
Remember me
We present a case of 46-year-old male with no pertinent past medical history who presented to the emergency department with ongoing chest pain for 9 days associated with intermittent fevers and shortness of breath. On examination, the patient had a heart rate of 88 beats per minute and blood pressure of 143/72 mmHg. There were no audible murmurs or rubs on auscultation. He endorsed ongoing chest pain and shortness of breath.
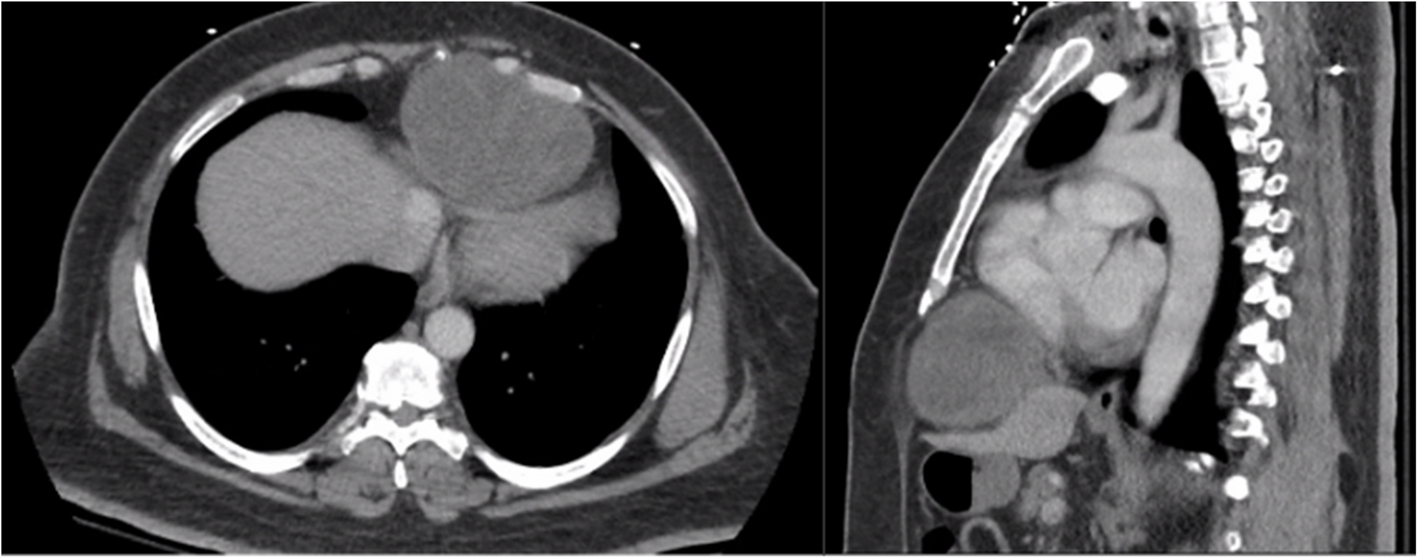
The patient underwent contrast computed tomography (CT) angiography pulmonary embolism with pulmonary arterial phase timing that showed no evidence of pulmonary embolism, but demonstrated a moderate sized pericardial effusion with high density concerning for hemopericardium, along with an outpouching on the right atrial wall with a narrow neck concerning for a pseudoaneurysm (Fig. 1). Further workup, including lab work and an electrocardiogram, were unremarkable. Transesophageal echocardiogram (TEE) redemonstrated the pericardial effusion and right atrial pseudoaneurysm (Fig. 2).
Fig. 1
Computed tomography angiogram of the chest. Computed tomography angiogram showing a right atrial pseudoaneurysm. Neck of the pseudoaneurysm is shown by the green arrow. Attenuation of the pericardial fluid was 28.4 Hounsfield units
Fig. 2
Transesophageal echocardiogram of pseudoaneurysm. Pseudoaneurysm with pericardial effusion redemonstrated on transesophageal echocardiogram arising from right atrium
The case was discussed at the multidisciplinary cardiac conference and the decision was made to take the patient to the operating room given his ongoing symptoms as well as concern for hemopericardium and rupture of pseudoaneurysm into the pericardial space. Cardiac magnetic resonance imaging (MRI) and positron emission tomography (PET) CT were not performed given time-sensitive nature of the case and the desire for tissue diagnosis. The operation was performed via median sternotomy with cardiopulmonary bypass. A pericardial effusion and dense pericardial adhesions were found intraoperatively. After meticulous lysis of adhesions, central cannulation was performed, and the aorta and right atrium were cannulated. Right atrial pseudoaneurysm was identified (Fig. 3) and excised with the surrounding atrial wall. The defect in the atrial wall was closed using a bovine pericardial patch. Full exploration of the chest revealed no other lesions. The resected specimen was sent for pathology to try to establish tissue diagnosis and the patient was closed. The patient’s post-operative course was unremarkable, and he was discharged home on post operative day 4. Operative cultures showed no growth. Pericardial fluid cytopathology demonstrated abundant mixed inflammation with eosinophils, reactive mesothelial cells, histiocytes, and lymphocytes, with no malignant neoplasm identified. Tissue histopathology demonstrated granulation tissue, perivascular lymphocyte infiltrate, dense fibrous tissue, focal calcification, and organizing fibrin thrombus, but no evidence of malignancy.
Fig. 3
Intra-operative photos of pseudoaneurysm. Pseudoaneurysm demonstrated by green arrow. A Blue arrow indicates pseudoaneurysm. B Green arrow indicates bovine pericardial patch used to repair defect in atrial wall after pseudoaneurysm resection
Six weeks postoperatively, the patient presented to emergency department with chest pain, new word finding difficulty, clumsiness, gait instability, and intermittent low-grade fevers. A CT chest scan showed multiple halo-like solid lung, pericardial, and bone nodules (Fig. 4A, B). The CT head scan showed 1–1.5 cm left anterior thalamic and left temporal lobe hemorrhagic lesions. Magnetic resonance imaging of the brain demonstrated multiple enhancing lesions in the left temporal lobe, left anterior thalamus, and right parietal lobe (Fig. 4C). Together, the findings were suspicious for hemorrhagic metastasis, invasive fungal infection (such as invasive aspergillosis), or septic emboli. Given the concern for metastatic process, a biopsy of a lung nodule was performed and showed focal organizing exudative and fibrotic pneumonia negative for carcinoma. A lumbar puncture was also performed and showed no malignant neoplasm. Given the repeated surgical specimens that were negative for malignancy, an extensive infectious and rheumatologic workup was pursued. He was discharged with outpatient infectious disease follow-up, as the most likely diagnosis on the differential was thought to be invasive fungal infection and cultures would take several weeks to result.
Fig. 4
Imaging findings on representation. A Computed tomography (CT) of chest showing multiple lung nodules (green arrows). B CT of chest showing nodular appearance of pericardial effusion and outpouching of the right atrium. C Head magnetic resonance imaging (MRI) demonstrating peripherally enhancing lesions (red arrow)
He represented one week later with returned right-sided chest pain, intermittent headaches, and abdominal pain. Repeat CT scan demonstrated increased number of pulmonary and pericardial nodules. Given the patient’s diagnostic dilemma and ongoing symptoms, a cardiophrenic nodule was biopsied with image guidance. Pathology demonstrated atypical cells, anaplasia, and poorly-formed vascular lumina, suggestive of angiosarcoma (Fig. 5).
Fig. 5
Pathology findings demonstrating angiosarcoma. A low power magnification (× 12.5) hematoxylin and eosin staining of pseudoaneurysm reveals fibrin and organizing hematoma with a variably cellular fibrous cyst wall. B High power magnification (× 400) of pseudoaneurysm reveals scattered enlarged pleomorphic tumor cells with rare atypical mitoses in the background of abundant reactive granulation tissue. C Cardiophrenic nodule (× 400) shows similar atypical cells with unequivocal anaplasia and poorly-formed vascular lumina. D Cardiophrenic nodule (× 400) shows malignant endothelial cells with endothelial hobnailing into the vascular lumen
The patient’s tissue biopsy from his initial right atrial pseudoaneurysm resection was retrospectively reviewed and similar atypical cells were noted in the background of granulation tissue and organizing thrombus (Fig. 5). A diagnosis of primary cardiac angiosarcoma was made. The patient is currently undergoing chemotherapy with weekly paclitaxel for metastatic cardiac angiosarcoma.
Comments (0)