
記住我


The patient was a 39-year-old male. He noticed heartburn and dysphagia 11 months before eventual referral to our hospital. The symptoms persisted, and he, therefore, consulted his local doctor 6 months later, and underwent an upper gastrointestinal endoscopy, which revealed Barrett's esophagus and adenocarcinoma of the esophagus. After starting proton pump inhibitor (PPI) treatment, he was referred to his previous hospital for esophageal cancer treatment. Since he was judged to be ineligible for surgery due to severe scoliosis and restricted ventilation, he received curative-intent chemoradiotherapy (4 courses of CF [cisplatin and fluorouracil] with radiotherapy [61.2 Gy/34 fractions]) (Fig. 1). After the treatment, he was referred to our hospital for a second opinion regarding additional treatment due to evidence of remnant cancer.
Fig. 1
Radiation dose distribution maps: radiation was administered to the upper (a, b), middle (c), and lower thoracic esophagus (d), where the tumor was located before the intervention. A total of 61.2 Gy of radiation was administered, with up to 41.4 Gy/23 Fr irradiated to the area, including prophylactic irradiation, and the subsequent 19.8 Gy/11 Fr targeted to the tumor
Medical history: paraplegia in both lower limbs, spinal cord tumor (at age 4).
Family history: none noted.
Physique on admission: height 141 cm, weight 38.3 kg, body mass index 19.3.
Respiratory function test: Before chemoradiotherapy, vital capacity (VC) 1.54 l, %VC 48.6%, forced expiratory volume in 1 s (FEV1.0) 1.46 l, FEV1.0% 94.8%; after chemoradiotherapy, VC 1.51 l, %VC 47.2%, FEV1.0 1.32 l, FEV1.0% 87.4%.
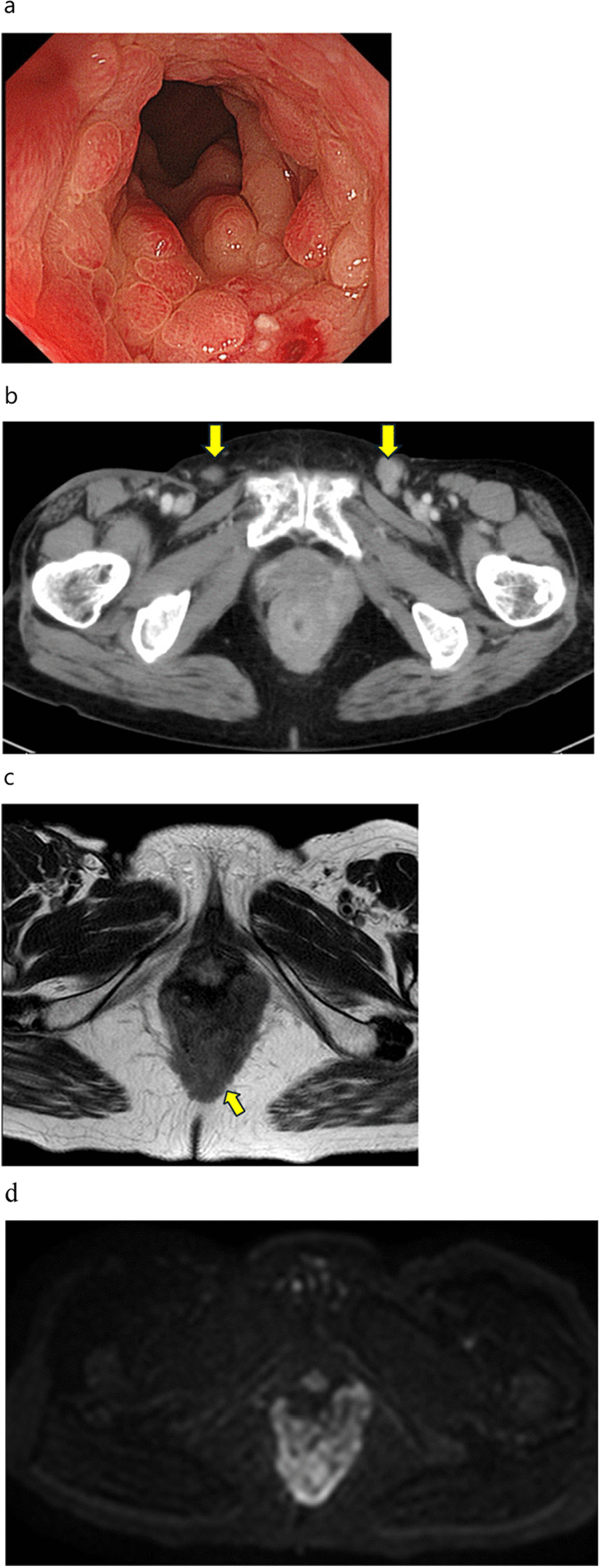
Upper gastrointestinal endoscopy: Before chemoradiotherapy, the squamocolumnar junction (SCJ) was observed 20 cm from the incisors. A marking clip was placed at the same site. Circumferential mucosal irregularity and stenosis were observed between 22 and 29 cm from the incisors. The esophagogastric junction was identified 35 cm from the incisors. The lesion was biopsied and diagnosed as adenocarcinoma. After chemoradiotherapy, the SCJ was found 3 cm distal from the marking clip, suggesting that Barrett's esophagus had regressed due to chemoradiotherapy and PPI treatment. The residual tumor was observed 24 cm from the incisors (Fig. 2).
Fig. 2
Upper gastrointestinal endoscopy images: a Before chemoradiotherapy, the SCJ was observed 20 cm from the incisors (arrowheads). A marking clip was placed at the same site. b Circumferential mucosal irregularity and stenosis were observed between 22 and 29 cm from the incisors. c After chemoradiotherapy, the SCJ was identified 3 cm distal from the marking clip (arrows). d Residual tumor was observed 24 cm from the incisors
Contrast-enhanced CT of the abdomen: The patient had severe scoliosis. The spinal curve was convex to the right at the level of the middle thoracic esophagus, and convex to the left at the level of the lower esophagus, with Cobb angles of 125° and 165°, respectively (Fig. 3). Before chemoradiotherapy, there was thickening of the esophageal wall from the upper to middle thoracic esophagus. There were enlarged lymph nodes around the right recurrent nerve. After chemoradiotherapy, CT showed reduced wall thickening and no enlarged lymph nodes (Fig. 4).
Fig. 3
The patient had severe scoliosis. The spinal curve was convex to the right at the level of the middle thoracic esophagus, and convex to the left at the level of the lower esophagus, with Cobb angles of 125° and 165°, respectively (a, b). 3D-CT image of the spine and ribs shows the narrowing of the rib cage (c)
Fig. 4
Contrast-enhanced CT images: a Before chemoradiotherapy, there was thickening of the esophageal wall from the upper to middle thoracic esophagus, and enlarged lymph nodes were present around the right recurrent nerve (arrow). b After chemoradiotherapy, CT showed reduced esophageal wall thickening with no enlarged lymph nodes
Positron emission tomography–CT: Before chemoradiotherapy, abnormal accumulation of 18F-fluorodeoxyglucose (18F-FDG) was seen from the upper to middle thoracic esophagus, with a maximum standardized uptake value (SUV) of 11.9. Mildly abnormal accumulation was also seen in the lymph nodes around the right recurrent nerve. After chemoradiotherapy, abnormal accumulation of 18F-FDG remained only in the middle thoracic esophagus, with an SUV max of 3.87. The abnormal accumulation in the lymph nodes around the right recurrent nerve had disappeared. No other abnormal accumulation was observed (Fig. 5).
Fig. 5
PET–CT images: a Before chemoradiotherapy, abnormal 18F-FDG accumulation was seen from the upper to middle thoracic esophagus, with an SUV max of 11.9. Mildly abnormal 18F-FDG accumulation was also seen in the lymph nodes around the right recurrent nerve. b After chemoradiotherapy, abnormal 18F-FDG accumulation remained only in the middle thoracic esophagus, with an SUV max of 3.87. Abnormal 18F-FDG accumulation in the lymph nodes had disappeared
Surgical findings: The patient underwent thoracoscopic subtotal esophagectomy involving gastric tube creation by hand-assisted laparoscopy with a flexible endoscope, followed by reconstruction with a narrow gastric tube via the anterior chest wall, and finally gastrostomy. Due to the minimal space in the thoracic cavity, there were few positions for port insertion. We selected the sixth intercostal posterior axillary line as the location for insertion of the first port. We subsequently inserted three ports as marked in Fig. 6 and performed the surgical operation with four ports, one port less than usual. There was marked tissue fibrosis in the upper mediastinal area, especially on the right side, which was thought to represent the effects of chemoradiotherapy on the tumor. Left upper mediastinal lymph node dissection was omitted to preserve vocal cord function. To determine the incision line, the esophagus was partially opened and we checked the clip placed at the location of the SCJ before chemoradiotherapy, and chose the slightly oral-side line from the clip as the oral incision line. Although the free space in both the thorax and abdomen was narrow due to scoliosis, and the convex curve of the thoracolumbar spine somewhat hindered visualization and manipulation, the surgery could be completed using the normal procedure (Fig. 6). The operative time was 6 h and 17 min, and blood loss was 70 ml.
Fig. 6
Intraoperative images: a Thoracic procedure was performed with the patient in the left lower semi-prone position. We selected the sixth intercostal posterior axillary line as the location for insertion of the first port and subsequently inserted three ports as marked. b Thoracoscopic view of the lower mediastinum. c There was marked tissue fibrosis in upper mediastinal area, especially on the right side, which was thought to be caused by the effects of chemoradiotherapy on the tumor. d Free space was narrow, and forceps operation was limited by the convex curve of the thoracolumbar spine when dissecting the lower thoracic esophagus
Postoperative course: In addition to a postoperative intravenous drip, enteral nutrition was administered through the gastrostomy. One week after surgery, an otolaryngologist confirmed that swallowing function was normal. A few days after oral intake was started, the patient required fasting and administration of antimicrobials for 8 days due to increased inflammation, which was thought to be caused by aspiration due to reflux. This treatment resulted in resolution of the inflammation, and the patient’s progress was good after resumption of oral intake. He was discharged home approximately 4 weeks after surgery. The postoperative pathological diagnosis was pT3N2M0 Stage IIIB as defined by the eighth edition of the Union for International Cancer Control (UICC) tumor-node-metastasis classification scheme, and the patient is scheduled to receive postoperative chemotherapy at the previous hospital.
Pathologic examination: Well-differentiated adenocarcinoma-like tumor cells infiltrated the outer membrane with a depth of T3, and tumor cells were scattered in the deep area near the oral margin (Fig. 7). True oral margins were difficult to assess. The distal margin was negative. The chemotherapy response was Grade 1b as defined by the Japanese Classification of Esophageal Cancer (12th Edition). Three lymph node metastases were observed (#105, #106recR, #109L).
Fig. 7
Histopathology images: tumor cells were scattered in the deep area near the oral margin. No cancer cells are seen in the squamous epithelium covering the superficial layer, suggesting that squamous re-epithelialization has occurred over the lesion
留言 (0)