
記住我
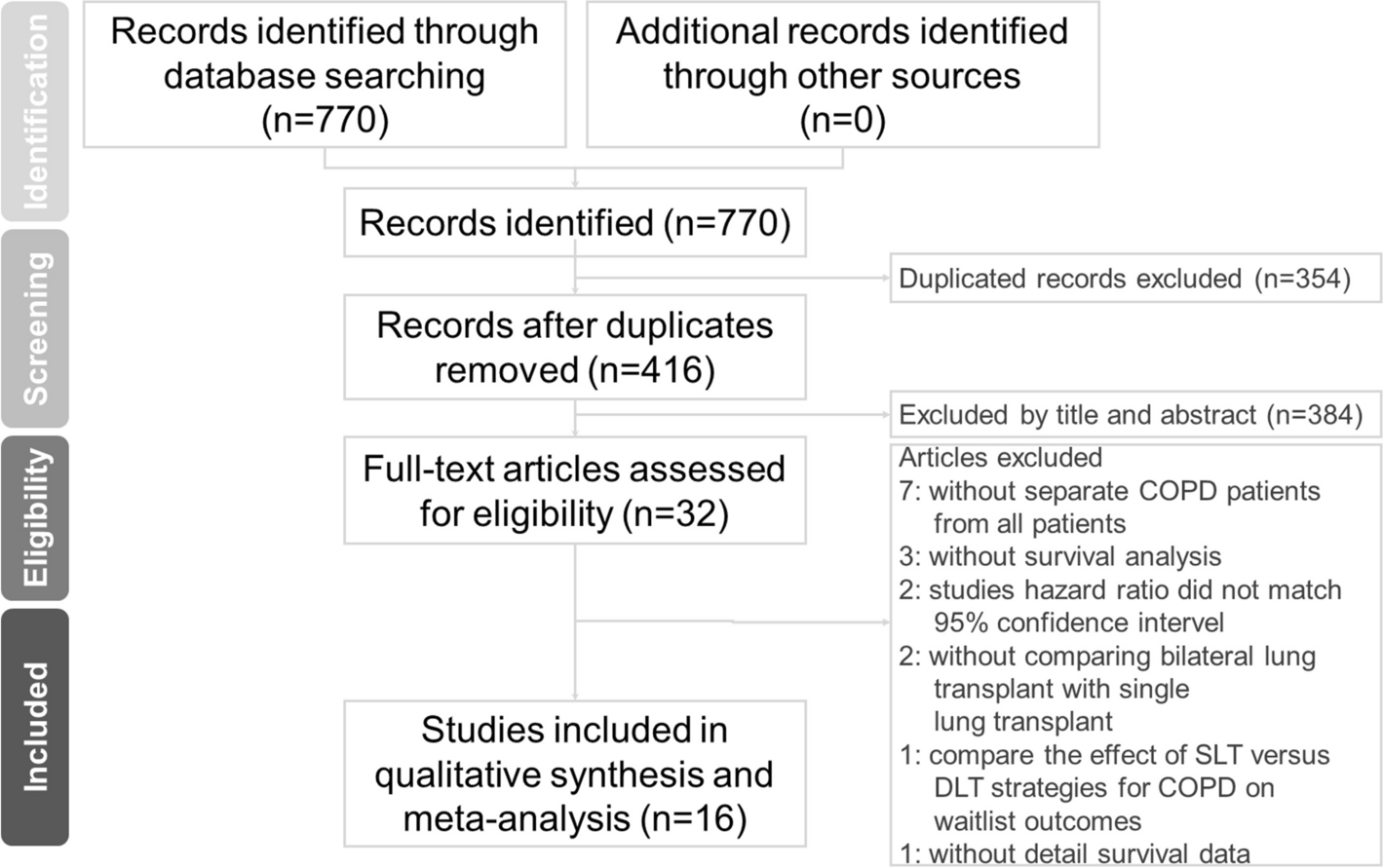





After obtaining Institutional Review Board approval the adult cardiac surgery database of Loma Linda University Medical Center was retrospectively reviewed from January 1, 2019 to July 15, 2022. All patients that underwent isolated coronary artery bypass grafting (CABG) were identified and those with a preoperative left ventricular ejection fraction of 40% or less were included in the study. Patients who underwent off-pump or beating heart CABGs were excluded, the remainder were retrospectively divided between those who received modified del Nido cardioplegia and those who received conventional cardioplegia (Fig. 1). Patients’ electronic medical records were reviewed and baseline characteristics including age, gender, weight, body mass index, ethnicity and comorbidities were documented. Preoperative left ventricular ejection fraction was determined from transthoracic or transesophageal echocardiograms performed prior to induction of anesthesia. In emergency cases where preoperative echocardiograms were not performed we used the intra-operative transesophageal echo that was inserted after induction of general anesthesia. We defined the urgency as cases as follows: elective cases came in from home for their previously scheduled operation, urgent cases were patients admitted to the hospital and required operative intervention prior to discharge and emergency cases were those that required surgery as soon as an operating room was available. When a range in left ventricular ejection fraction was documented we used the average of the range. We reviewed operative notes and intraoperative trans-esophageal echocardiograms to document intraoperative characteristics such as the urgency of the case, number of grafts performed, cardiopulmonary bypass time, aortic cross-clamp (ischemic) time and weaning time (difference between the bypass time and the ischemic time) as well as transfusion requirements and changes in post-reperfusion ventricular function. Incidence of postoperative new-onset atrial fibrillation, intensive care unit (ICU) length of stay (LOS), cumulative postoperative LOS and 30-day mortality were determined from the electronic medical record and recorded.
Fig. 1
Flow diagram of patient enrollment
Surgical technique and myocardial protectionAll operations were performed through a median sternotomy with central cannulation after the conduits were harvested. Patients were placed on cardiopulmonary bypass and cooled to 32–33 °C. Cardioplegia was delivered at 4 °C using the Quest Myocardial Protection System (Quest Medical, Inc., Allen, Texas) which allows for delivery of oxygenated blood from the oxygenator to the heart after addition of additives which differed depending on which cardioplegia strategy (conventional vs. del Nido) was employed. The type of cardioplegia, conventional vs. del Nido was based on the surgeon’s preference. Our del Nido formulation differs from the classical del Nido composition [4] which used a base solution of Plasma-Lyte A (Baxter Healthcare Corporation, Deerfield, IL) to which the cardioplegic additives were added and then this crystalloid component was mixed with blood in a ratio of four parts crystalloid to one part oxygenated whole blood. Our approach was to add the cardioplegic additives (whether conventional cardioplegia or del Nido) directly to the patient’s whole blood rather than in a crystalloid base (Fig. 2).
Fig. 2
Method of mixing the cardioplegia solutions
Components of additives used in each solution are shown in Table 1 (and Fig. 2).
Table 1 Cardioplegia componentsFor the conventional cardioplegia 6 mL of additives was added to one liter of patients’ oxygenated blood, for del Nido 25 mL of additives were added to one liter of patients’ oxygenated blood.
Warm induction was used in patients who were actively ischemic. Cardioplegia was delivered in both antegrade and retrograde directions. The amount delivered was based on patients’ weight and surgeon preference but the initial dose was generally around 1500 mL. The rate of delivery for antegrade was 250–400 mL/min keeping the cardiplegia line of pressure in the aortic root around 200 mm Hg. Retrograde cardioplegia was administered at 200–300 mL/minute keeping coronary sinus pressure around 40–45 mm Hg. Mild systemic hypothermia (32–33 °C) and topical hypothermia were used in all cases. Repeat doses of conventional cardioplegia were given retrograde and down the vein grafts every fifteen to twenty minutes. For del Nido repeat doses were planned at 60 min from the initial dose if the anticipated cross-clamp time was greater than 90 min. A warm dose of blood (‘hot shot’) was given through the coronary sinus or aortic root as well as 100 mg lidocaine, 2 gm Magnesium and 12.5 g Mannitol (del Nido only) which were given directly into the pump reservoir at the end of the ischemic interval prior to removing the cross-clamp.
Follow-upPatients were admitted to the ICU and down-graded to a telemetry unit when they were weaned from mechanical ventilation, off inotropic and pressor support, and had central venous and arterial lines removed. When standard criteria were met patients were discharged on aspirin, beta blockers and statins. Long-acting calcium channel blockers were also given in patients who had radial artery conduits. All patients were followed up at thirty days with a phone call.
Statistical analysisDescriptive statistics were used to summarize demographics and pre- and postoperative variables. If a variable was normally distributed and continuous, the mean ± standard deviation was used; otherwise, median [interquartile range] was used. All the continuous univariate analyses were completed using a 2-sample t test or a Wilcoxon rank-sum test depending on if normality assumption was met and the categorical analysis with Chi squared unless the cells with expected counts less than 5 exceeded 20% then Fisher exact test was used. p values < 0.05 were considered statistically significant.
留言 (0)