Protocol and registration
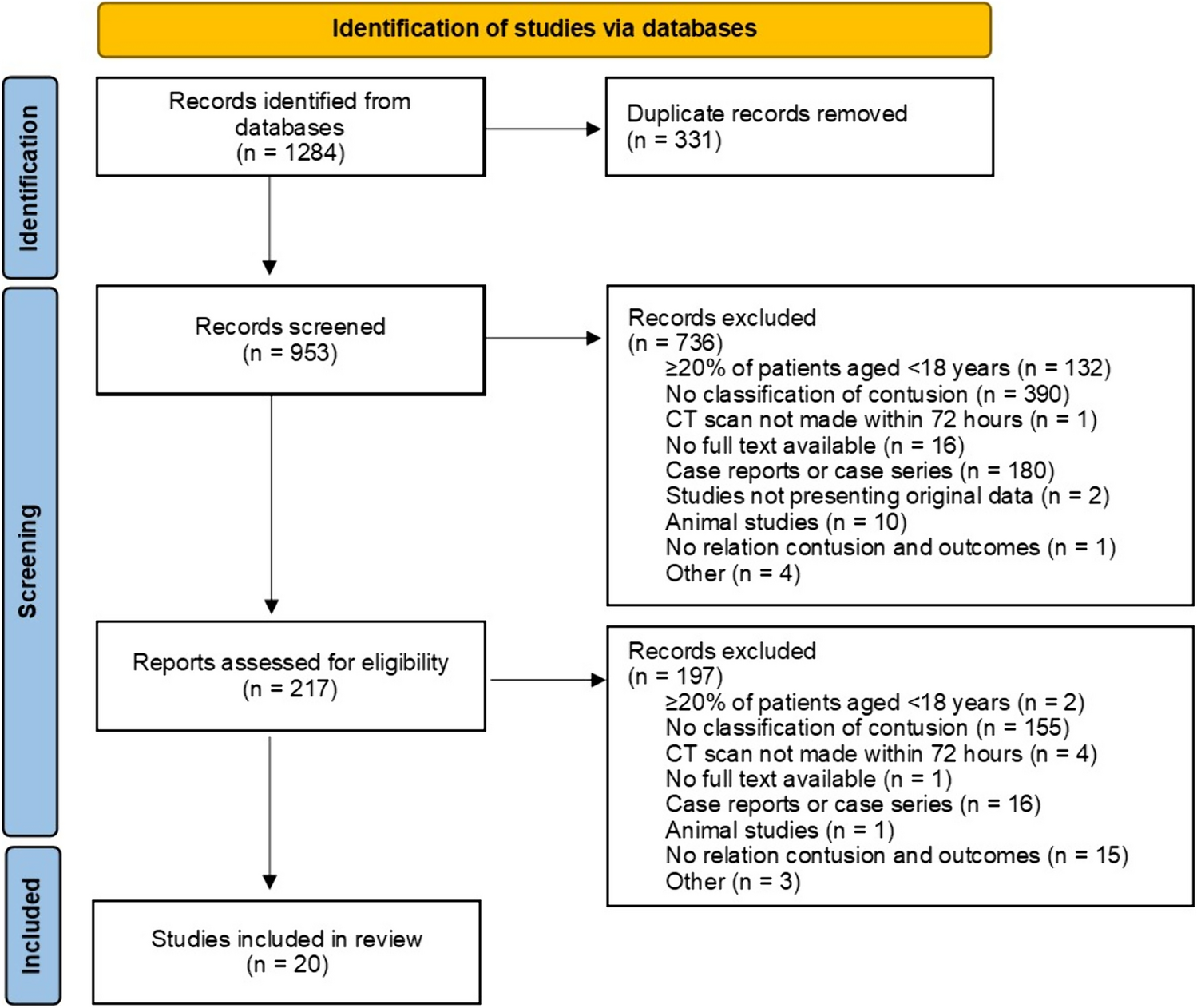
This systematic review was performed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [14]. The registration number in the International Prospective Registration of Systematic Reviews (PROSPERO) is CRD42023417924.
Search strategy
A comprehensive literature search for studies comparing the duration of the conservative treatment of patients with DRFs was performed on January 24th, 2023. The searches were conducted using PubMed, Embase, CINAHL, Cochrane Library, and Web of Science. Index terms were determined for the literature search, and included Medical Subject Headings (MeSH) and closely related words. The following MeSH terms were used: “Radius Fractures,” “Wrist Fractures, “Conservative Treatment,” “Casts Surgical,” and “Splints.” No language or time restrictions were incorporated into the search. Other sources involved the manual screening of reference lists of randomized clinical trials, review articles, and systematic reviews. The Clinical Trial Register was checked for unpublished articles, and their authors were asked to give an update regarding their results. For a full search strategy, see Supplementary 1.
Study selection
The studies retrieved from the searches were imported into Rayyan for Intelligent Systematic Review [15]. After dataset de-duplication, two reviewers (M.B. and L.G.) independently performed title and abstract screening to determine whether each study should be included in this review. Disagreements between the two authors were discussed, and a third reviewer (L.S.) was involved if consensus could not be reached.
Eligibility criteria
All studies, randomized controlled trials (RCT) and otherwise, investigating the duration of conservative treatment for patients with DRFs were eligible for inclusion. The exclusion criteria consisted of (1) studies investigating the operative treatment of patients with DRFs, (2) pediatric patients (age < 18 years), (3) veterinarian studies, (4) the absence of the full text, and (5) case reports, editorials, conference abstracts, and letters to the editor. Studies in languages other than English, Dutch, or German were translated to review the abstracts for eligibility.
Quality assessment
The included articles were assessed for their quality by two reviewers (M.B. and L.G.). The Cochrane Risk of Bias tool 2 (RoB2) was used to assess the risk of bias based on five domains: (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result. The risk of bias was rated as low, some concerns, or high [16]. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the quality of evidence, which was rated as very low, low, moderate, or high [17].
Data extraction
Data extraction was performed independently by two reviewers with the use of a predefined data extraction form. The following characteristics were extracted from the included studies: author, year of publication, study design, number of included patients, follow-up period, non-operative immobilization treatment, reduction or none performed, duration of treatment, and outcome measurements (including wrist function, grip strength, range of motion, pain scores, and radiological outcome).
Analyzed outcome measurements from included articles
Patient-reported outcome measurements
The PROMs were evaluated with the Patient Rated Wrist Evaluation (PRWE); Disabilities of the Arm, Shoulder and Hand (DASH); Gartland and Werley; de Bruijn and the de Bruijn modified, Cooney, Patient-reported Outcome Measurement Information System Pain Interference (PROMIS-PI); and the Mayo Wrist score tools. The PRWE consists of three subscales: pain, function, and cosmetic. Participants are asked to respond to all items using a scale ranging from 0 to 10, with a total score of 100 [18]. The DASH and quick DASH (qDASH) tools assess the functional outcome of the upper extremity on a 5-point scale with 30- or 11-item questionnaires, respectively. Higher overall outcomes on the PRWE and (q-)DASH questionnaires represent a worse functional outcome [19]. The Gartland and Werly score combines subjective and objective items evaluating the wrist and hand function; here, a lower score represents a better functional outcome [20]. The de Bruijn and the modified de Bruijn scoring lists by Christersson et al. [21] evaluate functional outcome; again, a lower outcome represents a better wrist function [22]. The Cooney score assesses the domain’s pain, function, range of motion, and grip strength, with a total score of 100 points. In this score, a higher outcome over all domains represents a better functional outcome [21, 23]. The PROMIS-PI measures the extent to which pain limits a patient’s ability to engage in physical, mental, and social activities, with a lower overall outcome representing less pain interference [24]. Finally, the Mayo Wrist Score represents pain during the active motion of the injured wrist compared to the contralateral wrist and indicates the possibility of resuming daily activities; it is measured on a scale from 0 to 100, where a higher overall outcome represents a better wrist function [25].
Pain scores
Pain scores were either measured using a visual analog scale (VAS) or as a percentage of normal and mild pain.
Grip strength
Grip strength was measured using hand-grip dynamometry. It was expressed as mean grip strength of the injured limb and grip strength of the injured limb as a percentage of the contralateral wrist.
Range of motion
Range of motion was measured by joint extension, flexion, and deviation. It was expressed as degrees of motion, forearm rotation, mean range of motion, mean deviations of the injured wrist expressed as percentages of the uninjured wrist, and as the sum of flexion, extension, and radial and ulnar deviation.
Radiological outcome
Radiological outcome was measured using the Lidström criteria. The results were presented as excellent, good, fair, or poor based on anatomical outcomes expressed as percentages [26]. Measurements of radial and volar angulation in degrees, radial length, and shortening in millimeters were used to determine anatomical differences during treatment.
Statistical analysis
The data were collected and analyzed using the Review Manager software (version 5.3). The protocol and study population were investigated to determine clinical homogeneity. Statistical homogeneity was determined by the use of I2 tests, with values less than 40% considered homogeneous [27]. Funnel plots were generated using Review Manager to determine the publication bias [28].



Comments (0)