Participants and procedures
Participants (aged 12–16 years) were recruited via convenient sampling from 14 middle schools in 6 districts in Changsha Hunan Province, China. Students in grades 7 through 9 with parental consents to participate in our study and able to complete all scales and assessments independently were included in the study. Data were collected through a self-administered paper-based questionnaire anonymously. Participants were informed of relevant research information before the survey was started by well-trained psychiatrists. Moreover, we also provided extra mental health support during the survey if they had psychological distress or reported higher suicidal risk. This study was approved by the ethics committee of the Second Xiangya Hospital of Central South University. Written informed consents were obtained from the parents of all the participants.
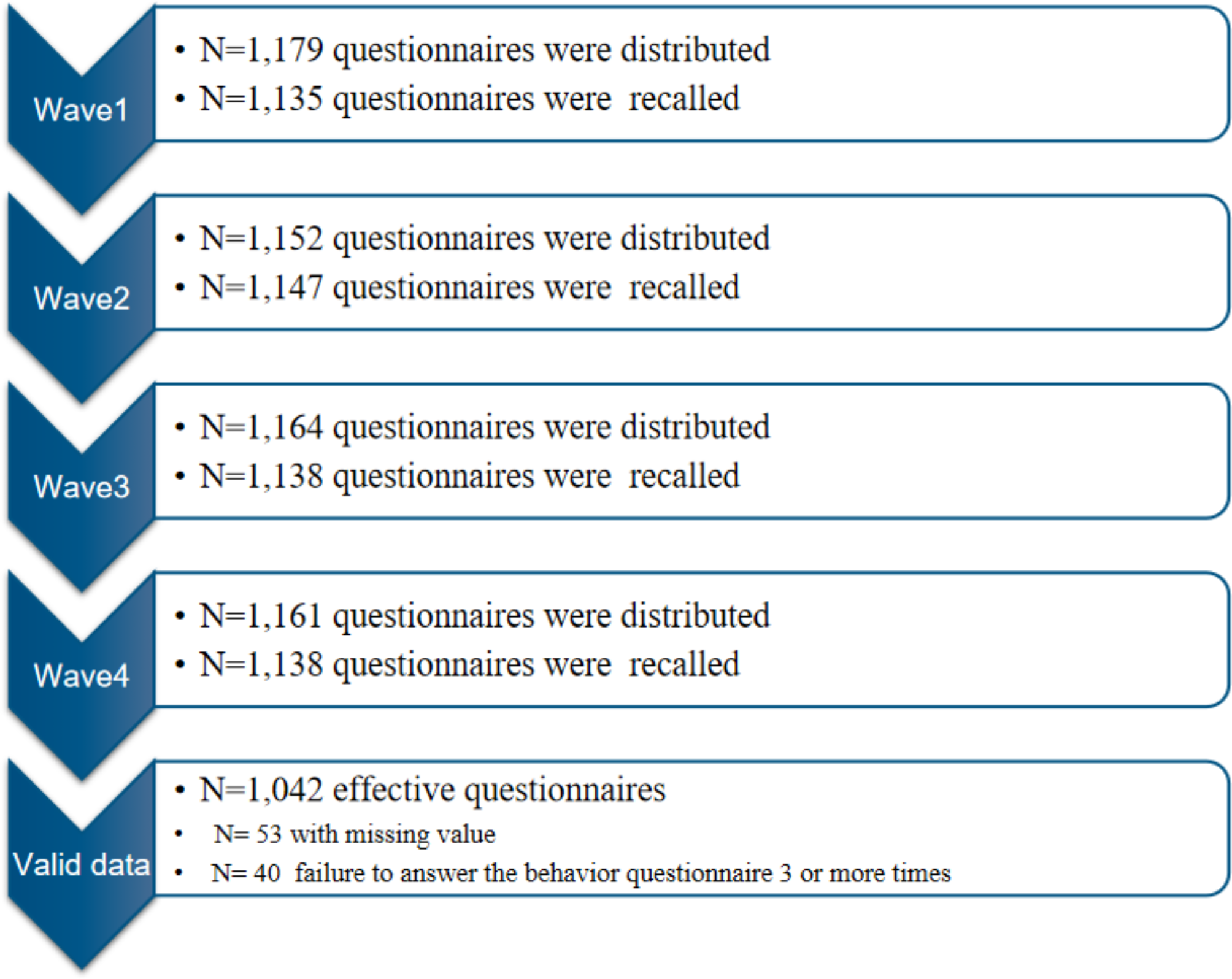
The survey was conducted from February 12, 2021, to May 12, 2021, and in total, 1,501 participants completed the questionnaire survey. All answers were imported manually into the Electronic Data Capture System (EDC) of the Department of Psychiatry at the Second Xiangya Hospital by researchers. Questionnaire responses that had obvious errors were excluded.
MeasuresDemographic characteristics
Basic demographic information, including gender (male/female), age (years), residence (urban/rural), the only child in the family (yes/no), parental education level (Primary school or below/Middle school/High school/Bachelor/Master or above), and monthly household income per capita (estimated by Chinese yuan), were collected.
Parenting styles
Parenting styles were assessed by the short form of Egna Minnen Betraffande Uppfostran (s-EMBU) [23]. Each item in the questionnaire evaluated the perceived parenting styles of the father and mother, respectively. Items were scored by the Likert scale of 1–4 points (1 = “never” to 4 = “always”). The scale consists of three factors, including rejection (item 1,4,7,13,16,21), emotional warmth (item 2,6,12,14,19,23), and overprotection (item 3,5,8,11,17,18, 22). Negative parenting styles include rejection and overprotection from parents, whereas positive parenting styles refer to emotional warmth from parents. The s-EMBU demonstrated satisfactory psychometric properties among Chinese high school teenagers [24]. The s-EMBU also showed good internal consistency in our study with a Cronbach’s Alpha of 0.730 and 0.767 for the father and mother’s parenting styles, respectively.
Proximal psychological factors
Depressive and anxiety symptoms during the past two weeks in adolescents were measured by questionnaires of Patients Health Questionnaire-8 (PHQ-8) [25] and Generalized Anxiety Disorder-7 (GAD-7) [26], respectively. We excluded the item “Thoughts that you would be better off dead, or thoughts of hurting yourself in some way”, given that the last item in PHQ-9 overlapped the suicide measurement adopted in our study. Both PHQ-8 and GAD-7 have shown good reliability and validity in adolescents and college students [27, 28], The Cronbach’s α was 0.855 and 0.916 for PHQ⁃8 and GAD-7 in our study.
Affective lability during the last month was assessed by 18 items of the Affective Lability Scale (ALS-18) [29], which were grouped into three subscales measuring affective transitions from anxiety to depression (item 1,3,5,6,7), depression to elation (item 2,10,12,13,15,16,17,18), and anger (item 4,8,9,11,14), respectively. Each item was rated on a 4-point Likert scale of 0–3 points (0 = “very uncharacteristic of me” to 3 = “very characteristic of me”). A higher score indicates a higher level of affective lability. The Chinese version of ALS-18 demonstrated good psychometric properties among the Chinese student sample [30], This scale was tested to have good reliability in our sample (Cronbach’s α = 0.972).
Rumination during the last month was evaluated by a 10-item Ruminative responses scale (RRS-10) [31]. The scale is scored by summing the responses for each of the ten items, with each item rating from 1 to 4 (1 = “never” to 4 = “always”). A higher score suggests higher levels of rumination. The scale has demonstrated satisfactory psychometric properties among Chinese students [32]. The Cronbach’s α was 0.908 in our study.
Resilience during the last month was assessed using the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) [33]. Items are rated on a 5-point Likert scale (0 = “not true at all” to 4 = “true nearly all of the time”), yielding a total score of 0 to 40. A higher score indicates better resilience. The CD-RISC-10 demonstrated satisfactory psychometric properties among Chinese adolescents [34]. The scale displayed good internal reliability in our sample (Cronbach’s α = 0.929).
Suicidal thoughts
Adolescent suicidal thoughts were measured by the 12-item concise health risk tracking self-report (CHRT-SR) [35] that evaluated a person’s active suicidal thoughts during the past 24 h. The CHRT-SR is composed of three subscales, including hopelessness (item 1, 3, 4, 5, 6, 7, and 8), social support (item 2 and 9), and active suicidal thoughts (item 10, 11, and 12). Given the factor of hopelessness and social support exhibiting high interrelations (Rp > 0.4) that termed “redundant nodes” in network analyses [36], we only included the factor of suicidal thought that assessed the severity of suicidal thoughts in the preceding 24 h. Participants rated each item on a scale from 1 to 5 (1 = “strongly disagree” to 5 = “strongly agree”), with higher values indicating more imminent suicidal risk. The CHRT-SR has demonstrated good internal reliability in adolescents with suicidality [37] and good internal reliability in our sample (Cronbach’s α = 0.923). Details of each questionnaire were provided (see Table S2).
Statistical analysisData description and general differences
Data distribution was examined by probability plot and Kolmogorov-Smirnov test. Descriptive features of continuous variables with normal distribution were presented by mean and standard deviation (SD), non-normal variables by median and interquartile range (IQR), and categorical variables were presented by frequency and percentages. The differences in continuous variables with non-normal distribution between groups were examined by the Mann-Whitney U test on SPSS Version.25.0 software, with a significance threshold set at 0.05.
Adolescent psychosocial network
To show the interrelationships at symptoms levels between parenting styles and proximal psychological risk factors, firstly, we constructed the adolescent psychosocial network consisting of 26 nodes representing the parenting styles for father and mother (i.e., six items for rejection, emotional warmth, and overprotection from father and mother, respectively), emotional symptoms (i.e., eight items of PHQ-8, seven items of GAD-7, and three factors of ALS-18), and two items for rumination and resilience. The network structure was estimated by Gaussian graphical model (GGM) using Extended Bayesian Information Criterion (EBIC) selection via the R package “bootnet’’ and “qgraph” [38]. Specifically, we applied rank transformations (Spearman correlations as input) during the network construction considering the data were skewed [39]. Moreover, we created the layouts for each graph via the Fruchterman-Reinold algorithm [40], which prioritizes the more connected nodes in the center of the network and the less connected ones in the periphery. Before demonstrating network metrics, network accuracy and stability were assessed by bootstrapping procedure via the R package “bootnet’’. In addition, we tested the significance of the edge weights and centrality indices of each node.
Besides, we computed bridge strength in the established network. Bridge strength was calculated to denote the importance of a node to the network, as a recent study indicated that bridge closeness or betweenness may not be directly interpreted in the psychological network [41]. Bridge strength is calculated by the sum of absolute values of the edges connected to a given node to nodes in other symptom clusters, which denotes the importance of the symptom in connection with other symptom clusters [16].
Network associated with suicidal thoughts
To investigate whether the bridge symptoms were correlated with active suicidal thoughts in adolescents, we re-estimated the psychosocial network structure by including a continuous variable that measures active suicidal thoughts in adolescents over the past 24 h.
In light of a previous study reporting that girls who perceived more parent rejection and neglect in childhood tend to exhibit more suicidal attempts than boys [42], we also examined whether the network properties differ by gender. The difference in network properties including global strength, network structure, and edge weights via the R package “Network Comparison Test (NCT) [43]. The p-value was estimated by permutation test in NCT (5000 iteration), and the significance level was set at 0.05, 2-tailed.
Besides, to investigate the influence of demographic covariates on our original symptoms network, we reconstructed the network by including additional demographic factors (e.g., age, sex, residence, educational level, income). Then, the absolute differences in edge weights between the original symptom networks and the re-estimated network termed the “Delta network”, were calculated. The weaker difference in edge weights indicated that the covariates did not significantly affect the network structure.
Linear regression analysis
To further assess the predictive value of the identified bridge symptoms in the psychosocial network for active suicidal thoughts in adolescents, we conducted a linear regression analysis to explore the relationship between the bridge strengths of the psychosocial symptoms and their edge weights connected to active suicidal thoughts. The bridge strengths of each psychosocial symptoms were served as the independent variables and the edge weights connected the psychosocial symptoms to active suicidal thoughts were served as dependent variables. A significant correlation indicates that a node with higher bridge strength may predict higher suicidal thoughts.



Comments (0)