Study population
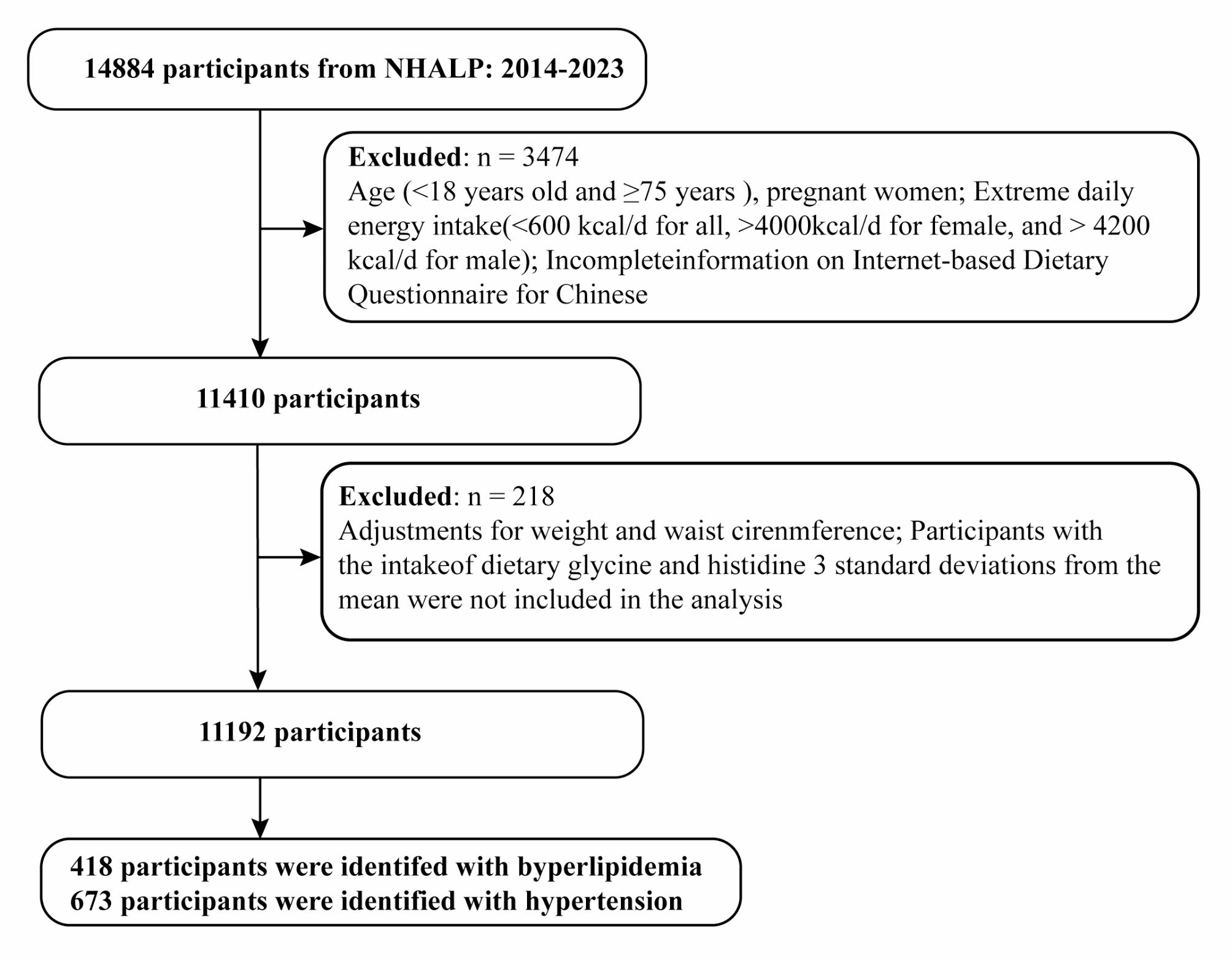
National Health and Nutrition Examination Survey (NHANES) is an ongoing program of studies that combines interviews and physical examinations in the form of a series of surveys, aiming to assess the health and nutritional status of adults and children in the United States. We analyzed data of the NHANES cycles from five study cycles (1999 to 2000, 2001 to 2002, 2003 to 2004, 2011 to 2012, and 2013 to 2014) because both serum B12 and MMA were only measured in those study cycles. Overall, among 26,661 adults aged 20 years, there was a total of 2072 subjects with past histories of CHD. After excluding without serum MMA and B12 measurement (n = 315) and lost to follow-up (n = 2), 1755 eligible patients were included in our analysis.
Study exposure: MMA and vitamin B12
Blood samples were collected via venipuncture, and MMA was determined in plasma and/or serum. MMA level was measured using Gas chromatography-mass spectrometry (GC/MS) for the 1999 through 2004 surveys, and Liquid chromatography-mass spectrometry (LC-MS/MS) for the 2011–2014 surveys. An evaluation of MMA measurement by two methods (n = 326) showed excellent correlation (r = 0.99) and consistency (Deming regression, Bland-Altman analysis) for GC/MS and LC-MS/MS detection, supporting that MMA data measured by both protocols can be combined for analysis.
Serum B12 levels were determined using the Quantaphase II Folate/B12 Radioassay Kit (Bio-Rad Laboratories) between 1999 and 2004, and an automated electrochemiluminescence immunoassay (Elecsys E170; Roche) between 2011 and 2014 in the central laboratory of NHANES. Both assays demonstrated comparable coefficients of variation (< 5%) and limits of detection (20–30 pg/mL). A comparative analysis was conducted in-house on 284 specimens to evaluate any differences between the two assays. To account for errors considered by Deming regression in both methods, B12 values obtained using the Roche assay were converted to Bio-Rad B12 levels based on NHANES recommendations.
Dietary intake was assessed by 24-h food recalls conducted by trained interviewers. From 1999 to 2002, one diet recall was conducted in-person in the Mobile Examination Center; since 2003, the second recall was added via telephone 3 to 10 days later after the first recall and the average of the two dietary recall was adopted to reduce estimation errors [10]. Standard protocols and tools were employed to aid in assessing the volume and dimensions of the food consumed. The Food and Nutrient Database for Dietary Studies was utilized to estimate the nutritional components of the foods [16].
Information regarding the consumption of dietary supplements containing B12 was obtained through standardized questionnaires [16]. All participants were queried about their use of dietary supplements within the previous 30 days. To minimize misclassification errors, the ingredient information was verified by referencing the bottles and labels.
Functional B12 deficiency, characterized by impaired sensitivity to B12 therapy, has been previously defined as MMA > 250 nmol/L and serum B12 > 400 pg/mL [17, 18]. In this study, patients with CHD were categorized into four groups based on the combination of binary serum B12 and MMA, enabling the assessment of B12 sensitivity. The groups included MMAlowB12low (MMA ≤ 250 nmol/L, B12 ≤ 400 pg/mL), MMAlowB12high (MMA ≤ 250 nmol/L, B12 > 400 pg/mL), MMAhighB12low (MMA > 250 nmol/L, B12 ≤ 400 pg/mL), and MMAhighB12high (MMA > 250 nmol/L, B12 > 400 pg/mL).
Covariates
The following variables were collected by standardized questionnaires: age, sex, race/ethnicity, smoking status, alcohol consumption, and physical activity. Race/ethnicity was recorded as non-Hispanic whites, non-Hispanic blacks, Hispanic Mexicans and others. Smoking status was categorized as never, former and current smokers. Former smokers were defined as participants who had ever smoked at least 100 cigarettes but had now quit. Alcohol consumption (g/d) was estimated according to questionnaire. One drink, approximately 10 g of alcohol, was defined as 12-oz beer, 4-oz wine, or 1 ounce of liquor [19]. Leisure physical activity status (inactive, moderate, and vigorous) was determined by the self-reported [19]. Moderate physical activity was defined as leisure activities with a light sweating or a slight to moderate increase in breathing or heart rate in the past month. Vigorous activity was defined as exercise with heavy sweating, or significant increase in breathing or heart rate for at least 10 min [19]. Medications use, including cardiovascular prescriptions ACEI/ARB, β-blocker, diuretics, anti-lipid agents, and anti-platelet agents, and Metformin, during the 30 days prior to the interview was ascertained from self-report [20]. The specific names of prescription drugs were ascertained according to the medication container label, which was linked to standardized generic prescription medication catalogues, as our previously described [21]. Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters) squared. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation. The total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and C-reactive protein were measured as our previous described [9]. Hypertension was defined as antihypertensive prescription medication, systolic BP ≥ 140 mmHg, or diastolic BP ≥ 90 mmHg. Diabetes was defined as treatment with anti-hyperglycemic or HbA1c ≥ 6.5%. Chronic obstructive pulmonary disease (COPD) including chronic bronchitis and/or emphysema were defined according to the self-reported diagnosis [9]. Malignancy or cancer was recorded by a self-report diagnosed by doctor.
Study outcomes
The study endpoints were all-cause mortality, cardiovascular mortality, heart-specific mortality, stroke-related mortality and cancer-related mortality. Mortality status and cause of death were determined by NHANES-linked National Death Index public access files through December 31, 2019. The leading cause of death was identified based on the International Classification of Diseases, 10th Revision (ICD-10), including death due to cardiovascular disease (heart disease: I00-I09, I11, I13, I20-I51, and cerebrovascular disease: I60-I69), malignant neoplasms (C00-C97). Because of International Classification of Diseases, 9th Revision (ICD-9) used prior to 2015, we translated from ICD-9 code to ICD-10 code for further analysis.
Statistical analysis
All analyses were conducted in compliance with the analytical guidelines of the NHANES data set [10]. All estimates are weighted with a raw masked variance of primary sampling unit, pseudo-strata, and appropriate sampling weights to account for complex sampling designs, unless otherwise stated. Continuous variables and categorical variables are expressed as weighted mean (standard error, SE), and weighted percentages, respectively. Participants with CHD were divided into three tertiles groups: T1 (MMA < 120 nmol/L), T2 (MMA 120–216 nmol/L), and T3 (MMA > 216 nmol/L). The trend test was used to analyze the baseline characteristics across MMA groups. Weighted linear regression was used for measurement data, and logistic regression was used for categorical variables.
Estimates of all-cause mortality, cause-specific mortality, and 95% CI are based on the Poisson distribution, where mortality is expressed as the number of deaths per 1000 person-years of follow-up. If an intersection point is identified, we further conducted the Landmark analysis to assess to the mortality risk occurring before and after the intersection point. Unadjusted and multivariate adjusted weighted Cox proportional risk regressions were used to assess the association between MMA, B12-related biomarkers (serum level, dietary intakes, supplements use, and sensitivity to B12), and the risk of mortality. Three adjustment models are used. Model 1 was adjusted for age (years, continuous variables), sex (male, female), and race/ethnicity (non-Hispanic white, black, Hispanic Mexican, or other). Model 2 was additionally adjusted for smoking status (never, ever, or current), physical activity (inactive, moderate, or vigorous), body mass index (< 18.5, 18.5–25, 25–30, or ≥ 30 kg/m2), hypertension (no/yes), diabetes (no/yes), chronic obstructive pulmonary disease (no/yes), cancer (no/yes), total cholesterol (mmol/L, continuous), high-density lipoprotein cholesterol (mmol/L, continuous), C-reactive protein (mg/dL, continuous), Vitamin B12 (B12, continuous), and estimated glomerular filtration rate (mL/min/1.73 m², continuous) were added. Model 3 was additionally adjusted for cardiovascular medications, including metformin (no/yes), ACEI/ARB drugs (no/yes), β-blocker use (no/yes), diuretic drugs (no/yes), anti-lipid use (no/yes) and anti-platelet use (no/yes), was also adjusted. The hazard ratio was calculated using the first group of classification variables (T1) as reference. Models for B12 supplements use were adjusted for dietary B12 intake from foods (continuous) and vice versa.
The association between baseline MMA and all-cause mortality was further stratified into specific subgroups based on age (< 65 years and ≥ 65 years), sex (male/female), current smoking (no/yes), body mass index (< 30 and ≥ 30), diabetes (no/yes) and eGFR (< 60 mL/min/1.73m2 and ≥ 60 ml/min/1.73m2) were grouped. The Survey-Weighted Wald test was used to assess the potential interaction between MMA and stratification factors on the risk of death. ROC curve analysis confirmed the prognostic performance of MMA and other cardiovascular biomarkers in patients with CHD. A two-tailed P value of < 0.05 was considered statistically significant.





Comments (0)