HPV-11 to be the second most common in cases of mixed infections [13]. Also, the highest HPV burden was found in individuals aged between 30 and 44, accounting for 51.8% of cases [13]. A study conducted in Sari included 90 participants, with 83 women and 7 men. Among the women, 65% (54 out of 83) tested positive for HPV, while all 7 men were positive [25]. Unlike our findings, the most common LR-HPV type was HPV-11 (23%), and the most frequent HR types were HPV-56 (18%) and HPV-39 (16%). In line with our findings, the highest HPV prevalence of 75% (36 cases) was found in individuals under the age of 31. However, unlike our results, most of the positive cases in this age group were associated with HR genotypes [25]. Among individuals with HPV infections, 39 cases (around 61.3%) exhibited co-infections with multiple genotypes. In contrast to our findings, where HPV-6 was the most common genotype in mixed infections, HPV-11 was the most prevalent genotype, appearing in 14 out of 61 cases [25].
In a study by Sabet et al., out of 567 participants in northeast Iran, 35.3% (n = 200) tested positive for HPV [26]. The distribution of HPV genotypes in this population included HPV-6 (50%), HPV-11 (10%), HPV-67 (5%), HPV-16 (15%), HPV-31 (10%), HPV-54 (5%), and HPV-89 (5%). They also observed multiple HPV genotypes in Razavi and North Khorasan, where 11.2% (28/108) had co-infections with two genotypes, 4.8% (12/108) with three, and 0.4% (1/108) with four or more genotypes. In South Khorasan, 3% (6/37) were co-infected with another genotype, while within a more diverse group, 8.6% (10/37) had two-genotype co-infections, 0.9% (1/37) had three, and 1.7% (2/37) had four or more genotypes [26]. In a separate study conducted in Sanandaj, out of 950 participants, 933 (98%) were female, while 17 were male [27]. Within the female group, 236 (25%) tested positive for HPV, whereas among the male participants, 13 out of 17 (76%) were HPV positive. Similar to our findings, the most prevalent HR genotype was HPV-16, and the most common LR genotype was HPV-6. Additionally, the highest percentage of positive HPV cases was seen in individuals under 20 years old (40%) and those aged 21–30 (35%). However, in terms of the total number of HPV-positive individuals, the 31–40 age group had the highest count of cases [27]. Furthermore, few studies have been carried out in Urmia to examine the prevalence of HPV genotypes. In the initial research conducted by Olia et al., focused on determining the HPV genotypes linked to vaginal infections among women, results indicated that 30 out of 80 samples (37.5%), were positive for HPV [14]. Similar to our findings, the majority of cases, 16 people (53.4%), were infected with LR genotypes. In addition, seven patients (23.3%) had infections with HR HPV genotypes, and another seven individuals (23.3%) had co-infections involving both LR and HR genotypes [14]. However, it is important to note that this investigation predominantly focused on female participants and did not include any males in the sample.
Overall, our study emphasizes a significant observation regarding the notably high prevalence of HPV-6 and HPV-16. Although current available vaccines offer good protection against HPV-6 and HPV-16, these remain among the most frequently detected strains in our research. Multiple factors may have contributed to this occurrence. In Iran, the provision of HPV vaccines is managed by private companies, and are not covered by insurance, making them unaffordable for many [28, 29]. Additionally, the vaccine has yet to be integrated into the national immunization schedule, and evidence supporting its cost-effectiveness in Iran is lacking [30, 31, 32]. Other barriers, such as high vaccine prices, financial difficulties, and a lack of public awareness, significantly impede vaccination initiatives [33]. This highlights the critical necessity for comprehensive national initiatives and enhanced regulation to enhance the availability and adoption of the HPV vaccine in Iran. Moreover, although existing vaccines offer strong protection against HPV-6 and HPV-16, they do not include HPV-56, which has become one of the most frequently identified strains in this study. This limitation inn vaccine coverage highlights the urgent need for expanded preventive strategies and enhanced screening initiatives.
It’s essential to recognize certain limitations in our research. Firstly, the majority of contributors were women, with a much smaller sample of men, which may not accurately represent the true epidemiology of HPV. Consequently, these findings are not applicable to men, highlighting the necessity for additional focused studies that incorporate a larger group of male participants in this area. Larger studies with broader sample sizes, especially focused on men, are necessary to better understand the prevalence and impact of HPV infections across different demographics. Secondly, it is essential to acknowledge that these observations may not be applicable to the broader population. This study’s participants were individuals who came to the laboratory expressly for HPV testing, likely due to noticeable symptoms or engagement in high-risk activities. Consequently, the heightened infection rates seen in specific subgroups mirror the characteristics of those actively seeking testing, rather than representing the general population. Another limitation of this study is the lack of DNA genotyping using specific primers (like GP5+/GP6+ ) followed by sequencing, which could have provided valuable data for phylogenetic analysis. Such an analysis would have offered a more detailed understanding of the HPV strains circulating in the region. This limitation highlights the potential for future research to incorporate such analyses to further enhance the understanding of HPV strain distribution. Additionally, the relationship between co-infections and the symptoms and prognosis of patients was not explored in this study. Further investigation into this matter would be valuable in understanding the clinical implications of co-infections. This limitation should be considered, and future studies could focus on the impact of mixed infections on patient outcomes.






Comments (0)