Primary cardiac tumors are very rare. The incidence is between 0.0017% and 0.03% in autopsy series. Most primary cardiac tumors are benign, but approximately 25% are malignant [5]. Among primary malignant cardiac neoplasms, approximately 80% are sarcomas. Angiosarcomas are the most common, followed by rhabdomyosarcomas, malignant mesotheliomas, and fibrosarcomas [6].
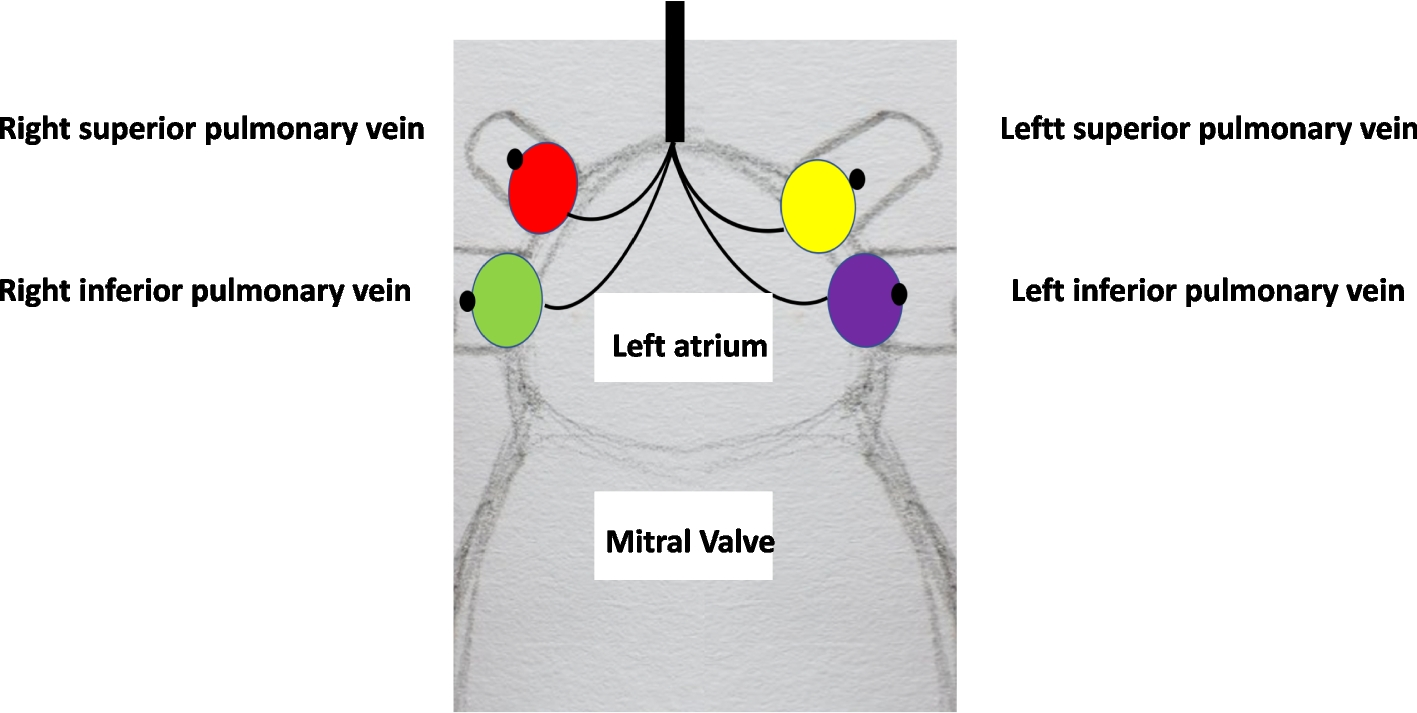
Myxofibrosarcoma is a malignant tumor of mesenchymal origin that most commonly occurs in the extremities of older patients and a primary myxofibrosarcoma rarely arises in the heart [4]. The clinical presentation often varies. Similar to other benign or malignant cardiac tumors, cardiac myxofibrosarcoma presents with symptoms such as dyspnea, chest pain, edema, and syncope. The LA is the most common location of the tumor, followed by the LA + PV, right heart system, and left ventricle [2]. We searched the number of cases of primary cardiac myxofibrosarcoma that have been reported using the Web of Science database, with keywords, “myxofibrosarcoma” and “cardiac.” There were 38 case reports of primary cardiac myxofibrosarcoma, but only one case was reported of a tumor located in the pericardium [7]. Thus, to the best of our knowledge, this is the first case report of primary cardiac myxofibrosarcoma occurring in both the LA and pericardium.
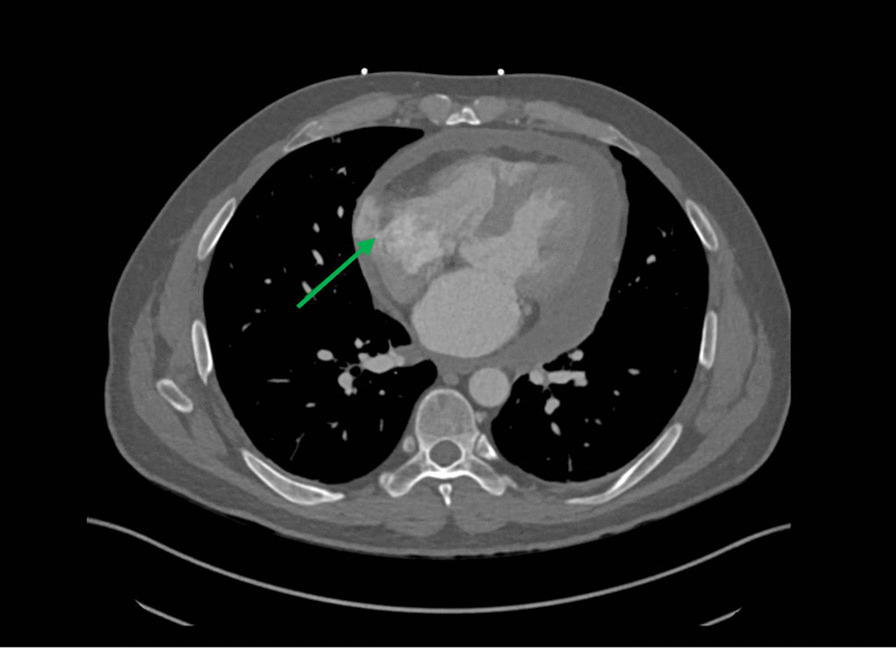
Distinguishing myxoma from myxofibrosarcoma is important because myxoma should be promptly resected to prevent sudden death or embolic event [8]. Currently, cardiac myxofibrosarcoma is difficult to differentiate from myxomas because both tumors are mainly attached to the LA wall [9]. In addition, because the histological types of cardiac tumors vary, characterization of cardiac tumors using imaging techniques has been challenging [9]. In our case, the echocardiogram and CT showed that the tumors were in the LA wall. However, the masses existed in both the LA and pericardium, and the LA mass was extended to the PV. Therefore, the tumors were not considered to be myxoma. MRI showed that both masses had high intensity on T2-weighted sequences and multiple low-intensity zones within the masses on enhancement sequences. John P et al. reported that undifferentiated sarcomas showed high intensity on T2-weighted sequences and heterogeneity on enhancement sequences [8]. Therefore, we assumed that the masses were sarcomas. However, we could not completely rule out the possibility that the tumor was benign, partly because it was mobile. In our case, image modalities showed pericardial fluid. We did not perform pericardiocentesis because hemodynamics was stable, and we planned to attempt tumor resection for preventing sudden death and embolic event regardless of whether the tumors were benign or malignant. Although gaining a definitive diagnosis from only pericardial fluid is difficult, we could gain additional findings which contribute to distinguishing malignancy from the fluid properties or cytological examination. The examination of pericardial fluid would be valuable to evaluate the prognosis.
The median survival time of primary cardiac myxofibrosarcoma patients treated with tumor resection is only 14 months [2]. Although complete surgical resection is important for prolonged survival, it is difficult, and only occurs in one-third of cases [10]. In our case, the masses were expected to be difficult to resect completely. The masses existed not only intracavitary, but also in the pericardium, and the patient was older. Considering these points, there is a treatment option: First, we resect only the pericardial tumor for intraoperative diagnosis. Then, if the tumor is suspected to be benign, complete resection is performed under cardiopulmonary bypass. For this option, if the tumor is suspected to be malignant, we could reduce surgical stress by not resecting the LA mass and gain a definitive diagnosis from the pericardial mass; however, we could not prevent sudden death. We chose the option of resecting both masses under cardiac standstill because we wanted to avoid detaching the LA tumor by cardiac uphold or unexpected arrhythmia at the time of resecting the pericardial tumor. The reason for operating was to prevent sudden death or embolic event from incarceration of the LA mass. Consequently, although we could not complete the resection, we could prevent sudden death or embolic event, as the patient wished. Recently, it has been reported that cryoablation can cause tumor tissue necrosis and apoptosis. Moreover, these effects may prevent the progression of the primary tumor and distant metastasis [11]. Ujihara et al. reported that cryoablation is an effective procedure to resect the non-transmural atrial wall when tumors are resected incompletely [4]. In our case, we should have use cryoablation for the remaining PV tumor.
Myxofibrosarcoma is categorized as a low grade to high grade neoplasm. Low grade myxofibrosarcoma tends to metastasize locally, whereas high grade myxofibrosarcomas invade local and adjacent tissues and are associated with distant metastasis to the lung, bone, brain, and lymph nodes [10]. The local recurrence and distant metastasis rates were 42.9% and 19.0%, respectively [4]. Therefore, if the tumor is a high grade myxofibrosarcoma or cannot be completely removed, additional radiotherapy and chemotherapy should be considered. However, the rarity of this tumor is an obstacle in establishing effective chemotherapy regimens and radiotherapy doses. In our case, although we prevented sudden death or embolic event, the patient died after 3 months because of incomplete surgical resection and not performing early additional radiotherapy and/or chemotherapy.
In summary, we report a rare case of primary cardiac myxofibrosarcoma located not only in the left atrium but also in the pericardium. Distinguishing myxofibrosarcoma from myxoma or other malignant tumors is difficult preoperatively. To decide the best therapeutic course for the individual patient, considering in depth preoperative laboratory findings as many as possible, several options of surgical and adjuvant therapy, and the patient’s wishes are important.






留言 (0)