
記住我
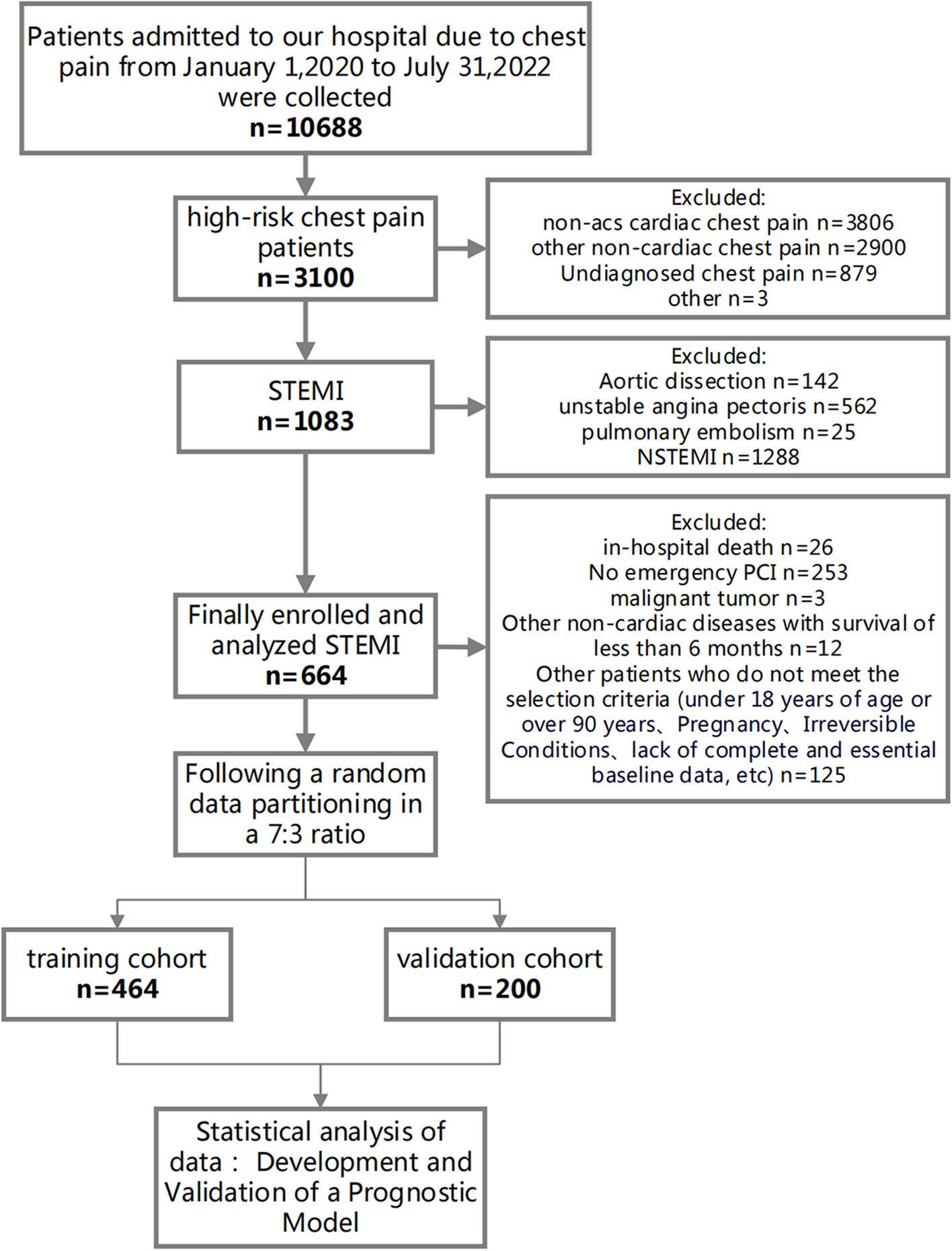





Databases were searched and total number of studies is 76 before May 2022. After removing 6 duplicate articles, we carefully read the remaining 70 articles. Then, 35 articles were excluded due to article type that did not meet our inclusion criteria. Subsequently, after a detailed reading of the remaining 35 papers, combined with our inclusion and exclusion criteria, 20 papers were finally excluded. In our meta-analysis, we finally included 7 retrospective articles that met our criteria for the study rigorously (Fig. 1).
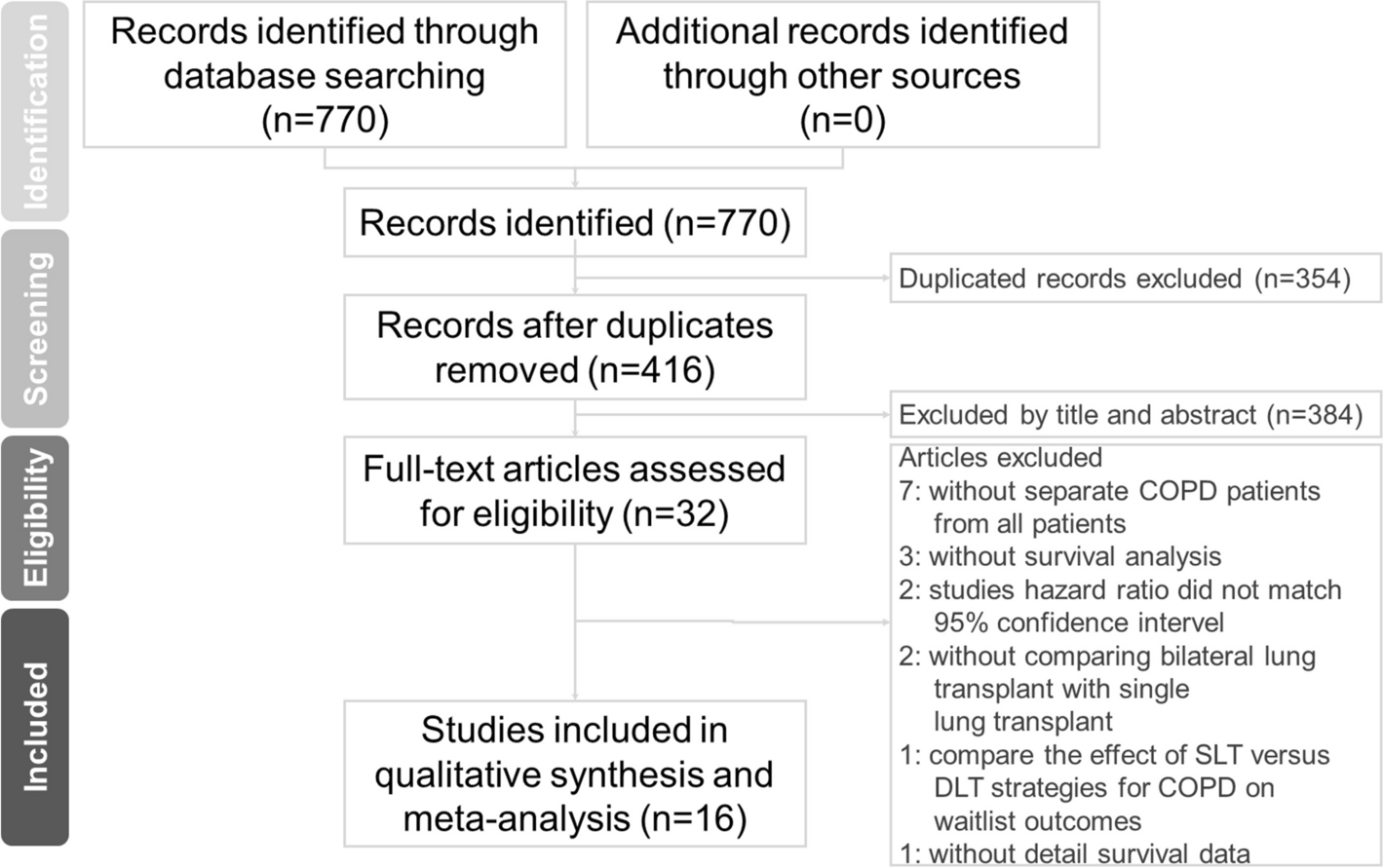
Fig. 1
Flow chart of literature search strategies
The characteristics of included studiesA prospective study was completed by Dong et al. [9]. The results were primarily analyzed for length of hospital stay, hospitalization costs and complications. Patel et al. [4] analyzed the outcomes of patients who were discharged on postoperative day 1 (POD1) with normal approach group. Drawbert et al. [2] summarized patients with stage I non-small cell lung cancer (NSCLC) from 2010 to 2015 and research objects including two groups. In Linden et al. [7] study, they found that carefully selected patients before the surgery may not increase risk of readmission or death. In Dong et al. [6] research, 353 patients were included with 136 persons in the day surgery group and 217 people in the inpatient surgery group. Towe et al. [8] reported that POD 1 discharge patients after lung resection is safe. Geraci et al. [10] evaluated safety for patients discharged by POD1 after different range resection of lobe.
The age between two groupsAge of patients was reported in all studies. The combined data revealed that the age in Day surgery group (DG) was younger than in inpatient surgery group, or named Normal surgery group (NG) (WMD = − 1.32, 95% CI − 2.17 to − 0.48, P = 0.002, I2 = 96%). (Fig. 2A).
Fig. 2
Forest plot of the meta-analysis. A Age. B smoking status of patient. C FEV1% predicted. D DLCO% predicted
The smoking status of patient between two groupsBriefly, four studies reported smoking status of patients between two groups. It revealed that the patients with smoking status in day surgery group were less than in normal group (OR 0.76, 95% CI 0.65–0.87, P = 0.0002, I2 = 71%). (Fig. 2B).
The pulmonary function tests between two groupsThe results of 3 studies revealed that the pulmonary function tests in DG were better than in NG, especially in percent of forced expiratory volume in 1 s predicted (FEV1% predicted) (WMD = 6.02, 95% CI 1.48–10.57, P = 0.009, I2 = 98%) and percent of diffusing capacity of the lung for carbon monoxide predicted (DLCO% predicted) (WMD = 6.00, 95% CI 1.45–10.55, P = 0.009, I2 = 95%). (Fig. 2C, D).
The comorbidity before the surgery between two groupsThe data regarding the preoperative comorbidity were reported in most of studies. The result showed that patients in day surgery were less likely to have hypertension, coronary heart disease, and chronic obstructive pulmonary disease (COPD) than in normal group. (Fig. 3A, B, C) But there is no difference in patients with diabetes before the surgery in two groups (OR 0.84, 95% CI 0.66–1.05, P = 0.13, I2 = 61%). (Fig. 3D).
Fig. 3
Forest plot of the meta-analysis. A Hypertension. B Coronary heart disease. C COPD. D Diabetes
The surgical methods between two groups4 researches reported the surgical method by open access in two groups and the result revealed that open access in DG was less than in NG (OR 0.55, 95% CI 0.51–0.59, P < 0.00001, I2 = 100%) (Fig. 4A). However, it showed minimally invasive surgical method was more popular in DG than in NG (OR 1.74, 95% CI 1.63–1.87, P < 0.00001, I2 = 99%) (Fig. 4B).
Fig. 4
Funnel plot of the meta-analysis. A Surgical method by open access. B Surgical method by VATS. C Lobectomy. D Segmentectomy
The resection range of lobe between two groupsLobectomy or segmentectomy was informed in 4 studies. The pooled data revealed that the lobectomy in DG was less than in NG (Fig. 4C), but segmentectomy in DG was more than in NG (OR 1.90, 95% CI 1.69–2.13, P < 0.00001, I2 = 62%) (Fig. 4D).
The operation time between two groupsResults of 5 studies showed that the operative time was shorter in day surgery group than in normal group (WMD = − 28.54, 95% CI − 39.28 to − 17.80, P < 0.00001, I2 = 99%). (Fig. 5A).
Fig. 5
Funnel plot of the meta-analysis. A Operative time. B Average hospital cost. C 30-day readmission. D 30-day mortality
The average hospital cost between two groupsAccording the result of 2 studies, the average hospital cost in DG was lower than in normal group (WMD = − 1.15, 95% CI − 1.76 to − 0.54, P = 0.0002, I2 = 69%). (Fig. 5B).
The 30-day readmission between two groupsResults of 5 studies showed that there was no difference between two groups in 30-day readmission (OR 0.93, 95% CI 0.63–1.38, P = 0.72, I2 = 81%). (Fig. 5C).
The 30-day mortality between two groupsThe 30-day mortality was lower in DG than in NG according to the result of 3 studies (OR 1.90, 95% CI 1.39–2.58, P < 0.0001, I2 = 63%). (Fig. 5D).
The postoperative complications between two groupsPostoperative complications of surgery patients was reported in 5 studies. The results showed that the postoperative complications in day surgery group was lower than in inpatient surgery group (OR 0.20, 95% CI 0.16–0.24, P < 0.00001, I2 = 91%) (Fig. 6A). From the Fig. 6B–F, in DG, it showed that postoperative complications including hydrothorax, hemorrhage, arrhythmia, lung infection and persist air leak were less than in NG. However, there is no statistical difference between two groups in pneumothorax, chylothorax and hoarseness (Fig. 7A, C).
Fig. 6
Funnel plot of the meta-analysis. A Postoperative complications. B Hydrothorax. C Hemorrhage. D Arrhythmia. E Lung infection. F Persist air leak
Fig. 7
Funnel plot of the meta-analysis. A Pneumothorax. B Chylothorax. C Hoarseness
留言 (0)