Study design and settings
This was a nationwide retrospective cohort study of the impact of doctor cars on in-hospital survival compared with that of a non-physician staffed GEMS for patients with severe trauma with an injury severity score (ISS) of ≥ 16. Anonymized data were collected from the Japan Trauma Data Bank (JTDB), established by The Japanese Association for Acute Medicine and The Japanese Association for the Surgery of Trauma. Overall, 280 major emergency hospitals were included in the JTDB [21].
Patients
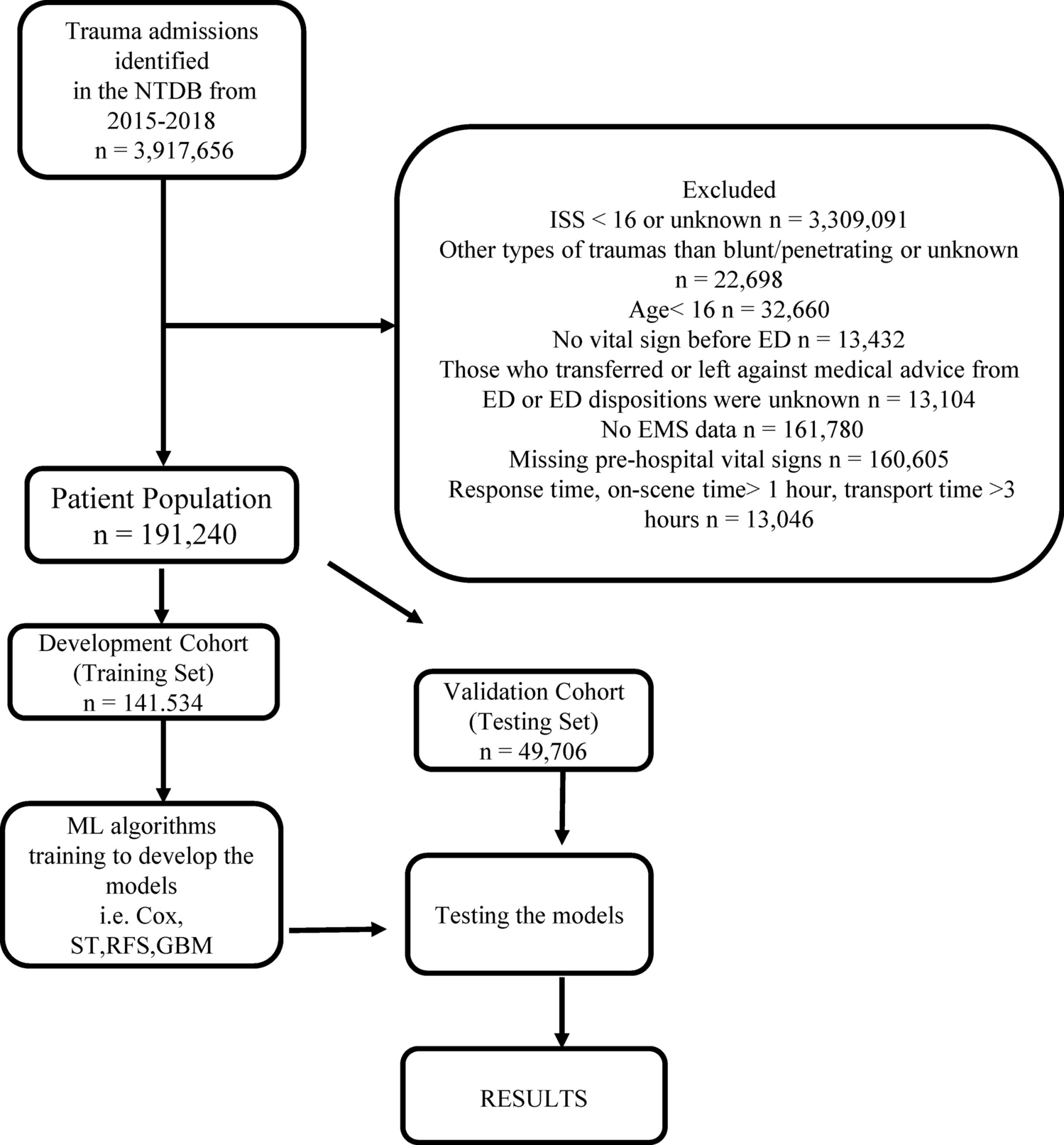
In total, 372,365 patients with trauma were enrolled in the JTDB between April 2009 and March 2019. The inclusion criteria were as follows: (1) ISS ≥ 16, (2) age 15–85 years, (3) a clear injury history, (4) those transported to the hospital from the scene, and (5) a clear means of transport—a doctor car or non-physician staffed GEM [15]. However, the exclusion criteria were as follows: (1) cardiac arrest at the scene (heart rate = 0 was defined as cardiac arrest); (2) Abbreviated injury scale (AIS) = 6 (an unsalvageable condition); and (3) patients with missing variables necessary for analysis.
Exposure
In this study, the exposure group used doctor cars in pre-hospital care. This included conventional high-standard ambulances with a physician on board and passenger car-type emergency vehicles approved for operation in Japan in April 2008, without a bed for patient transport, dispatching a physician and a nurse to the scene.
Control
Non-physician staffed GEMS in pre-hospital trauma care was defined as the control group.
Outcome measures
The outcome was in-hospital survival at discharge.
Variables
We obtained the following information from JTDB: age, sex, pre-hospital vital signs (systolic blood pressure [SBP], respiratory rate [RR], heart rate [HR], and Japan coma scale [JCS]) [26], season, injury year, injury time (day or night), injury day (weekday or holiday), trauma type (blunt or sharp), pre-hospital time course (injury to emergency department arrival), facility, ISS and the highest score of AIS values for each region of the body, and patient survival status at hospital discharge [7, 15, 24, 27]. The days of injury were defined as weekdays and holidays based on the Japanese calendar. This study aimed to investigate the impact of pre-hospital doctor car interventions on outcomes, as in previous reports; therefore, physiological information post-hospital arrival was not included [15].
Statistical analyses
For the baseline characteristics of the patients, categorical and continuous data were expressed as n (%) and mean ± standard deviation (SD), respectively, based on a normal distribution. When data did not follow a normal distribution, continuous data were expressed as medians (interquartile range [IQR]). Patient data were classified into doctor car and non-physician staffed GEMS groups. The chi-squared test, Welch's t-test, and Wilcoxon rank sum test were used to compare categorical, continuous volume, and median [IQR] data, respectively, between groups. The analysis was considered significant if the two-sided p-value was < 0.05. A sample size calculation was not performed. Data were analyzed using SAS version 9.4 statistic software (SAS Institute, Inc., Cary, NC, USA).
This study used multivariable logistic regression analysis with adjustment for covariates to explain the association between outcomes and doctor cars. Generalized estimating equations (GEE) were applied to the logistic model to account for the hierarchical structure of the data collected from multiple facilities, that is, clustering by the hospital [28,29,30]. Covariates included age, sex, injury year, season, injury day, injury time, ISS, pre-hospital vital signs (SBP, RR, HR, and JCS), and pre-hospital time course.
Hospital volume (HV) was defined as the annual number of patients hospitalized with severe trauma (ISS ≥ 16) [24]. Subgroup analyses of the relationship between doctor cars and survival compared with non-physician staffed GEMS were conducted for HV ≥ 50 patients/year and HV < 50 patients/year groups [24].




留言 (0)