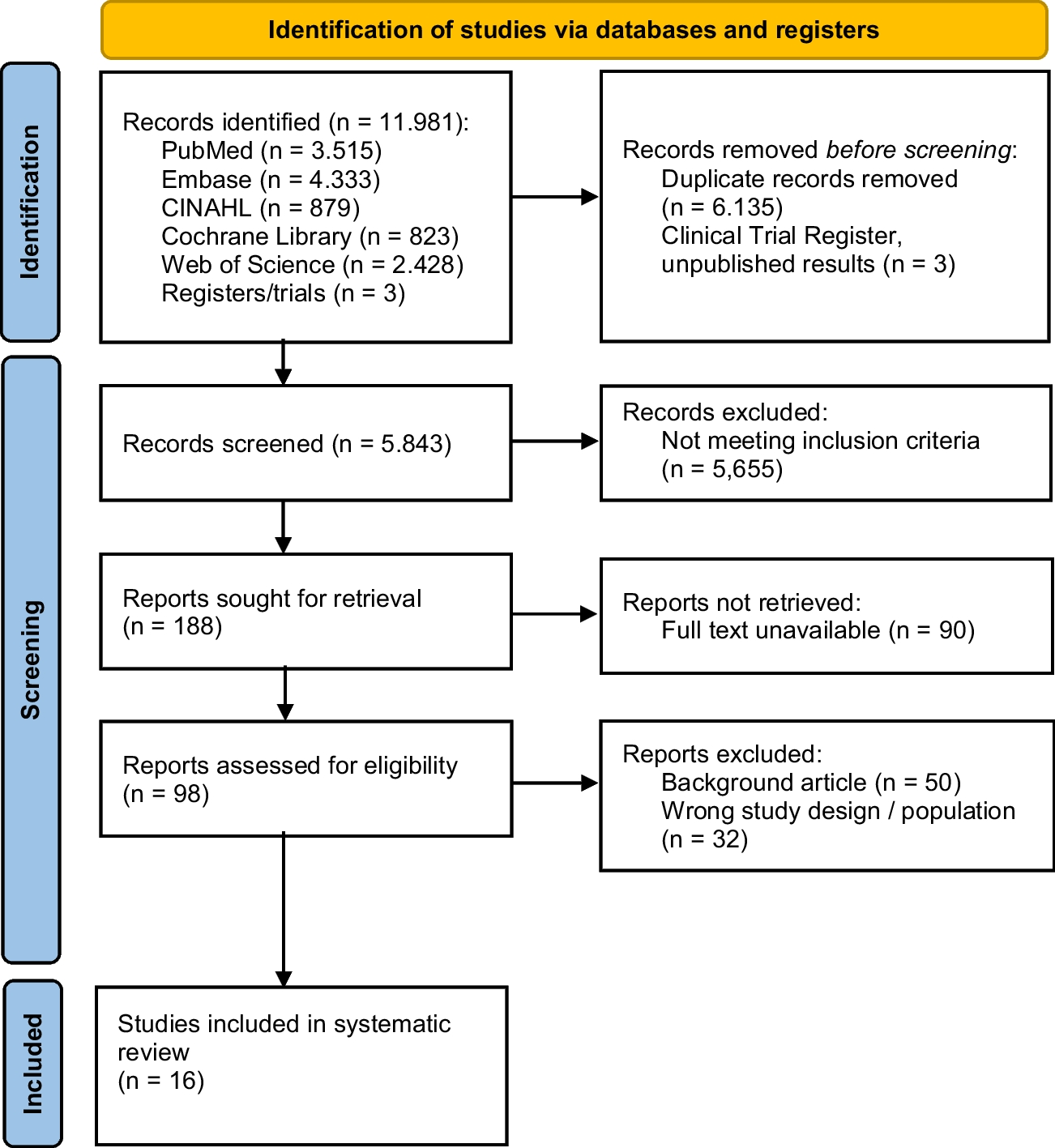
We included more and newer studies [22, 29,30,31, 34, 40,41,42,43] for this meta-analysis and systematic review, 20 observational studies and 3 RCTs. According to our latest findings, the SP group performed better in entrance alignment and intraoperative fluoroscopy time, and had significantly superior Lymsholm scores and anterior knee VAS scores to the IP group, while we did not find similar results in terms of operative time and intraoperative blood loss.
The SP approach has attracted a lot of attention from scholars in the intraoperative and postoperative conditions. In two meta-analyses published in 2018, the results showed the superiority of the SP group over the IP group in terms of intraoperative blood loss, ROM, VAS, Lysholm, and fluoroscopy time. The authors acknowledged the need for more other high-quality RCTs to confirm these findings [9,10,11,12]. In 2021, Packer [13] found differences between the two approaches in Lysholm scores, fluoroscopy time, and entrance alignment in a meta-analysis including 12 studies, while the differences in complications and intraoperative blood loss were not significant. However, Ponugoti [14] found in his meta-analysis that the two approaches differed only in VAS and Lysholm, while there were no significant differences in operative time, fluoroscopy time, deep infection rate, bone nonunion, or secondary procedures. In addition to pain, Lysholm's ratings include instability, thigh muscle atrophy, swelling, and lameness. Despite the correlation between Lysholm and VAS, due to the higher level of heterogeneity resulting from variability in follow-up time, the author stated that their long-term results still need to be confirmed and evaluated in further studies. Sepehri [15] found in a recent meta-analysis that the SP group performed better in Lysholm and intraoperative fluoroscopy time, but showed no such differences in operative time.
The alignment of the entry point is a parameter that is often overlooked by researchers, yet it is equally influenced by the approach. First, mechanically, since the SP approach avoids patellar obstruction, the inserted guide pin easily finds a satisfactory angle while providing a narrow safe entry point for the intramedullary nail to ensure a satisfactory distance deviation [25]; in fluoroscopic slice position, the entry point of the sagittal plane can be clearly confirmed to be located at the junction between the anterior cortex and the articular surface in the tibial plane [43] and therefore did not show any correlation with the two entry points. This may explain the better performance of the entrance point in the coronal plane in terms of accuracy.
In addition, Anderson [23] found that in terms of distance, the accuracy of the entry point in the coronal plane was significantly better than in the sagittal plane, which was similar to our analysis. In cadaveric studies, Franke [17] found that when using the SP approach in the procedure, a more parallel insertion angle to the longitudinal axis was obtained. Thus, both the risk of iatrogenic fracture of the posterior cortex and implant protrusion can be reduced. Therefore, it is reasonable to believe that the suprapatellar approach can help the surgeon to obtain better accuracy in angles and distances in the coronal plane.
According to the accuracy of the achieved reposition, Avilucea [20] reported primary angular disorders in 35 (26.1%) patients in the SP group and 5(3.8%) patients in the SP group (p < 0.0001). For valgus and recurvatum, SP performed better than IP. Moreover, Matthew [42] reported that 11 (15%) patients in the SP group had alignment of > 5 degrees from ideal, compared to 17 (33%) patients in the IP group. Gao [41] reported that 3 (4.3%) patients in the SP group and 15 (23.8%) patients in the IP group had poor fracture reduction. Although this seems to indicate that SP has better reduction results, the data are almost exclusively from distal tibial fractures, and the difference between fracture reduction in the middle and proximal tibia remains to be studied more.
Both Chan [28] and Courtney [21] reported one case requiring return to the operating room for exchange intramedullary nailing due to nonunion in the SP group. MacDonald [24] reported 11 further procedure cases in the SP group, in which 6 involved removal of distal locking screws and 5 involved removal of proximal locking screws. These number are three and one in the IP group. Sun [26] reported seven cases of implant loosening, 4(4%) in the SP and three (5%) in IP; they all led to bone nonunion and IMN revision. However, there were no significant differences in the major complication rate that induced revision or implant removal between the two groups. None of our current study included skin incision infections and deep infections, as these are influenced by multiple factors. Also, open fractures were not included in our study because of the high incidence of sepsis [46]. Therefore, the available findings suggest that although the SP group outperformed the IP group in terms of reposition accuracy and remaining malposition, the superiority in the subsequent need for revision may be challenged.
In the analysis of the fluoroscopy time, the SP group took less time than the IP group and the statistical results were discrepant. In the infrapatellar approach, the knee is placed in a hyper-flexed position on the fluoroscopic triangle device, whereas in the suprapatellar approach the semi-extended position of the knee (15–20°) not only facilitates the repositioning, but also allows for a shorter and easier fluoroscopy condition [6]. Moreover, the fluoroscopy time required by itself is substantially reduced due to the easier positioning of the intramedullary nail entry point under the SP approach. Correspondingly, the reduction in fluoroscopy time also shortens the operative time. It was worth mentioning that Wilianmson [7] innovatively focused on the data of radiation exposure (cGY/cm2), which was significantly lower in the SP group than in the IP group. Azzawi [29] stated the same conclusion in his study. These suggest that the change in approach will benefit both the surgeons and the patients. In the study of Gao [41], the mean number of fluoroscopy procedures (n) in the SP group was 14.10, significantly lower than that of the IP group at 19.61. Almost all of the studies that included fluoroscopy condition favored the SP group. Therefore, we have reason to believe that fluoroscopy time(s), fluoroscopy number (n), and radiation exposure (cGY/cm2) were significantly lower in the SP group than in the IP group.
There are more clinical evaluations of knee function, and due to limitations in literature screening, we only included in our analysis the Lysholm score [8]. This meta-analysis showed that between the two groups, the SP group had a better Lysholm score. Because pain conditions were also included in the Lysholm score, it had some association with the VAS pain score. The outcome of both groups may depend on intraoperative damage to the patellofemoral joint, saphenous nerve, intramedullary nail protrusion, and local inflammation, although the specific device maximally protects the patellofemoral cartilage and talus [10]. Gelbke [9] showed that SP nail insertion contact pressure was high on the patellofemoral joint, but still lower than the threshold of chondrocyte damage. In addition, Leliveld [35] found that the infrapatellar approach may damage the infrapatellar nerve, thereby causing postoperative knee pain and numbness in patients. Katsoulis [4] reported a 47% rate of knee pain after intramedullary nail fixation; however, there is a lack of data to support whether the SP approach will reduce this.
Most of the Lysholm scores in this meta-analysis were from patients 6 months postoperatively. Meanwhile, at the 12-month follow-up, several studies [22, 28, 41] reported the total knee Lysholm scores were comparable between the two groups. Nevertheless, MacDonald [24] reported significant improvements in SP compared to IP at only 1 year. In addition, Sun [26] found tha Lysholm scores were higher in the SP group at both 6 and 24 months after surgery. At about 30 months of follow-up, Çiçekli [33] did not find a significant difference in Lysholm scores between the two groups. These may suggest that the two approaches are fraught with uncertainty in the long-term prognosis of Lysholm scores, even so, we are still confident in the results of this meta-analysis that they differed significantly at least within 6 months after surgery.
Postoperative anterior knee pain was always unavoidable [18], and the sources of pain include implant protrusion, changed biomechanics. and the injury of intra-articular structures, patellar tendon, fat pad, and infrapatellar branch of the saphenous nerve [19]. Theoretically, the change in approach could effectively circumvent some of these factors. For example, in the suprapatellar approach, precise insertion points can avoid damage to the knee structure. A more parallel insertion angle to the longitudinal axis can avoid implant protrusion and infrapatellar nerve injury. These may explain the association between higher insertion point accuracy and lower VAS scores.
Likewise, most of the VAS scores in this meta-analysis were also from patients 6 months postoperatively. In the long-term prognosis, Sun [26] showed significant difference between the two groups at 12 and 24 months postoperatively; he also reported the conditions at 1and 3 months, but the outcomes were not significant. Lu [43] reported better performance in the SP group at 12 months, though it contradicted the findings of some studies [28, 30, 41].
Although some former studies [25, 28, 36, 37] did not find any difference in VAS scores between SP and IP, more data from the combined meta-analysis still gives us confidence in the results. Considering the high heterogeneity for some results of this meta-analysis, it should be treated with caution, which also means that we need more high-quality studies.
Although our meta-analysis incorporated more recent studies, explored most of the relevant questions, and reached the latest conclusions in the two groups, several potential limitations should be noted: (1) we were unable to include more RCTs in the literature due to the specificity of the study; (2) in the face of high heterogeneity, we were not able to explore their sources; (3) the prognosis of short-term follow-up within 6 months as well as infection, deformity,and bone nonunion was not comprehensive due to literature limitations.




留言 (0)